2276
Investigation of multi-site reliability and reproducibility study of non-respiratory gated cardiovascular 4D flow MRI1Radiology department, Hubei Shiyan Taihe Hospital, Shiyan, China, 2GE healthcare China, Beijing, China, 3Radiology department, Changzhou No2 people hospital, Changzhou, China
Synopsis
Respiratory gating or navigator technique is used in 4D flow imaging to reduce the effect of respiratory motion. Non-respiratory gated 4D flow MRI reduces the overall scan time but may face uncertainty in reproducibility and reliability. In this work, the reliability and reproducibility of non-respiratory gated 4D flow was investigated in 10 patients and 3 different sites in two separate scans. Better measurement consistency was observed intra-site than inter-site. The intra-correlation coefficient results showed excellent to good reproducibility between sites were observed ( ICC > 0.95 for blood flow, ICC > 0.85 for peak). Bland–Altman analysis also showed great test-retest reliability.
Purpose
To systematically investigate the multi-site reproducibility, test-retest reliability and observer variability of non-respiratory gated 4D flow MRI in the thoracic great vessels for the assessment of blood flow and peak velocity.Introduction
The 4D flow MRI shows great potential in quantitative assessment of hemodynamic features of other cardiovascular diseases, especially in the application of congenital heart diseases [1]. Typically, respiratory gating or navigator technique is used in 4D flow imaging to reduce the effect of respiratory motion, which inevitably prolongs the acquisition time. It could be very challenging for patients with severely illness to complete the whole scan. It has been further demonstrated that 4D flow MRI without respiratory gating may reduce the scan time up to 60% compared to those with respiratory gating [2]. 4D flow without respiratory gating holds promises for its widespread clinical applications, however whether non-respiratory gating may cause additional measurement disturbance stays unknown. This study is set to investigate the multi-site reproducibility, test-retest reliability and observer variability of non-respiratory gated 4D flow MRI.Material and Methods
This study was approved by the local ethics board and written informed consents were obtained from all subjects before MRI examinations. Ten healthy subjects (6 males, 4 females, age 264) without a history of cardiovascular diseases were recruited in this study. All participants underwent 4D flow MR scan in three sites equipped with the same MR scanner (MR750w, GE, WI) and eight-channel cardiac coil, all the participants were scanned twice in two separate visits. The same protocol was followed using the kat-ARC sequence [3]: TE/TR = 2.1/4.2 ms, flip angle = 8, FOV = 320 x 320 mm, matrix size = 180 x 180, velocity encoding sensitivity along all three directions = 150 cm/s. A total of 74 axial slices were acquired to cover the whole chest with a slice thickness = 2.4 mm, which was then interpolated to 1.2mm. Flow analysis of acquired 4D flow data was performed using the Arterys (Arterys Inc, CA) [4]. For each acquisition, region of interest (ROI) based measurements of blood flow (mL/beat) and peak velocity (cm/s) were performed in ascending aorta and pulmonary artery. ROIs were semi-automatically placed above the valves using Arterys software. The coefficients of variance (CVs) were calculated to measure the multicenter (inter-site) variance and test-retest (intra-site) variance. The multi-center reproducibility was assessed by two-way mixed effect intra-class correlation coefficient (ICC). The test-retest reliability was evaluated using the Bland-Altman test. The Pearson correlation coefficient was computed to assess the level of test-retest agreement.Results
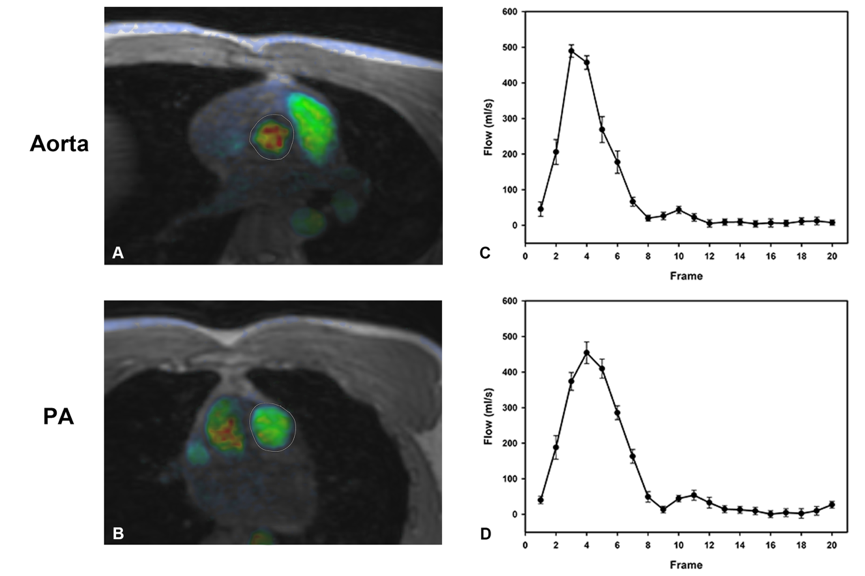
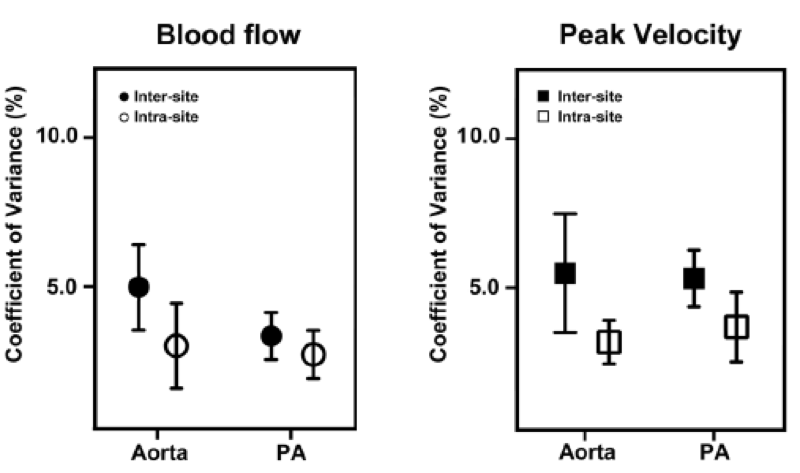
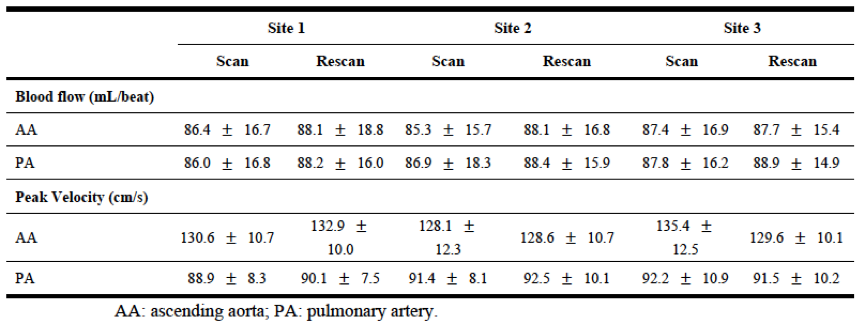
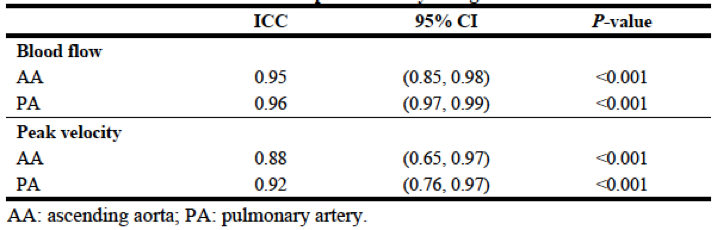
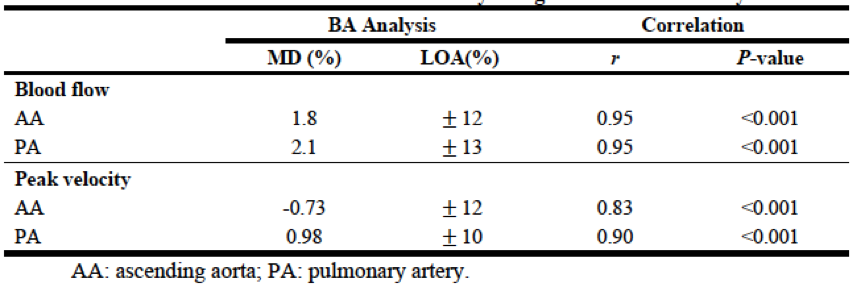
The measured blood flow waveform of one typical volunteer accompanied with the ROIs are shown in Figure 1, measurements from each scan are summarized in Table 1. CVs of both intra- and inter-sites scans are shown in Figure 2. It was seen that inter-site measurements tended to have higher CV values than those of intra-site for both blood flow and peak velocity. Overall, CV values indicated good inter- and intra-site data consistency. The multi-site reproducibility assessed by ICCs for all measurements were listed in Table 2. Great multi-site reproducibility was observed for both blood flow measurements (all ICC values were larger than 0.95). For peak velocity measurements, all ICC values were greater than 0.85, which indicated good multicenter reproducibility of peak velocity measurements. In addition, to demonstrate the test–retest reliability of both blood flow and peak velocity, the Bland–Altman analysis was used and detailed results were summarized in Table 3. Both blood flow and peak velocity showed good test–retest agreements in all measurements (MD < 3%). The Pearson correlation analysis also showed significant test–retest agreement (all r > 0.80 and P < 0.001).Discussion and conclusion
Quantitative assessment the hemodynamic properties of blood flow from both aorta and pulmonary artery is critical for cardiovascular diseases such as valve diseases, vascular stenosis, vessel wall diseases and even congenital heart diseases. The progression of 2D PC MRI to 4D flow allows simultaneous visualization of both relevant anatomical structures and velocity field, as well as easy scan prescription. However, its relatively long scan time holds back the clinical applications of 4D flow MRI. Respiratory gating reduces the respiratory motion, but may significantly prolong the overall scan time. In the present study, the multi-site reproducibility, test–retest reliability, and inter-observer agreement of non-respiratory gated 4D flow MRI in measuring blood flow and velocity of thoracic great vessels were evaluated. Good test–retest reliability, multicenter, and inter-observer agreements were obtained. The accuracy of 4D flow has been previously investigated and reported [5], confidence of its reproducibility without respiratory gating may further enhance its clinical applications.Acknowledgements
No acknowledgement found.References
[1] Vasanawala SS, Hanneman K, Alley MT, Hsiao A. Congenital heart disease assessment with 4D flow MRI. Journal of Magnetic Resonance Imaging 2015;42(4):870-86.
[2] Kanski M, Töger J, Steding-Ehrenborg K, Xanthis C, Bloch KM, Heiberg E, et al. Wholeheart four-dimensional flow can be acquired with preserved quality without respiratory gating, facilitating clinical use: a head-to-head comparison. 2015;15(1):20.
[3] Lai P, Shimakawa A, Cheng JY, Alley MT, Vasanawala S, Brau AC. Sub-8-minute cardiac four dimensional flow MRI using kat ARC and variable density signal averaging. Journal of Cardiovascular Magnetic Resonance 2015;17
[4] Chelu RG, Wanambiro KW, Hsiao A, Swart LE, Voogd T, van den Hoven AT, et al. Cloudprocessed 4D CMR flow imaging for pulmonary flow quantification. 2016;85(10):1849-56.
[5] Feneis JF, Kyubwa E, Atianzar K, Cheng JY, Alley MT, Vasanawala SS, et al. 4D flow MRI quantification of mitral and tricuspid regurgitation: Reproducibility and consistency relative to conventional MRI. Journal of Magnetic Resonance Imaging 2018.
Figures