2267
Biventricular flow components assessed with 4-dimensional flow cardiac magnetic resonance in patients with pulmonary hypertension1Radiology, China-Japan Friendship Hospital, Beijing, China, 2Department of Pulmonary and Critical Care Medicine, China-Japan Friendship Hospital, Beijing, China, 3Siemens Shenzhen Magnetic Resonance Ltd, Siemens Shenzhen Magnetic Resonance Ltd, Shen Zhen, China, 4Siemens Medical Solution, Siemens Medical Solution, Chicago, IL, United States, 5Department of Cardiovascular surgery, China-Japan Friendship Hospital, Beijing, China
Synopsis
Using 4D FLOW CMR, flow components including percent of direct flow (PDF), retained inflow (PRI), delayed ejection flow (PDE) and residual volume (PRV) of bi-ventricles in patients with PH were quantified. Compared with non-PH patients, flow components had significantly alterations. RV PDF and PRV significantly correlated with RVEDV, RSV, RVEF and RV mass as well as NT-proBNP. Moreover, RV PDF and PVR correlated with pulmonary artery pressure and PVR. We think that 4D flow CMR may become a powerful surrogate for the future PH studies
Introduction
Previous studies( 1-3) have developed and applied 4-dimensional flow cardiac magnetic resonance imaging (4D flow CMR) for the evaluation of cardiovascular hemodynamics, but characteristics of ventricular flow components in patients with pulmonary hypertension (PH) remain unclear. The purpose of this study was to observe the alterations of biventricular blood flow components assessed with 4D flow CMR in patients with PH and to investigate the correlation of flow components with conventional CMR functional parameters (end-systolic and end-diastolic volume, ejection fraction) and the hemodynamics including pulmonary arterial pressure(PAP), pulmonary vascular resistance (PVR) measured via right heart catheterization.Methods
We prospectively enrolled 126 patients (105 patients with PH and 21 patients without PH, age 47±13 years, F/M=64/62) that had been referred to evaluate PH with right heart catheterization and CMR within 1 week. CMR imaging was performed on a 1.5 T clinical scanner (MAGNETOM Area, Siemens Healthcare, Erlangen, Germany). Standard Cine images were acquired for the calculation of right ventricle (RV) and left ventricle (LV) end-diastolic and end-systolic volumes (RVEDV, RVESV, LVEDV, LVESV) and ejection fractions (RVEF, LVEF). 4D flow acquisitions were free breathing, using a retrospectively ECG triggered, respiratory navigator gated,3-dimensional, 3-directional, time-resolved phase-contrast magnetic resonance imaging sequence with a 52-ms measurement temporal resolution and 2.4×2.4×2.8 mm3 voxel size, with velocity encoding 100 -150cm/s. Then the percentages of direct flow (PDF), retained inflow (PRI), delayed ejection flow (PDE) and residual volume (PRV) of two ventricles were quantified by using cmr42 (Circle Cardiovascular Imaging Inc, Calgary, Canada). The ventricular flow components, correlation with conventional cardiac functional parameters, blood NT-proB-type Natriuretic Peptide (NT-proBNP) and hemodynamics were analyzedResults
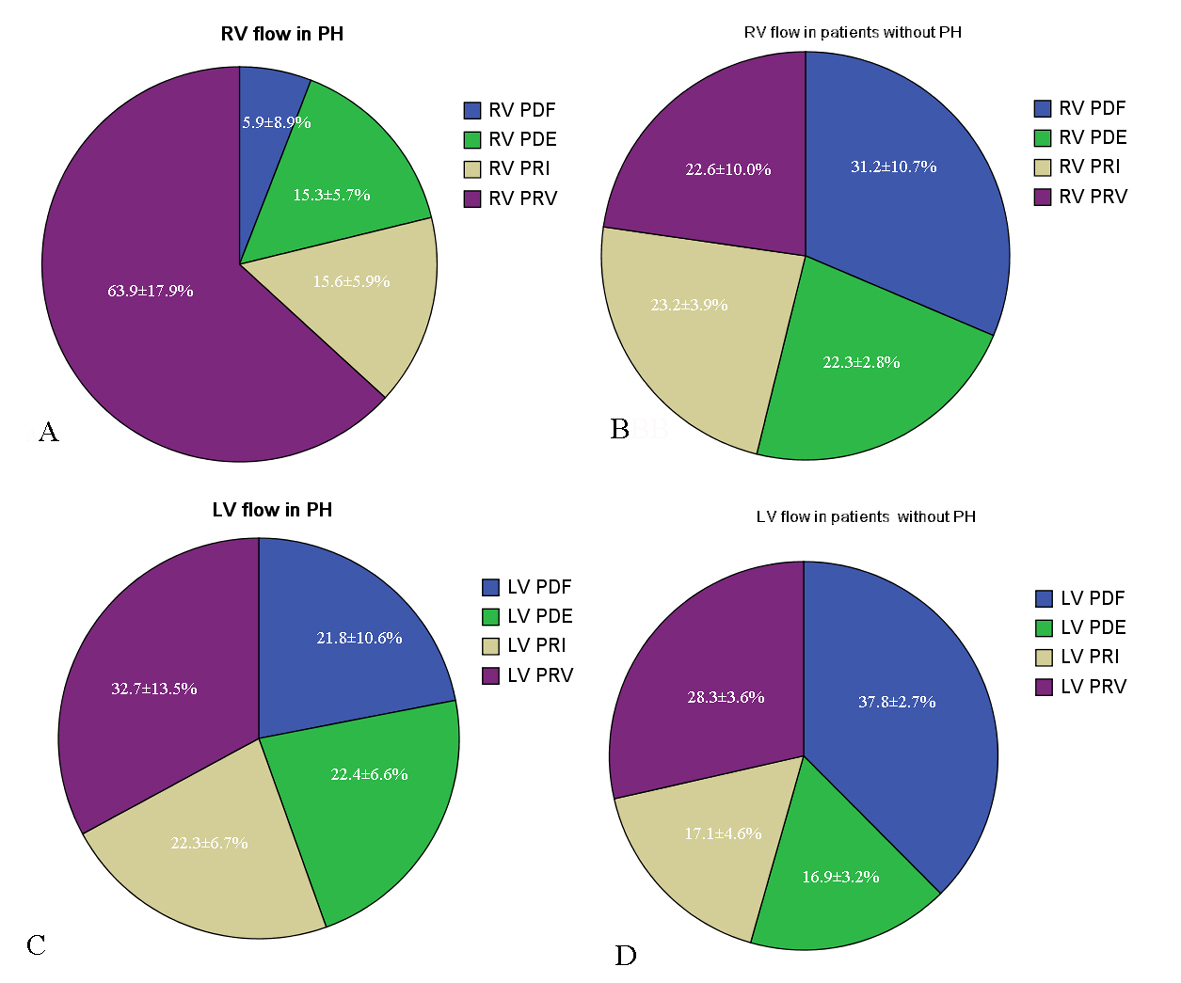
The proportion of RV and LV flow components in patients with and without PH were shown in Figure 1. Compared with non-PH patients, right ventricular (RV) PDF, PDE, PRI, and left ventricular (LV) PDF significantly decreased while RV PRV, LV PDE, and PRI increased. RV PDF, PDE, PRI, and PRV were significantly correlated with RVEDV, RSV, RVEF, and RV mass, as well as NT-proBNP. RV PDF negatively correlated with pulmonary arterial pressure and PVR, while PRV was positively correlated with pulmonary arterial pressure and PVR. When the RV PDF was less than 11%, the sensitivity and specificity of PDF for predicting PH were 88.6% and 98.7%, respectively, with an AUC of 0.95±0.02. When the RV PRV was greater than 42%, the sensitivity and specificity of PDF for predicting PH was 85.7% and 98.9%, respectively, with an AUC of 0.95±0.01(Figure 2).Conclusions
Bi-ventricular flow components analysis with 4D FLOW CMR could provide valuable information about disease severity and cardiac remodeling over conventional imaging parameters in PH.Acknowledgements
This
work is supported by National Natural Science Foundation of China (81871328),
Beijing Nature Science Foundation (7182149), China Medical Science and
Technology College Youth Medical Talent Award Program (2018RC320013)
References
1. Wheaton AJ, Miyazaki M.Four-dimensional Flow MRI: Principles and Cardiovascular Applications. J Magn Reson Imaging. 2012; 36:286-304.
2. Kamphuis VP, Westenberg JJM, van der Palen RLF, et al. Unravelling cardiovascular disease using four dimensional flow cardiovascular magnetic resonance. Int J Cardiovasc Imaging. 2017; 33:1069-1081.
3. Odagiri K, Inui N, Hakamata A, et al. Non-invasive evaluation of pulmonary arterial blood flow and wall shear stress in pulmonary arterial hypertension with 3D phase contrast magnetic resonance imaging. Springerplus. 2016;5:1071.
Figures