2320
Shortening Diagnostic T2w Breast Protocols to Capitalize on the Benefits of a Deep Learning Reconstruction
Timothy J Allen1, Leah C Henze Bancroft2, Roberta M Strigel1,2,3, Ty Cashen4, Orhan Unal2, Frank R Korosec1,2, Ping Wang1, Lloyd Estkowski4, Fred Kelcz2, Amy M Fowler1,2,3, R Marc Lebel4, and James Holmes2
1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Carbone Cancer Center, University of Wisconsin-Madison, Madison, WI, United States, 4Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States
1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Carbone Cancer Center, University of Wisconsin-Madison, Madison, WI, United States, 4Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States
Synopsis
A SSFSE-based fast acquisition was used in conjunction with a vendor-supplied, deep learning-based reconstruction to obtain T2-weighted images (Rapid T2w+DL) for diagnostic breast MRI. Radiologists compared the Rapid T2w+DL images to standard-of-care T2w FSE images assessing both image quality and utility in completing a typical clinical task. The fast acquisition provided a reduction in average scan time from 3:35 (min:sec) to 1:16 (64%). Deep learning was used to alleviate issues associated with the fast protocol (e.g. blurring and reduced SNR). Rapid T2w+DL images allowed for completion of the clinical task with results comparable to those obtained with standard T2w images.
Motivation
T2w imaging is routinely used in diagnostic breast MRI to identify benign features (e.g. benign cysts) and assist with differential diagnosis as benign findings are more likely to be T2 hyperintense (i.e. fibroadenomas). Historically, RARE acquisitions1 including fast spin echo (FSE) have been relatively long due to the need for limited echo trains to minimize T2 blurring and long TRs to allow T1 recovery. With increased desire to improve breast exam efficiency, many clinical practices have modified their protocols to save scan time, leading to compromised SNR or limited spatial resolution. Deep learning (DL) provides an opportunity to deviate from the conventional paradigm of trading off scan time, resolution, and SNR.We propose using a faster single-shot FSE (SSFSE) acquisition with a DL reconstruction to obtain T2w breast images. Inherently, SSFSE produces images with increased spatial blurring and reduced SNR. However, application of the DL reconstruction is expected to alleviate these issues and produce images comparable to those obtained with a slower conventional T2w FSE.
Methods
Patients scheduled for standard clinical breast MRI exams were approached to participate in this IRB-approved, HIPAA-compliant study. Participants (N=7) received a standard-of-care breast MRI exam on a 3T scanner (SIGNA Premier or Discovery 750w, GE Healthcare, Waukesha, WI) including a standard clinical T2w FSE series (echo train: 8, 288x288 matrix, 2.0 mm slices, mean scan time: 3:35 min:sec). A rapid T2w acquisition was performed using SSFSE (288x288 matrix, 2.0 mm slices, mean scan time: 1:16). The SSFSE series were reconstructed using a vendor-supplied, DL-based reconstruction prototype (DLRecon) trained to reduce noise, enhance sharpness, and remove simple artifacts. The combination of SSFSE with DLRecon is referred to as Rapid T2w+DL.A board-certified, breast imaging fellowship-trained radiologist (radiologist A) reviewed the clinical exams and identified features of interest including malignancies, cysts, and edema. Two additional board-certified radiologists (readers) reviewed and scored features identified by radiologist A. First, the standard T2w and Rapid T2w+DL images were evaluated side-by-side using a five-point Likert scale to assess the SNR, artifacts, image sharpness, and overall image quality (Table 1). A score of three or higher indicated images were of sufficient quality to aid in diagnosis. Radiologists were then shown contrast-enhanced T1w images with annotated features alongside both T2w images. Readers rated the feature signal intensity (low=1 to high=5) on both T2w images. Lastly, readers selected which T2w image they preferred considering image quality and feature signal intensity task.
In addition to the clinical patients, normal volunteers (N=3) were imaged with the standard T2w FSE and Rapid T2w+DL protocol on a 1.5T scanner (SIGNA Artist, GE Healthcare, Waukesha, WI). Images obtained at 1.5T have reduced SNR and are therefore apt to further benefit from DLRecon. For 1.5T scanning, the slice thickness was increased to 2.4 mm and the Rapid T2w+DL protocol used a 320x192 matrix to partially compensate for field strength SNR differences. 1.5T images were reviewed by the readers and their image quality was scored.
Results
Acquisition times for the standard T2w scans were between 2:46 (min:sec) and 4:29 (mean: 3:35) and for the Rapid T2w+DL were between 0:52 and 1:45 (mean: 1:16). Images from a typical volunteer (Figure 1) demonstrate the denoising and sharpening of features provided by DLRecon. As shown in Figure 2, T2w images and Rapid T2w+DL images from a patient with T2 bright cysts show comparable T2w contrast. An example of a T1 bright finding is demonstrated in Figure 3.A summary of results from the review by the radiologists is shown in Figure 4.The mean brightness of lymph nodes (N=9) in the standard T2w images was 4.4 compared to 4.5 in the Rapid T2w+DL. Cysts (N=6) had a mean brightness of 4.2 and 3.7, respectively, and known malignancies (N=2) 3.5 and 3.3, respectively. Single examples of additional features were rated equally bright on each T2w image: hematoma, edema, seroma, nonmass enhancement, and benign background enhancement.
Reader one rated the overall quality of the Rapid T2w+DL as 3.1 at 3T and 3.3 at 1.5T. They rated the overall quality of the standard T2w images as 3.7 at 3T and 4.0 at 1.5T (Figure 4). They preferred standard T2w images in eight out of the ten cases. Reader two rated the overall quality of the Rapid T2w+DL as 4.7 at 3T and 5.0 at 1.5T, while rating the standard T2w images as 4.0 regardless of field strength. They preferred the Rapid T2w+DL images in 8 out of 10 cases.
Discussion
Time reduction in the Rapid T2w+DL protocol could be highly beneficial in a clinical environment, especially for sites using an abbreviated breast MRI protocol. In our study, scores were similar for the feature-based assessment and image quality in the T2w images and the Rapid T2w+DL images despite the reduced scan time for the latter. Signal characteristics of the standard T2w scan were preserved in the Rapid T2w+DL images. Both radiologists agreed that both T2w protocols produced images of good quality providing initial evidence that a SSFSE sequence with deep learning could be used as a substitute for slower FSE scanning. Our preliminary results are encouraging, but further study is necessary.Acknowledgements
This project was supported by the Departments of Radiology and Medical Physics, University of Wisconsin.References
1. J. Hennig; A. Nauerth; H. Friedburg (1986), "RARE imaging: A fast imaging method for clinical MR", Magn Reson Med (in German), 3 (6), pp. 823–833, doi:10.1002/mrm.1910030602Figures
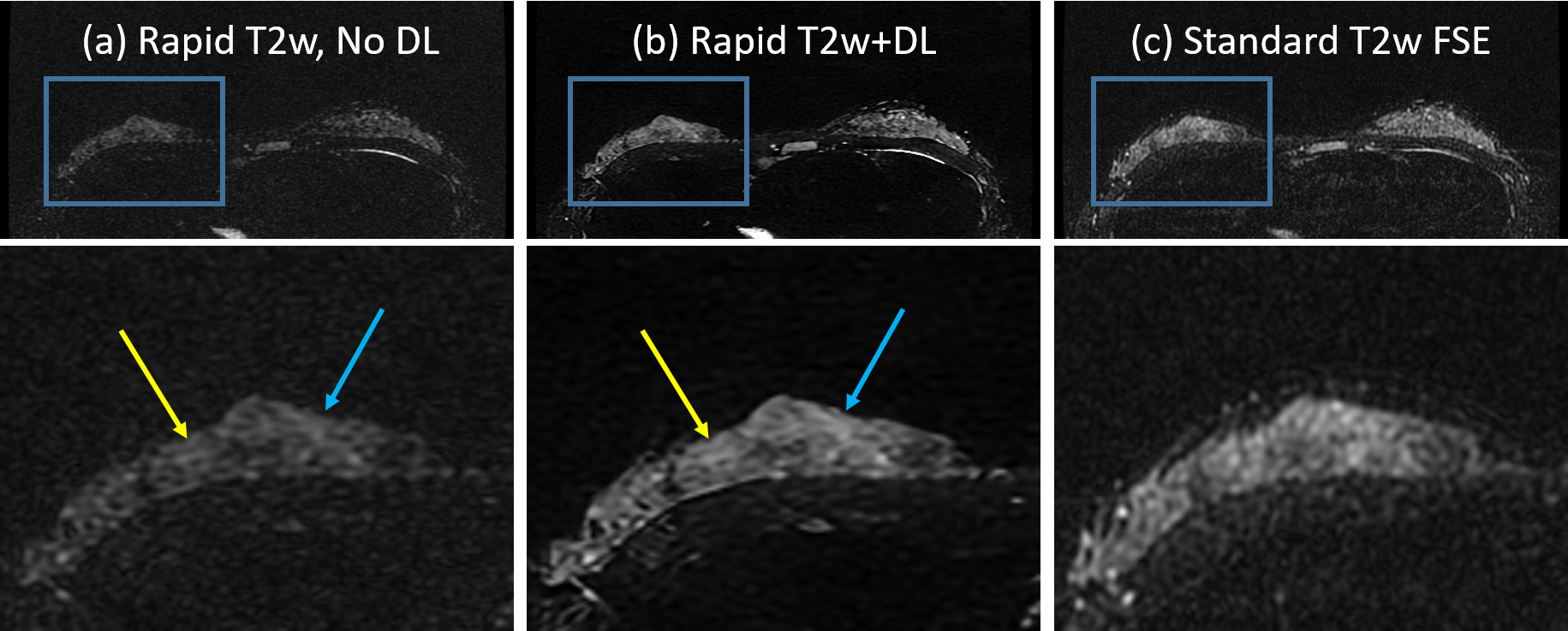
Figure
1: As expected, the SSFSE fast T2w images (in this case acquired at 1.5T)
(a) showed reduced SNR compared to the standard longer FSE T2w images (c).
However, application of the DL reconstruction to the SSFSE data (b) results in
denoising (yellow arrow) and sharpening of features (blue arrow). These become better visualized in the
magnified views of fine detail tissue features (inset).
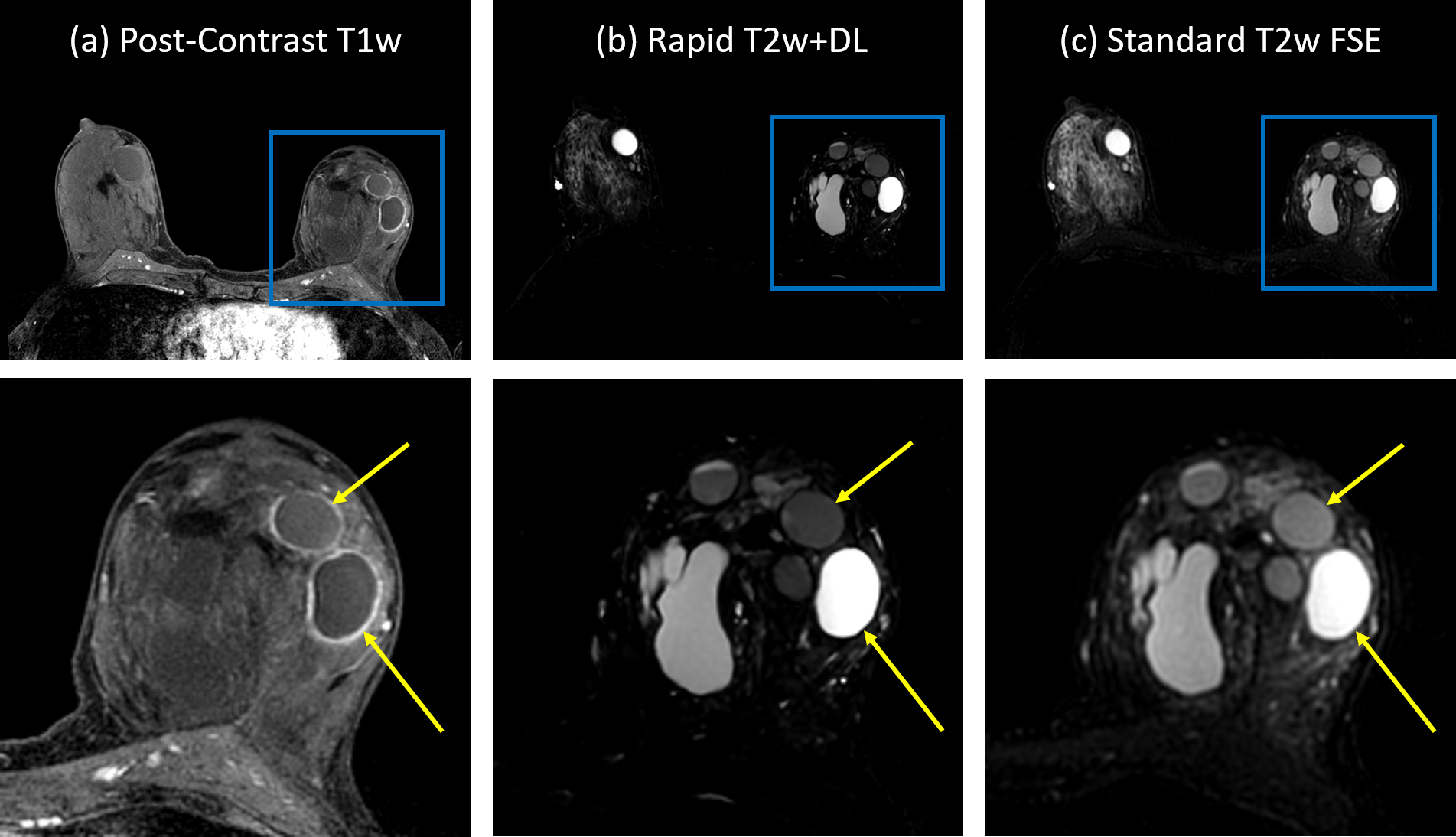
Figure 2: (a) First phase of T1w post-contrast 3D spoiled gradient echo sequence. Many
cysts are visible and some have enhancing margins (arrows). Corresponding
features in the T2w images show similar brightness on both the Rapid T2w+DL acquisition
(b) and the standard T2w acquisition (c).

Figure 3: An example of a region of enhancement noted on the
T1w image (a, arrow). In both the Rapid T2w+DL (b) and standard T2w (c) images,
the region of brightness was scored at a level of 4.5 by both readers in both
T2w images.
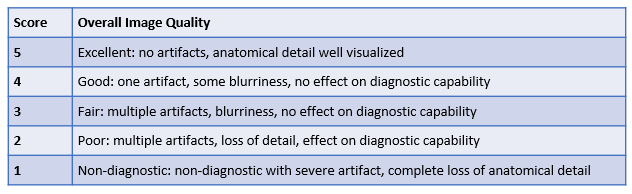
Table
1: Scoring criteria used to rate
image quality.
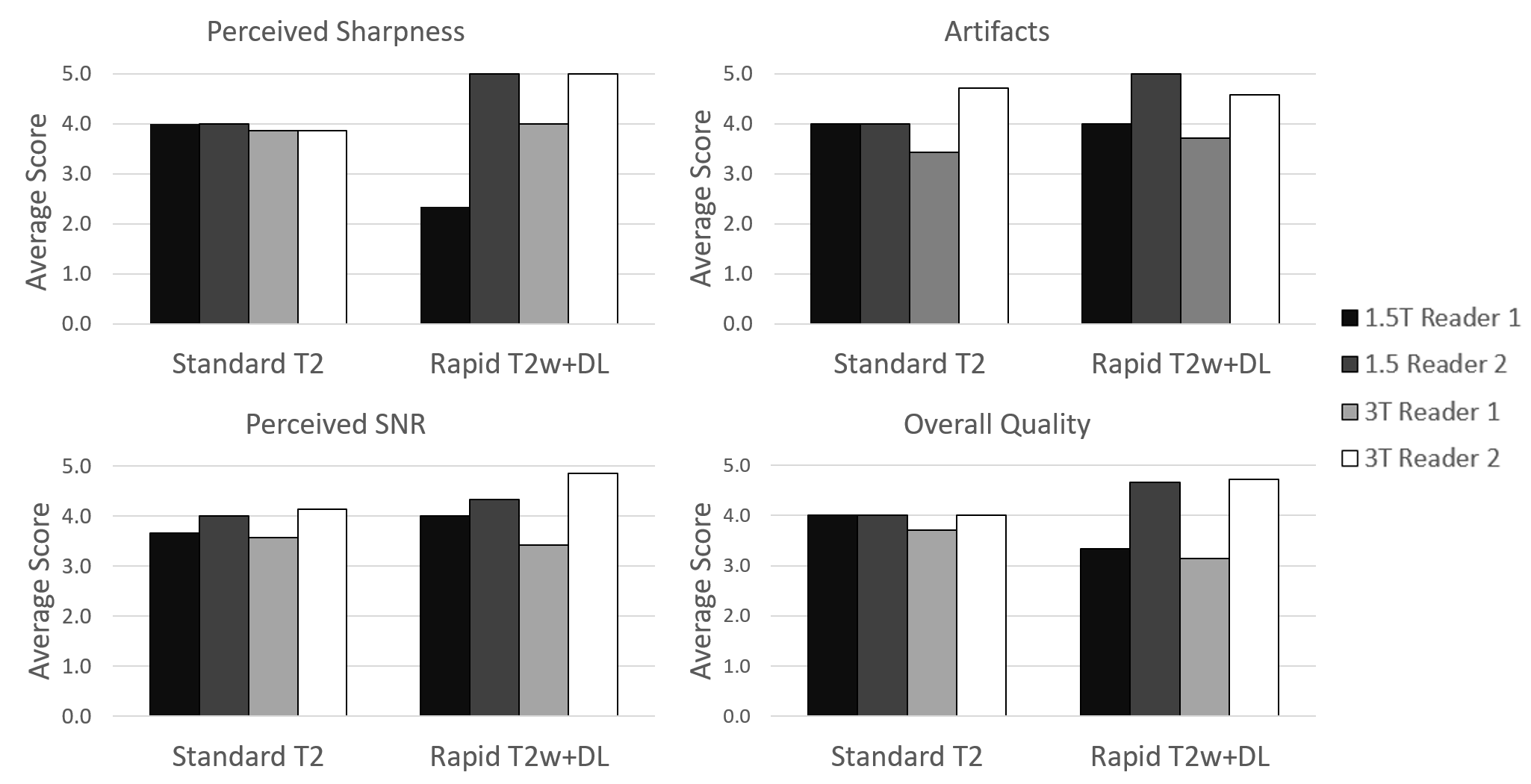
Figure 4: For overall quality, both the standard T2w and the
Rapid T2w+DL images were rated above a 3.0 indicating that any imperfections caused
by the rapid SSFSE acquisition did not have an impact on the diagnostic utility
of the image when reconstructed using the DL recon. This was true for both 1.5
and 3.0T imaging. Overall image quality scores are shown along with scores for
perceived sharpness, artifacts, and perceived SNR.