2334
Pre-surgical evaluation of residual cancer by breast MRI after neoadjuvant systemic treatment with High-resolution Diffusion Weighted Imaging
Rie Ota1, Masako Kataoka1, Maya Honda1, Ayami Ohno Kishimoto1, Akane Ohashi1, Mami Iima1, Kanae Miyake Kawai1, Tatsuki R Kataoka2, Masakazu Toi3, and Kaori Togashi1
1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University graduate school of medicine, Kyoto, Japan, 2Department of Pathology, Kyoto University Hospital, Kyoto, Japan, 3Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University graduate school of medicine, Kyoto, Japan, 2Department of Pathology, Kyoto University Hospital, Kyoto, Japan, 3Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
We aimed to investigate the accuracy of high resolution-DWI (HR-DWI) using rs-EPI in estimating residual lesion size after neoadjuvant systemic treatment (NST) using pathological information as a reference. Diagnosis of pCR by two readers were accurate in 83/79 % with HR-DWI, while 50/46 % on HR-CE MRI. Spearman’s correlation coefficient between size on pathology and that on HR-DWI were 0.79 (p<0.0001), indicating strong correlations. Spearman’s correlation coefficient between size on pathology and that on HR-CE-MRI were 0.68 (p<0.0001). Using HR-DWI, residual lesions were depicted with good agreement with the pathology without using contrast agent.
Purpose
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) after neoadjuvant systemic treatment (NST) is used in evaluating residual breast cancer. However, accurate diagnosis of pathological complete response (pCR) is difficult due to various enhancement pattern after treatment (e.g. over-diagnosis by inflammation), even using high-resolution contrast-enhanced (HR-CE) MRI. Our preliminary analysis suggested that the accuracy of diagnosing pCR on MRI can be improved using DWI with single shot echo-planar imaging (ss-EPI). However, image distortion prevented accurate measurement of the residual tumor. Readout-segmented echo-planar imaging (rs-EPI) is a multi-shot sequence to reduce echo spacing and the time taken to traverse k-space in the phase-encoding direction, resulting in less-distorted image. With this technique, evaluating breast lesions using high resolution-DWI (HR-DWI) has become feasible. In this study, we aimed to investigate the accuracy of HR-DWI using rs-EPI in estimating residual lesions after NST using pathological information as a reference. The accuarcy of HR-CE was also investigate in comparison.Material and Methods
PatientsBreast cancer patients who underwent MRI including HR-DWI at the completion of NST, followed by surgery between December 2015 and July 2019 were included. Patients who underwent pre-surgical MRI after NST were searched through radiological and pathological database in our hospital.
MRI protocol
A 3.0T MRI system (Prisma: Siemens Healthcare) and 18-channel breast coil was used. Our clinical protocol included T2WI, T1WI, DWI (ss-EPI), HR-DWI(rs-EPI) for patients with known or suspicious breast lesions, T1WI-DCE and HR-CE MRI. Detailed parameters were as follows: HR-DWI: b=0,850sec/mm² (unilateral breast ipsilateral to the known/suspicious lesion; sagittal, TR/TE=8300/48.8ms, FOV=180x145mm; matrix=166x107; thickness, 1.5mm), T1-weighted DCE images(axial VIBE with fat suppression; TR/TE, 3.70/1.36 ms; FA 15; FOV=330x330mm; matrix=384x346; thickness, 1.0 mm).
Image analysis
Pre-surgical MRIs were independently evaluated by two radiologists with 20 and 3 years’ experience of breast MRI. They identify lesions on HR-DWI/HR-CE-MRI and measured their size (maximum diameters) in a sagittal plane. They were blinded to the final diagnosis of pCR, yet allowed to refer to ADC map and/or previous MRI if necessary.
1) Diagnosis of of complete response (CR)
Residual lesion was identified as the area with high signal intensity on HR-DWI, and the enhanced area on HR-CE. CR was defined as the complete lack of the area with high signal intensity on HR-DWI/the enhanced area on HR-CE.
2) Size of residual tumor
Inter-reader variability: The inter-reader variability for the lesion size in HR-DWI was evaluated by intraclass correlation coefficients (ICC).
Size measurement: Residual lesion size was determined by measuring the area with high signal intensity on HR-DWI, and by measuring the enhanced area on HR-CE. If no lesion was identified, it was diagnosed as CR and measured as 0.
Pathology analysis
Pathological diagnosis including residual cancer size was confirmed by pathology reports. pCR was defined as no invasive carcinoma (in situ lesion allowed).
Statistical analysis
Correlation between lesion size on pathology and that on HR-DWI were evaluated using Spearman’s correlation coefficient. The same analysis was performed on HR-CE MRI.
Results
1) Diagnosis of of CRIn total 57 patients (27-73 y.o.), 57 lesions were identified. Among them, 42.1% (24/57) achieved pCR while 57.9% (33/57) were categorized as non-pCR on pathology.
On HR-DWI, out of 24 pCR cases, reader 1 and 2 diagnosed 20 cases (83.3%) and 19 cases (79.2%) as CR respectively.
On HR-CE, out of 24 pCR cases, reader 1 and 2 diagnosed 12 cases (50.0%) and 11 cases (45.8%) as CR respectively.
2) Size of residual tumor
The ICC between lesion size were 0.99 (n=57) both on HR-DWI and HR-CE-MRI measured were also 0.99 (n=57). The median size on pathology, HR-DWI, and HR-CE MRI were 7mm (range: 0-172mm) 5mm (0-53mm) and 13mm (0-57mm) respectively.
Spearman’s correlation coefficient between size on pathology and that on HR-DWI were 0.79 (p<0.0001), indicating strong correlations. Spearman’s correlation coefficient between size on pathology and size on HR-CE MRI were 0.68 (p<0.0001).
The scatterplots of size on pathology and that on HR-DWI / HR-CE MRI were shown in figure 1 and Figure 2 respectively. Both plot showed similar distribution. Large tumor tended to be underestimated on both HR-DWI and HR-CE.
Representative cases are shown in Case1-3.
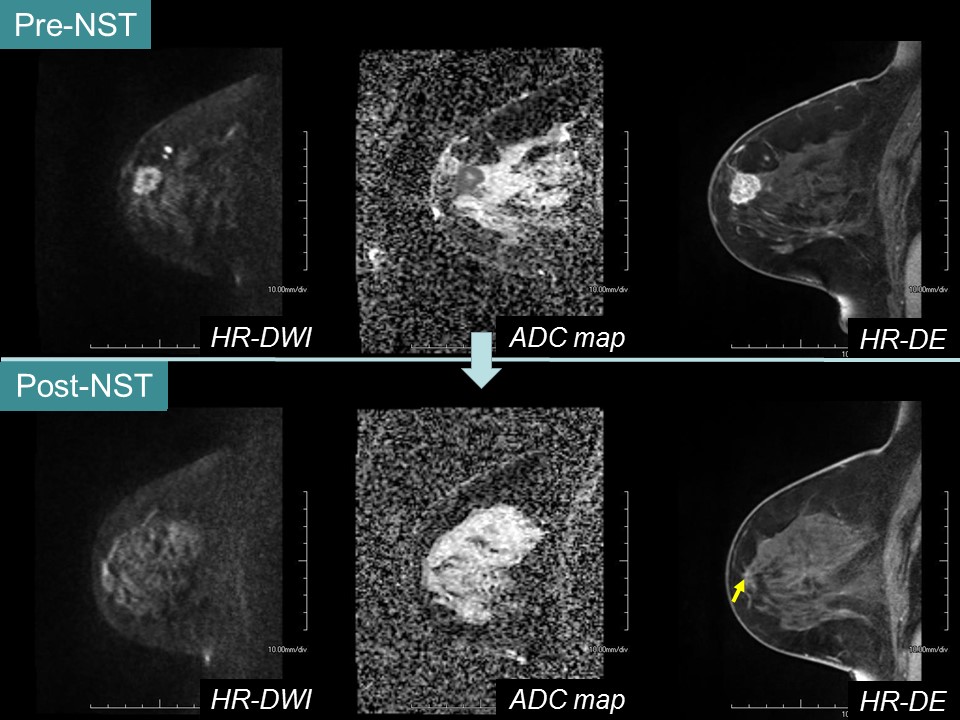
Case 1 (pCR): HR-DWI accurately diagnosed CR.
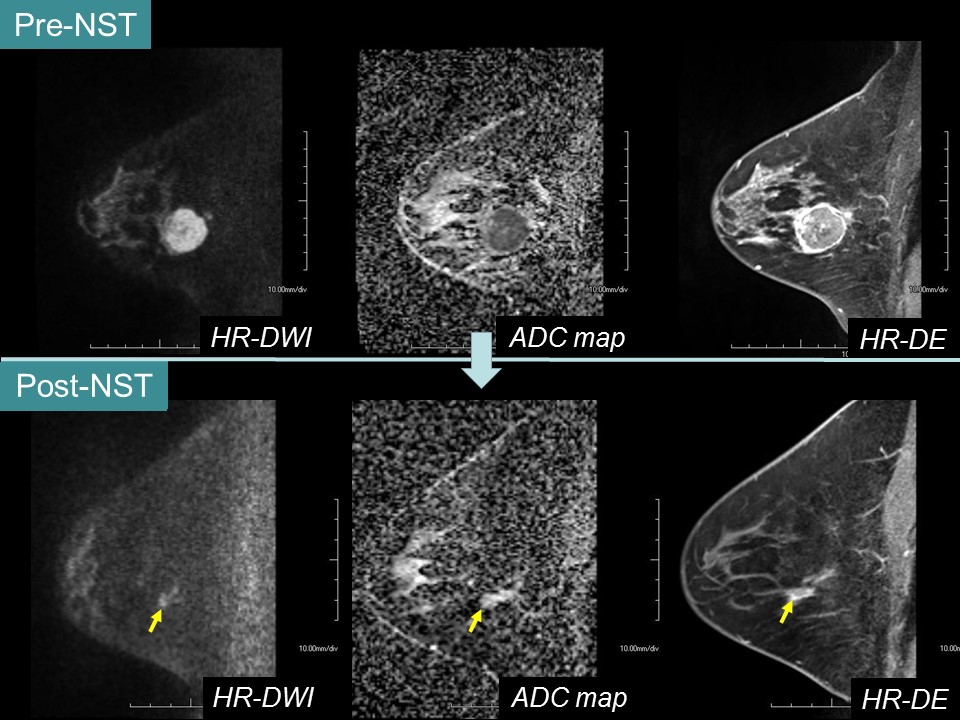
Case 2 (non-pCR): HR-DWI agreed with HR-CE MRI in depicting residual lesion.
Case 3 (pCR): false negative which both reader diagnosed high signal area as residual lesion (non-CR) on HR-DWI. ADC map showed high signal of the lesion, suggestive of non-malignant component.
Disucussion and Conclusions
Evaluation of residual tumor in post-NST MRI demonstrated better performance in diagnosing CR and better agreement in estimating residual size on HR-DWI than on HR-CE MRI. This superior performance can be attributed to the reduction of over-estimating enhanced fibrous tissues on HR-CE MRI. HR-DWI with less-distorted image may be used as a new non-contrast tool to evaluate post-treatment. A few challenging cases of high signal lesions on HR-DWI might be correctly diagnosed by combining information from ADC map.Limitations
Small sample size. Discrepant slice orientation between MRI and pathology.Acknowledgements
No acknowledgement found.References
- Lise J. Wilmes., et al., High-Resolution Diffusion-Weighted Imaging for Monitoring Breast Cancer Treatment Response. Acad Radiol. 2013 May;20(5):581-9.
- Kanao, S., et al., High-resolution diffusion-weighted MRI of the breast using readout-segmented EPI and single-shot EPI, Research Article - Imaging in Medicine, 2017. 9(6)
- Nathaniel M. Braman., et al., Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Res. 2017 July 10; 19: 80.
- Lise J. Wilmes., et al., Diffusion Tensor Imaging for Assessment of Response to Neoadjuvant Chemotherapy in Patients With Breast Cancer. Tomography. 2016 Dec;2(4):438-447
- Partridge, S.C., et al., Diffusion-weighted MRI Findings Predict Pathologic Response in Neoadjuvant Treatment of Breast Cancer: The ACRIN 6698 Multicenter Trial. Radiology. 2018 Dec;289(3):618-627.
- Kataoka, M., et al., High Resolution DWI with Readout-segmented EPI and computed DWI as a potential alternative of High Resolution Dynamic Contrast Enhanced MRI in evaluating Breast Cancer. Proc. Intl. Soc. Mag. Reson. Med. , 2016. 24.
- Iima, M., et al., Diffusion MRI of the breast: Current status and future directions. J. MAGN. RESON. IMAGING 2019 Sep14; 107-109.
Figures
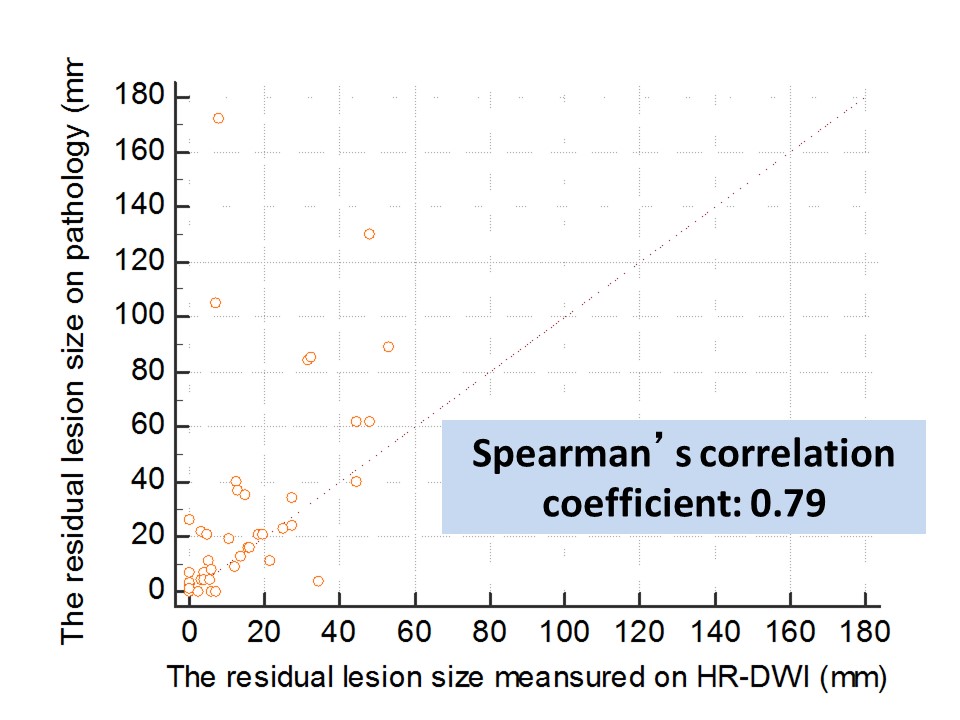
Figure 1: Scatterplot showing the correlation between size of residual tumor on pathology and HR-DWI.
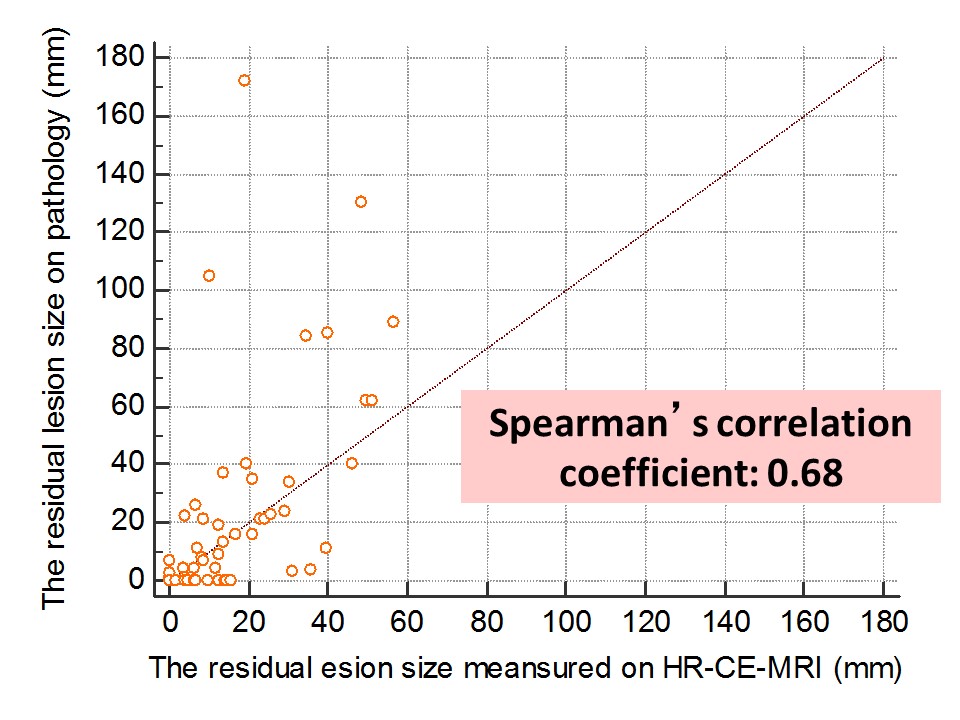
Figure 2: Scatterplot showing the correlation between size of residual tumor on pathology and HR-CE-MRI.
Case 1: Right breast cancer in
66-year-old patient underwent NST.
A
lesion on HR-DWI was not detected. Both readers classified as non-mass lesion
and measured as 4 mm
on HR-CE-MRI. There was
no residual lesion on surgery.
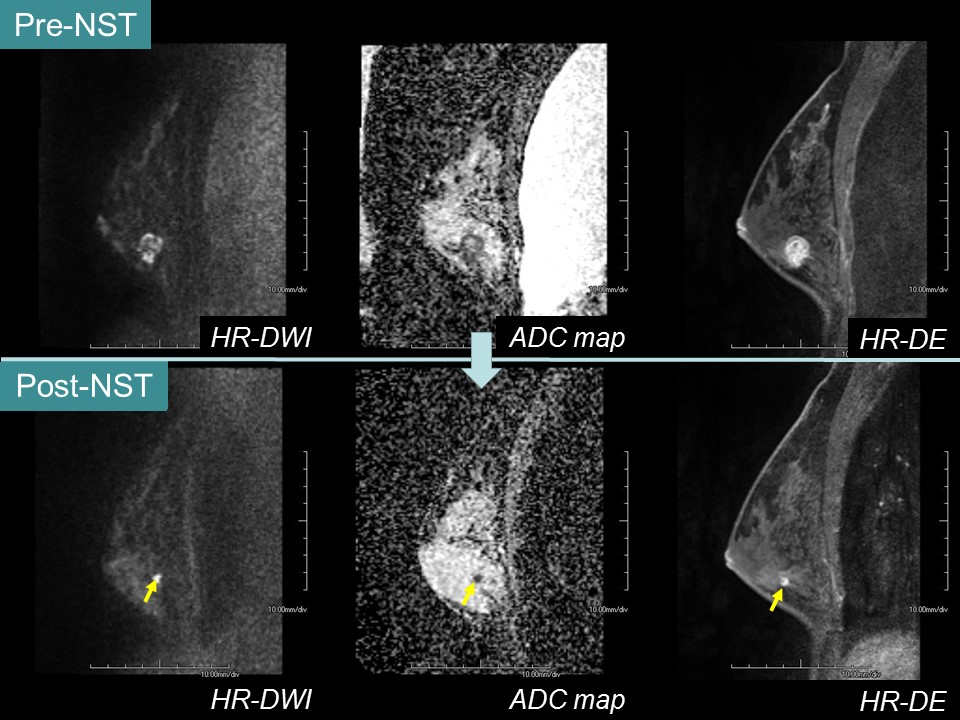
Case 2: Right breast cancer in
35-year-old patient underwent NST.
A
lesion with high signal intensity on HR-DWI was detected. Both readers measured
as 4 mm mass lesion on HR-DWI and 6 mm mass
lesion on HR-CE-MRI. ADC map
showed low signal in the lesion. The mean ADC value of lesion was 0.65×10-3 mm²/s. There residual lesion on surgery.
The pathological maximum diameter of the residual lesion was 4 mm.
Case 3: Right breast cancer in
32-year-old patient underwent NST.
A
lesion with high signal intensity on HR-DWI was detected. Both readers
identified non-lesion as mean 6 mm on HR-DWI and mean 14.5
mm
on HR-CE-MRI. ADC map
showed high signal in the lesion. The mean ADC value of lesion was 1.20×10-3mm²/s. There was no residual lesion on surgery.