2337
A Reader Study Comparing the Quality of High-Resolution Diffusion Weighted Imaging Methods for Breast MRI1Department of Biomedical Engineering, University of Minnesota, Minneapolis, MN, United States, 2Center for Magnetic Resonance Research, University of Minnesota, Minneapolis, MN, United States, 3Department of Radiology, University of Minnesota, Minneapolis, MN, United States, 4Masonic Cancer Center, University of Minnesota, Minneapolis, MN, United States
Synopsis
Axially reformatted (AR) SMS can provide full-coverage breast DWI with high quality and 1.25 mm isotropic nominal resolution. In this work we assess the image quality of AR-SMS in a clinical setting and compare it with a standard clinical sequence and RS-EPI. Three radiologists scored DWI and ADC maps from 30 patients with enhancing lesions. All three readers scored AR-SMS with the highest quality and ranked it as superior most frequently. Accounting for reader and subject effects, a linear mixed model found that AR-SMS outperformed RS-EPI, which both outperformed the Standard with statistical significance in both quality score and rank.
Introduction
Despite growing interest in diffusion weighted imaging (DWI) for breast cancer imaging, the clinical value of breast DWI has not been realized in part due to the low resolution and artifacts associated with single shot (SS) spin-echo echo planar imaging (SE-EPI). Several alternative strategies have been proposed, including readout-segmented (RS) EPI1,2, simultaneous multislice (SMS) imaging3, RS combined with SMS4, reduced FOV (r-FOV)5,6, multiband encoding in the PE direction combined with r-FOV7 and non-SE-EPI methods8-10. While promising, these methods cannot yet achieve anatomical quality and resolution with full coverage in a clinically acceptable scan time.SMS provides fast encoding of large volumes; previous work has demonstrated that axially reformatted (AR) SMS can provide full-coverage breast DWI with high quality and 1.25 mm isotropic nominal resolution11. AR-SMS uses standard SS SE-EPI but acquires thin sagittal slices to exploit aggressive SMS in the right/left direction, then reformats into axial slices with high in-plane spatial resolution. In this work we assess the image quality of AR-SMS in a clinical setting and compare it with a standard clinical sequence and previously proposed high-resolution RS-EPI2.
Methods
Acquisition and ReconstructionUnder an IRB-approved protocol, 30 female subjects undergoing clinical breast MRI exams were scanned prone on a 3 T Siemens Prismafit scanner using a 16-channel Sentinelle breast coil. Standard clinical scans were acquired, including a T2-weighted fast spin echo and a T1-weighted contrast-enhanced (CE) 3D gradient echo series. Parameters for the three diffusion methods are given in Table 1. The standard method (Std, with two variants A & B) was based on the ACRIN 6698 clinical trial12 to represent the most advanced clinically available breast MRI, acquired with 1.7 x 1.7 x 4 mm nominal resolution. AR-SMS was acquired with 1.25 mm isotropic nominal resolution and included an additional fully-sampled reference scan with reversed PE for topup distortion correction13. The RS-EPI sequence was based on Wisner et al.’s2 implementation with 5 readout segments and 1.8 x 1.8 x 2.4 mm nominal resolution.
The vendor’s online reconstructions were used for Std and RS-EPI DWI. AR-SMS reconstruction was performed offline in MATLAB including Ghost/Object Nyquist ghost correction14, GRAPPA, slice-GRAPPA15 for SMS, and topup distortion correction13. Separate axial b-value images and ADC maps (log-linear fit) were written to DICOM for viewing.
Reader analysis
All enhancing lesions were identified using DCE subtraction images. Two lesions of large and small size were used for training. 31 lesions (4-52 mm) were indicated on CE-subtraction images and presented in random order on a PACS workstation, including clinical images (pre-, post-, and subtraction CE and T2-weighted) and axial b = 800 s/mm2 images and ADC maps from all three DWI methods randomly labeled A, B, and C.
Three radiologists were asked to measure the longest dimension on each b = 800 s/mm2 image and the lesion-average ADC on the ADC maps; they were subsequently asked to rate their confidence in these measurements from one (no confidence) to five (very high). The overall image quality was given a score on a scale of one (unusable) to five (excellent/equivalent to CE-MRI) and ranked with respect to other methods (1st-3rd). The image quality score and ranking were fit in R (v 3.5.0) to a linear mixed effects model, including intercepts for reader and subject, while accounting for repeated measurements.
Results
Figures 2 and 3 show representative examples of a small and large lesion, including CE images that indicated the lesion of interest, and the b = 800 s/mm2 and ADC maps from all three DWI methods.Figure 4 summarizes the overall quality score and rank according to the individual readers and linear mixed effects model. All three readers scored AR-SMS with the highest overall quality and ranked it as superior most frequently. Although the agreement between the readers was poor to fair for quality score, the linear mixed effects model indicates that AR-SMS outperformed RS-EPI, followed by Std in both quality score and rank with statistical significance after accounting for reader and subject effects. The Std variants A and B were grouped for the primary analyses; no significant differences were found when repeated with A and B independently.
Figure 5 plots the confidence of measurements of lesion size (a) and ADC (b). There was a trend for higher lesion confidence using RS-EPI and even higher using AR-SMS, though it did not reach statistical significance. The DWI method did not have an effect on the confidence of the ADC measurements.
Discussion
Overall, RS-EPI and AR-SMS show clinical promise and achieve significantly higher overall image quality than the standard SE-EPI within a 5-minute scan time. Furthermore, AR-SMS was rated with higher quality than RS-EPI for a matched scan time.Despite the findings of improved image quality, and a trend toward higher confidence in size measurement on the b=800 s/mm2 images, readers did not find that the high-resolution methods improved their confidence in measuring ADCs. This may be due to the PACS software, which did not support colocalization of ROIs across ADC maps and diffusion-weighted images.
Conclusion
Readers found that AR-SMS had the overall highest image quality, followed by RS-EPI and then Std. Both high-resolution methods were significantly superior to the standard SS SE-EPI method.Acknowledgements
NIH P41 EB027061
NIH S10OD017974-01
NIH R21CA201834
References
- Bogner W, et al. Readout-segmented Echo-planar Imaging Improves the Diagnostic Performance of Diffusion-weighted MR Breast Examinations at 3.0 T. Radiology. 2012;263:64-76.
- Wisner DJ, et al. High-resolution diffusion-weighted imaging for the separation of benign from malignant BI-RADS 4/5 lesions found on breast MRI at 3T: DWI on Suspicious Breast Lesions at 3T. JMRI. 2014;40:674-681.
- Ohlmeyer S, et al. Simultaneous Multislice Echo Planar Imaging for Accelerated Diffusion-Weighted Imaging of Malignant and Benign Breast Lesions. Investigative Radiol. 2019;54:524-530.
- Filli L, et al. Simultaneous multi-slice readout-segmented echo planar imaging for accelerated diffusion-weighted imaging of the breast. European Journal of Radiol. 2016;85:274-278.
- Wilmes LJ, et al. High-Resolution Diffusion-Weighted Imaging for Monitoring Breast Cancer Treatment Response. Acad Radiol. 2013;20:581-589.
- Singer L, et al. High-resolution diffusion-weighted magnetic resonance imaging in patients with locally advanced breast cancer. Acad Radiol. 2012;19:526-534.
- Taviani V, et al. High-Resolution Diffusion-Weighted Imaging of the Breast with Multiband 2D Radiofrequency Pulses and a Generalized Parallel Imaging Reconstruction. Magn Reson Med. 2017;77:209-220.
- Granlund KL, et al. High-resolution, three-dimensional diffusion-weighted breast imaging using DESS. MRI. 2014;32:330-341.
- Gibbons EK, et al. Body Diffusion-Weighted Imaging Using Magnetization Prepared Single-Shot Fast Spin Echo and Extended Parallel Imaging Signal Averaging. Magn Reson Med. 2018;79:3032-3044.
- Solomon E, et al. Overcoming Limitations in Diffusion-Weighted MRI of Breast by Spatio-Temporal Encoding. Magn Reson Med. 2015;73:2163-2173.
- McKay JA, et al. Comparison of methods for high spatial-resolution breast diffusion imaging. Proc of 25th ISMRM. 2017:2115.
- Hylton N, et al. Diffusion Weighted MR Imaging Biomarkers for Assessment of Breast Cancer Response to Neoadjuvant Treatment: A sub-study of the I-SPY 2 TRIAL. ACRIN. https://www.acrin.org/6698_protocol.aspx
- “TOPUP,” FSL. [Online]. Available:http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/TOPUP.
- McKay JA, et al. Nyquist Ghost Correction of High-Resolution SMS Breast DWI with Ghost/Object Minimization. Proc of 27th ISMRM. 2019:3354.
- Setsompop K, et al. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn Reson Med 2012;67(5):1210-1224.
Figures
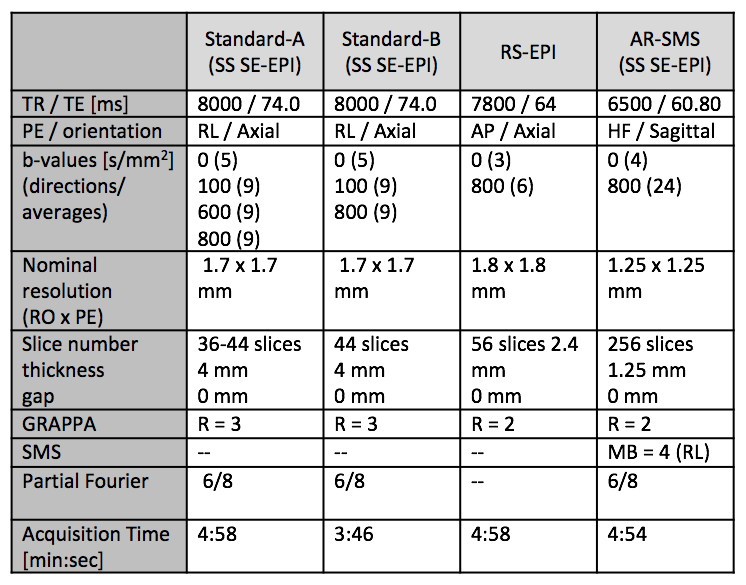
Figure 1. Table of acquisition parameters for DWI.
Std-A was used for patients of ISPY-2 clinical trial (N = 21); Std-B, with fewer b-values, was used for screening patients (N = 9) to reduce total scan time. All patients were additionally scanned with RS-EPI and AR-SMS.
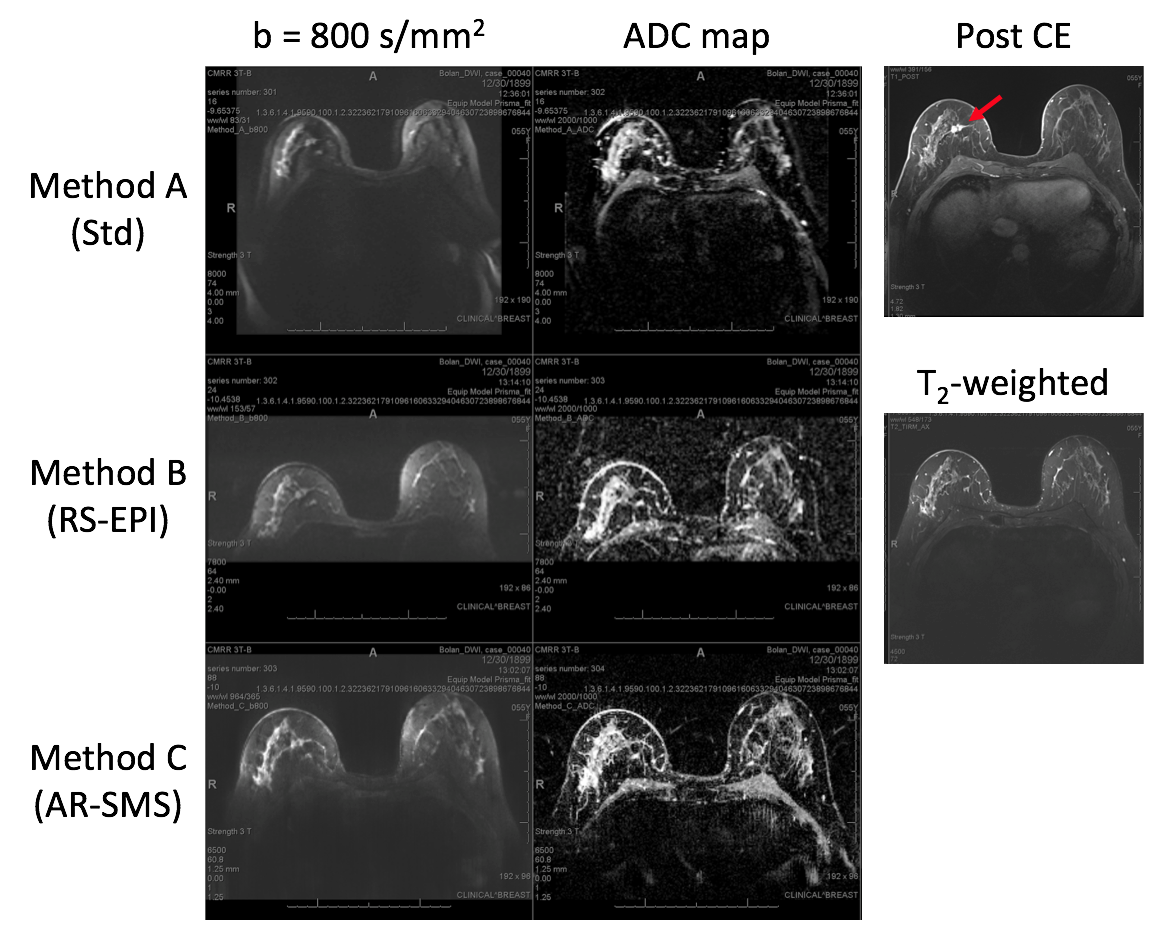
Figure 2. Screenshot of case with a small biopsy-proven cancer.
Readers were provided with axial b = 800 s/mm2 images and ADC maps for all three methods, randomly ordered A, B, and C. Anatomical post-CE and T2-weighted images are provided for comparison and to identify lesion (red arrow). Average quality scores were: A/Std= 2, B/RS-EPI = 2.7, C/AR-SMS = 2.7, indicating RS-EPI and AR-SMS were rated equivalent and better than the Std method.
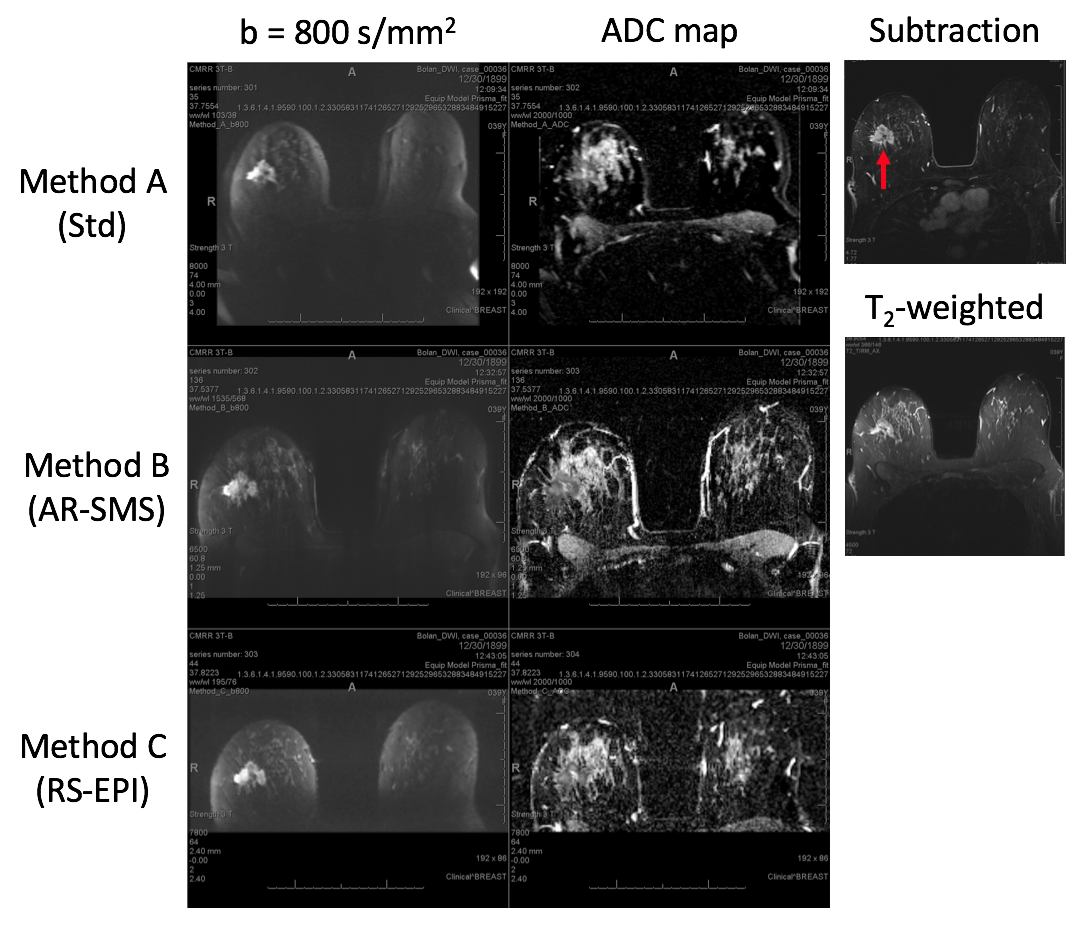
Figure 3. Screenshot of case with a large biopsy-proven cancer.
Readers were provided with axial b = 800 s/mm2 images and ADC maps for all three methods, randomly ordered A, B, and C. Anatomical CE subtraction and T2-weighted images are provided for comparison and to identify lesion (red arrow). Average quality scores were: A/Std = 2.3, B/AR-SMS = 4.3, C/RS-EPI = 3, indicating AR-SMS was scored superior, and both high resolution methods were scored as better than the Std method.
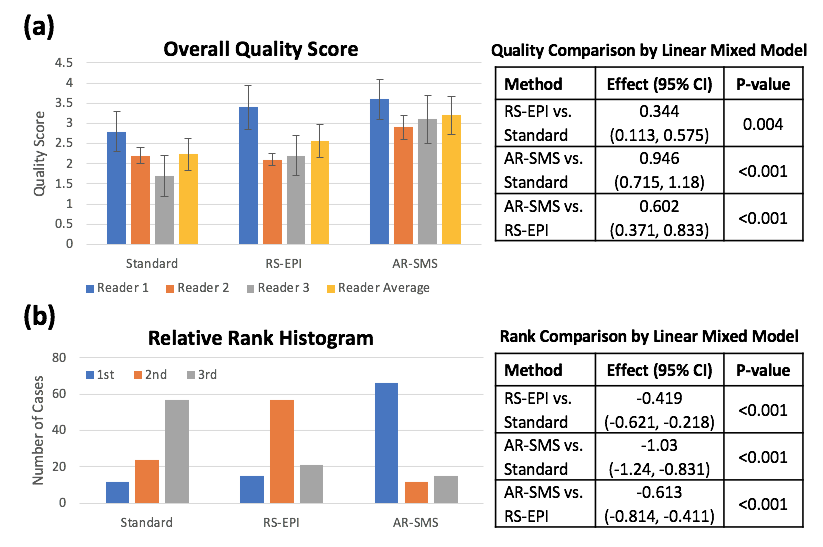
Figure 4. Summary of reader study results.
a) Mean quality scores on a per-reader basis (left) and method comparison by linear mixed model (subject and reader effects, right). Error bars indicate standard error. Overall quality was scored from 1 (unusable) to 5 (excellent/equivalent to CE). Readers consistently scored AR-SMS higher than RS-EPI and Std.
b) Histogram of relative rank for all readers and lesions and rank comparison according to linear mixed model, including significance levels. Methods were ranked 1st-3rd place. AR-SMS most frequently ranked 1st, followed by RS-EPI.
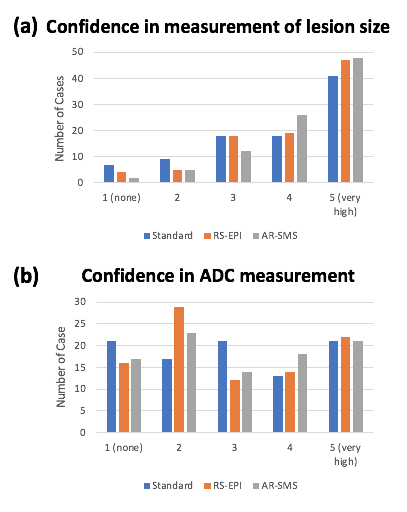
Figure 5. Confidence of lesion size and ADC measurements.
Histograms of confidence ratings in measurement of lesion size (a) and ADC (b) on DWI across all readers and lesions. Although there is a trend of higher confidence in lesion size with RS-EPI and AR-SMS, the results are not statistically significant. The ADC confidence did not depend on the DWI method (b).