2324
Prediction axillary lymph node status of Breast Cancer by MRI Radiomics1Chongqing University Cancer Hospital & Chongqing Cancer Institute & Chongqing Cancer Hospital, ChongQing, China, 2Philips Healthcare, Shanghai, China
Synopsis
To establish a radiomic model based on dynamic contrast enhanced (DCE) magnetic resonance imaging predicting ALN status noninvasively before operation.
Background
The status of axillary lymph node (ALN) is closely related to the prognosis of the patients with breast cancer, and determines the mode of surgery and the formulation of adjuvant treatment [1,2]. ALN status is currently determined by invasive SLN biopsy in clinical practice.Methods
In this retrospective research, we collected 197 patients who underwent breast magnetic resonance dynamic enhancement before operation and had confirmed postoperative pathology for breast cancer from September 2016 to May 2019. According to the postoperative pathology, the patients were divided into ALN-metastasis group(82) and non-ALN-metastasis group(n=115),then the patients were randomly assigned to training group(n=131) and verification group(n=66). A dedicated software (Philips radiomics tool) was used to draw the contour of the tumors in the early phase and late phase enhanced Silhouette images and calculate the features. A total of 3386 radiomic features were extracted from each patient include tumor intensity statistics, size and shape, intensity statistics, and texture feature using pyradiomics [3]. In the following feature dimension reduction analysis, we used Spearman correlation analysis to select the key features. In modeling stage, we investigated 5 classification methods (including Passive Aggressive Classifier, Perceptron, Ridge Classifier, SGD Classifier, Logistic Regression, Linear SVC) for training and prediction. We use 5-fold cross validation results as the performance of a specific machine learning classifier. We use ’accuracy’ as the optimization metric to select the classifier. The model was trained on the training cohort and their performance was evaluated on the cross-validation cohort using the area under ROC curve (AUC).Results
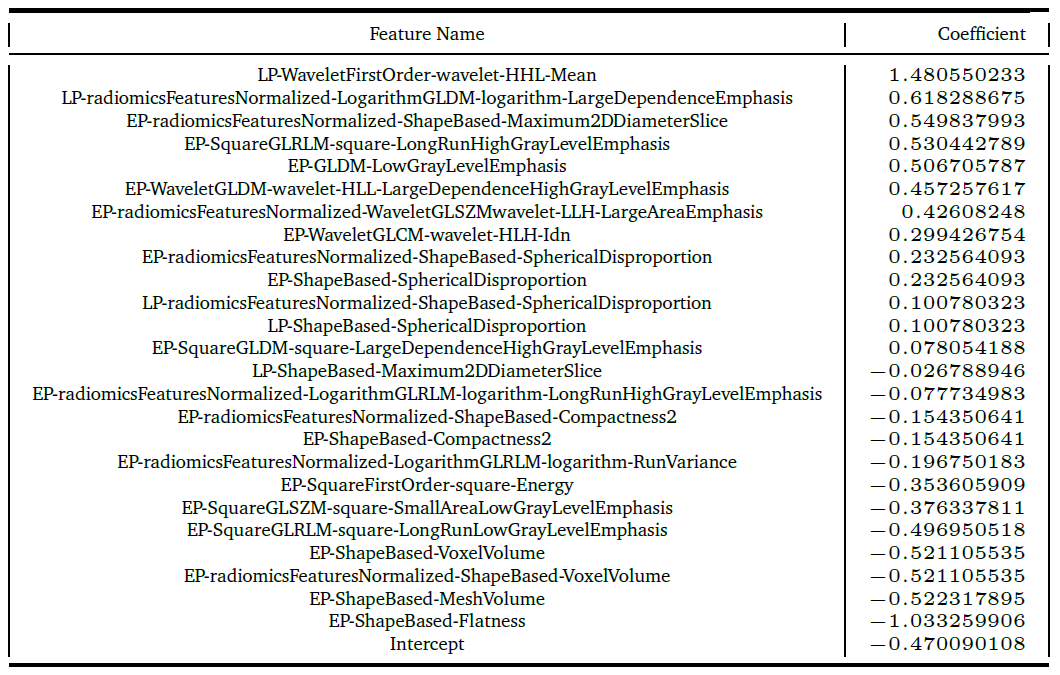
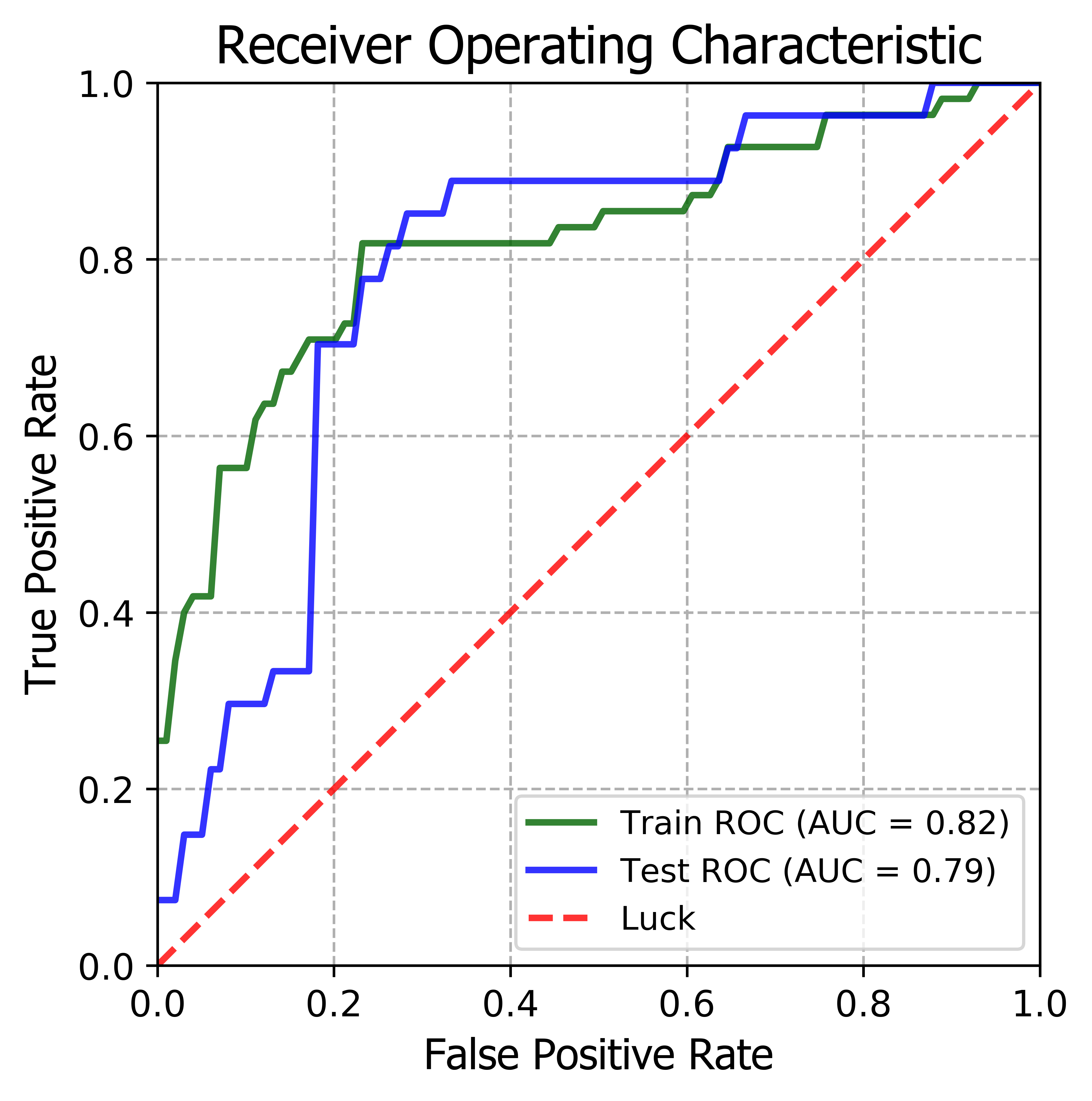
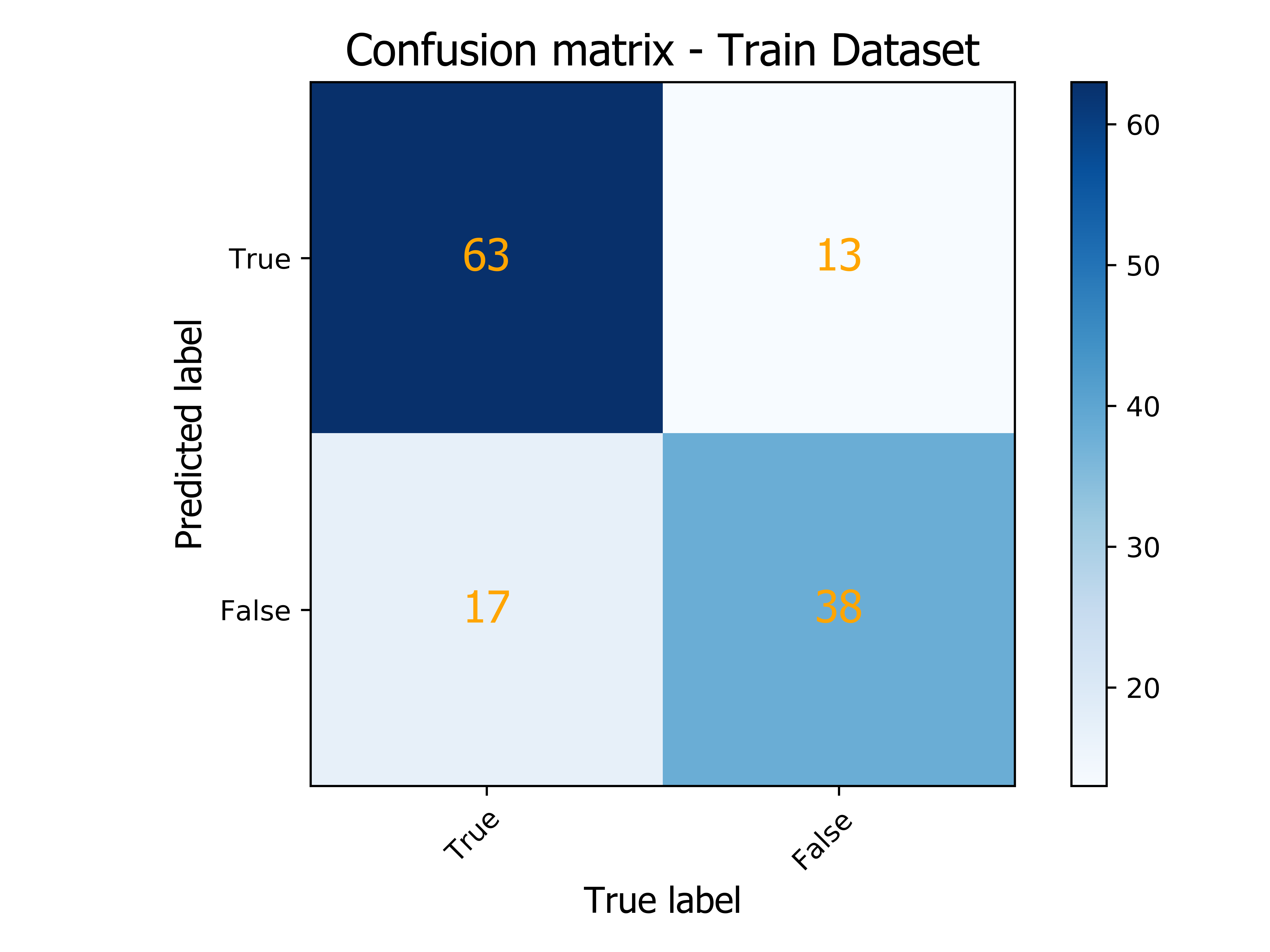
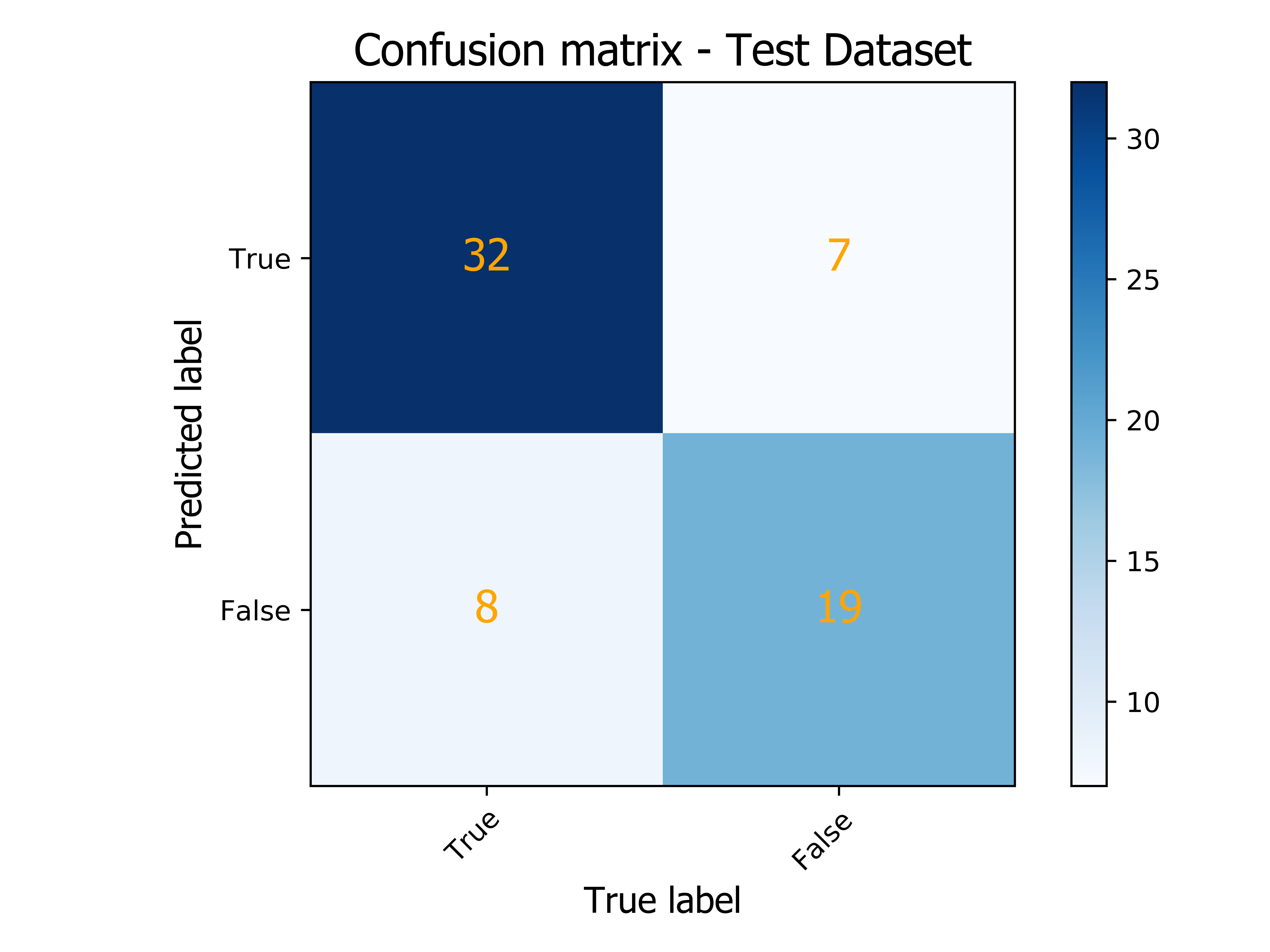
25 radiomic features were select the key features to predict ALN status, Including 20 features from early phase enhanced images and 5 features from late phase enhanced images. Ridge Classifier was found to produce the most accurate model on training dataset. The prediction model displayed an AUC of 0.82 and 0.79 for predicting ALN status in the training group and validation group, respectively.Conclusion
Our result shows that some radiomics features have great potential to be an useful index in predicting ALN status, therefore providing helps for the development of clinical treatment decisions for breast cancer.Discussion
This study tried to predict the ALN metastasis in patients with breast cancer by DCE-MRI radiomic characteristics, and showed good predictive performance in the training group and validation group, respectively (AUC 0.85 ,0.79). MSKCC Nomogram is a model to predict the SLN status which developed by The Memorial Sloan-Kettering Cancer Center. It based on some clinicopathological characteristics, such as tumor size, and pathological type and age, the AUC was 0.754 [4]. Compared with MSKCC Normogram, The predictive efficiency of our radiomic model is better, and as a non-invasive method, which can be carried out before operation, and radiomic will have the potential to provide more auxiliary information for clinical treatment.Acknowledgements
No acknowledgement found.References
1. Weigel MT, Dowsett M. Current and emerging biomarkers in breast cancer: prognosis and prediction. Endocr Relat Cancer. 2010;17(4):R245-262.
2. DeSantis CE, Lin CC, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin. 2014;64(4):252-271.
3. van Griethuysen, J. J. M., Fedorov, A., Parmar, C., Hosny, A., Aucoin, N., Narayan, V., Beets-Tan, R. G. H., Fillon-Robin, J. C., Pieper, S., Aerts, H. J. W. L. (2017). Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Research, 77(21), e104–e107.
4. Bevilacqua JL, Kattan MW, Fey JV, Cody HS, 3rd, Borgen PI, Van Zee KJ. Doctor, what are my chances of having a positive sentinel node? A validated nomogram for risk estimation. J Clin Oncol. 2007;25(24):3670-3679.
Figures