2325
Combination of curve types, shape and gray level co-occurrence matrix features on breast MR to differentiate mass-like DCIS from invasive cancer1Peking University Cancer Hospital & Institute, Beijing, China
Synopsis
For radiologists, mass-like DCIS on breast MRI is unable to be distinguished from invasive ductal cancer by bare eyes. However, different treatment strategies for these two entities pushed us to do the differentiation using innovative approaches. By combining usage of tumor dynamic curve type on DCE, whole tumor shape features and features from GLCM to reflecting heterogeneity inside certain areas on MR images, we were able to achieve diagnostic accuracy 84.7% in telling DCIS from IDC in mass-like lesions, by using only one feature from each categories.
INTRODUCTION
Treatment strategies for breast invasive ductal cancer (IDC) and ductal cancer in situ (DCIS) are different. DCIS, though tend to behave benignly in biological nature, is resistant to neoadjuvant chemotherapy. Biopsy was the only way to acquire pathologic results before therapy, but was subject to misleading results caused by heterogeneity inside the tumors. Since DCIS can appear as various morphologies on imaging, it remains a problem to distinguish DCIS from IDC reliably on images, especially for those with mass-like morphology. Thus we made a hypothesis that the interpretation of tumor heterogeneity by gray level co-occurrence matrix (GLCM) along with blood supply may help to distinguish DCIS from IDC on dynamic contrast enhanced MR (DCE-MRI).METHODS
his is a retrospective study enrolling breast cancer patients who received either lumpectomy or mastectomy starting from January 2018. Two radiologists were asked to defined the lesions as mass-like or non-mass-like on MRI. According to operational pathology reports, consecutive 48 IDC patients and consecutive 24 DICS patients with mass like lesions on MRI were included. Initial MR images at the time of diagnosis were retrieved. Regions of interest (ROI) were drawn manually on early phase of DCE images and covered the whole enhanced areas using threshold drawing method. Thus whole tumor ROIs were extracted for the following analysis using a house made radiomics software based on 3D slicer. Five basic GLCM features (energy, entropy, correlation, contrast and inverse variance) on early and late enhancing phase respectively, and five basic shape features (volume, major axis, least axis, flatness and surface-volume-ratio) were acquired. Dynamic curve types were classified into 3 types according to the changing rates of mean signal intensities from early to late phases. Initial comparisons between DCIS and IDC were made using Mann-Whitney U test to select potential valuable features, and then binary logistic regression analysis were used to pick variables and assess the diagnostic abilities.RESULTS
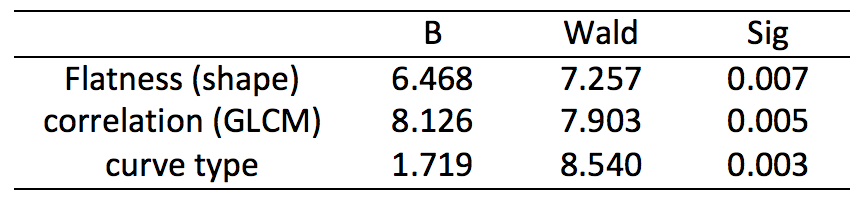
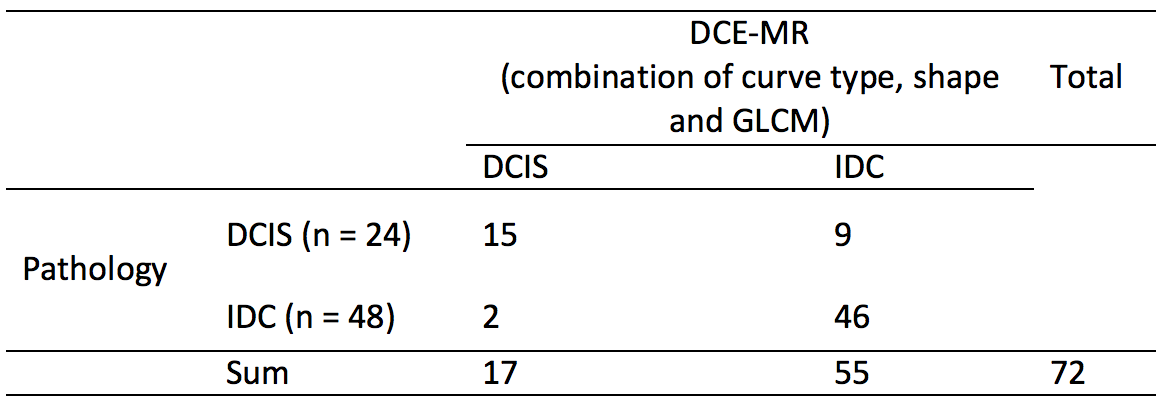
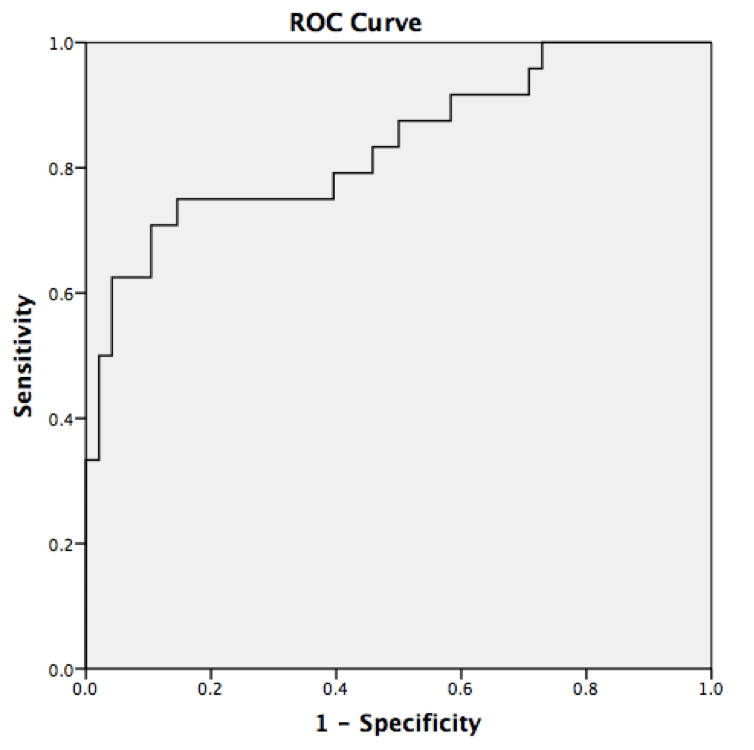
Significant differences between DCIS and IDC were seen in 7 variables, including volume, least axis, flatness and surface-volume-ratio, GLCM correlation and curve type (P<0.01). Binary logistic regression analysis finally revealed the combination of three variables from each three categories (curve type, flatness from shape, correlation from GLCM of late phase) to compose a formula (fig 1) and achieve as high as 84.7% accuracy in diagnosing DCIS (figure 2), AUC=0.836 (figure 3).DISCUSSION
There were some imaging finding on MRI that can be used to distinguish DCIS from IDC, but only applicable for non-mass-like lesions, not for mass-like ones [1]. So it is quite impossible for radiologists to do the differentiation using bare eyes. Innovative approaches of images provide us with a way to further analyze the heterogeneity inside the tumor areas beyond the touch of human eyes. There were researches using quantitative ADC values of diffusion-weighted MRI to distinguish DCIS and IDC [2], but the image quality of DWI remains challenging and may cause artifacts that affect results. Only adopting numerous features from imaging radiomics has the problem of reliability and stability. Thus we simply picked the basic GLCM features, and altogether with tumor shape features and dynamic curve types. Only one feature in GLCM (correlation) and only one feature in shape, along with curve type, were finally involved in final formula and achieved high accuracy in differentiated DCIS from IDC.CONCLUSION
To differentiate mass-like DCIS from IDC on MRI, combination of variables from tumor shape, enhancing curve type and GLCM can help to achieve high diagnostic accuracy.Acknowledgements
Thank Hui Liu, Ph.D. for integrating and modifying the radiomics software.References
[1]. Goto M, Yuen S, Akazawa K, et al. The role of breast MR imaging in pre-operative determination of invasive disease for ductal carcinoma in situ diagnosed by needle biopsy. Eur Radiol. 2012 Jun;22(6):1255-64. doi: 10.1007/s00330-011-2357-2.
[2]. Bickel H, Pinker-Domenig K, Bogner W, et al. Quantitative apparent diffusion coefficient as a noninvasive imaging biomarker for the differentiation of invasive breast cancer and ductal carcinoma in situ. Invest Radiol. 2015 Feb;50(2):95-100. doi: 10.1097/RLI.0000000000000104.
Figures