2264
Flow measurement with time of flight (TOF) in patients undergoing carotid revascularization: A comparison with arterial spin labeling (ASL)1Radiology, University of Washington, Seattle, WA, United States, 2Electrical and computer engineering, University of Washington, Seattle, WA, United States, 3Biomedical Engineering, University of Arizona, Tuscon, AZ, United States, 4Surgery, University of Washington, Seattle, WA, United States, 5Surgery, University of Arizona, Tuscon, AZ, United States
Synopsis
In this study, we assessed the potential of using vasculature features extracted from TOF images as surrogate markers of intracranial blood flow in patients undergoing carotid revascularization surgery and MR imaging prior to, within 48 hours after and 6 months after surgery. The intracranial vasculature features, including total volume, total length and total number of branches etc., on TOF images were extracted using a novel tool named iCafe, and then compared with arterial spin labeling (ASL) cerebral blood flow (CBF) measurement. The results show that TOF-iCafe vasculature features have similar behaviors as ASL CBF over the time points.
Introduction
Time of flight (TOF) images are routinely used for assessment of large vessel diseases. However, from the perspective of imaging mechanism, TOF is sensitive to blood flow, which is usually manifested as the visibility or intensity of distal smaller-size vessels. We have developed a tool named iCafe [1] to extract the intracranial vasculature based on TOF images, and showed that the derived vasculature features can reflect the age-related flow change [2]. Previously, we also performed a preliminary analysis of the change of TOF-iCafe features over multiple time points on a cohort of patients undergoing carotid revascularization surgery [3]. In this abstract, the TOF-iCafe results based on an expanded sample size were shown. Besides, we also further compared the TOF-iCafe features with arterial spin labeling (ASL) flow measurement.Methods
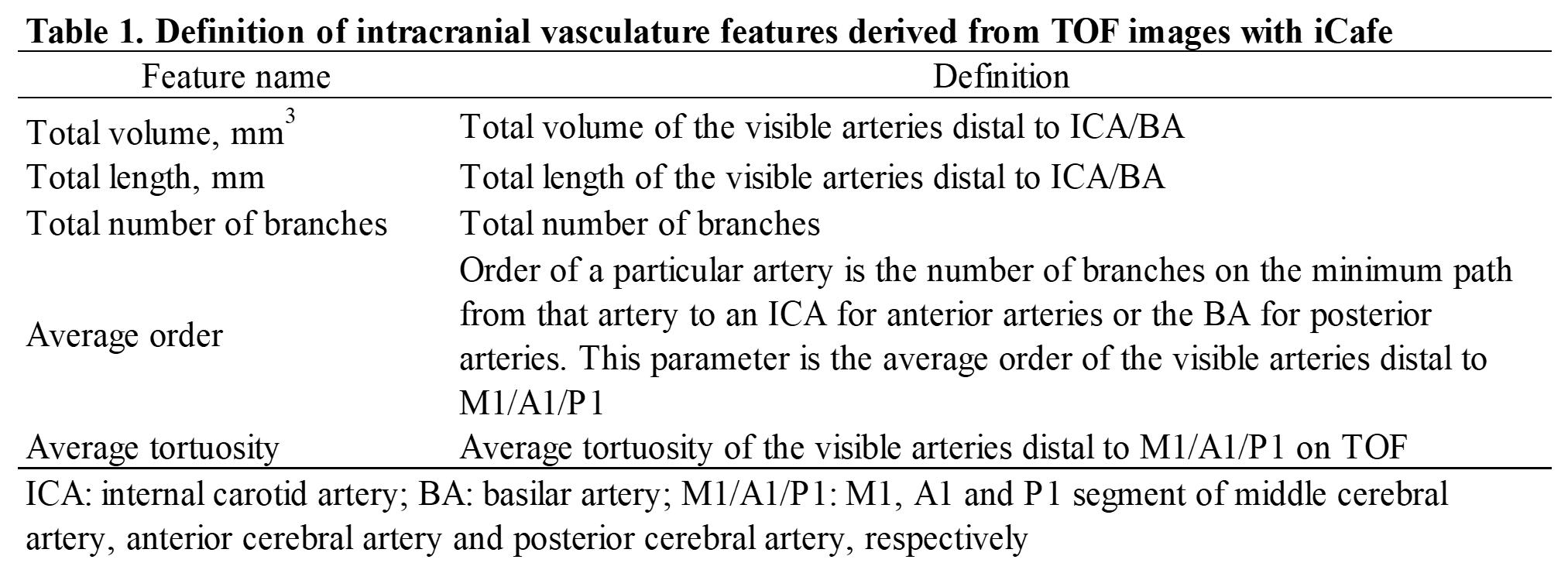
Patients: This study retrospectively analyzed MR images of veterans who underwent carotid interventions (carotid endarterectomy or carotid stenting) at a Veterans Medical Center from 2011 to 2017. MR imaging: MR imaging, including 3D whole-brain pseudocontinuous ASL and 3D TOF, were performed with a 3T MR scanner (Discovery MR750, GE Healthcare) at three time points: prior to surgery (dubbed as time point 1, i.e. TP1), within 48 hours after surgery (TP2) and 6 months after surgery (TP3). Imaging parameters for ASL were: labeling duration 1450 ms, postlabeling delay 2525 ms, FOV 240×240 mm, spiral trajectory with 6-8 arms, slice thickness 4-5 mm, number of average 3-4. Imaging parameters for TOF were: TR 2.2-2.3 ms, TE 2.6-2.9 ms, FA 15°, in plane FOV 220-260 mm, through plane FOV 83-128 mm, in plane voxel size 0.74-0.86 mm, slice thickness 1.4 mm. Image review: Co-registration of images was performed between time points using SPM toolbox (https://www.fil.ion.ucl.ac.uk/spm/software/spm12/). The TOF images were cropped to achieve the same coverage across all time points, and then reviewed with iCafe to extract the intracranial vasculature features, including total length, total volume, total number of branches, average order and average tortuosity (See Table 1 for detailed definition). Cerebral blood flow (CBF) quantification was performed using the recommended hemodynamic model [4]. The CBF map of each ASL scan was reviewed independently and blinded to clinical information and TOF image review to determine the presence of labeling failure in either internal carotid artery, according to the presence of whole-hemisphere low perfusion compared to the contralateral side. Only ASL scans with good labeling in both sides were included for the final analyses. Statistics: Not all subjects had three time points of TOF and ASL. In order to maximize sample size, we included all usable data with 2 time points for comparison. By doing this, the sample size will differ between the statistical analyses. Wilcoxon signed-rank test was performed to compare the iCafe features or CBF between time points. Spearman correlation analysis was performed to test association between ASL CBF and iCafe features for each time point. P value <0.05 was considered statistically significant.Results
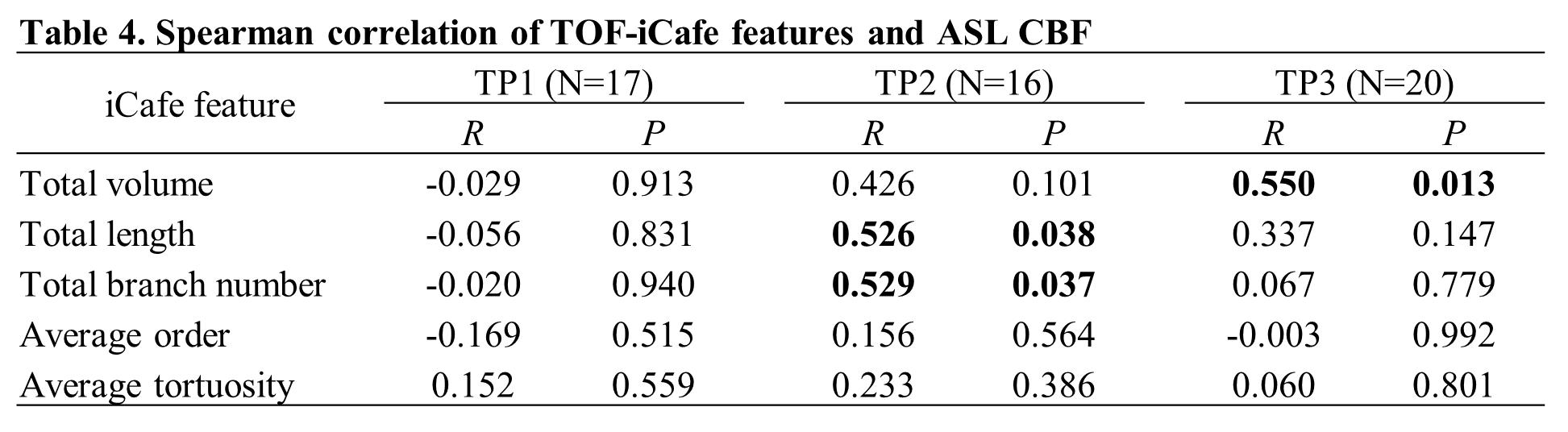
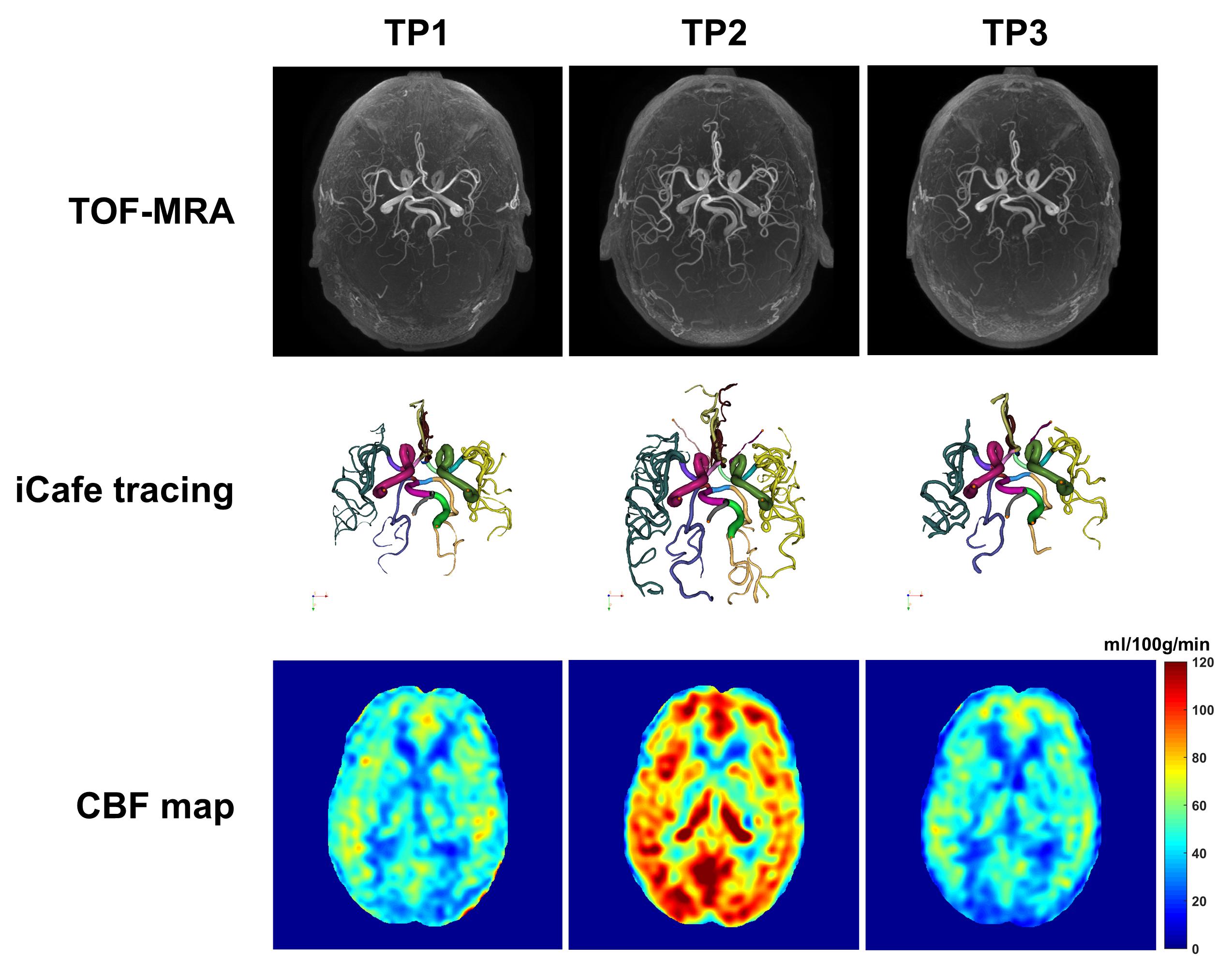
A total of 105 subjects (102 males, 69.4±7.6 years) were included. A large proportion of ASL scans demonstrated labeling failure, with 16.0% (8/50) scans in TP1, 23.9% (17/71) in TP2, and 26.0% (13/50) in TP3. Both CBF (Table 2) and iCafe features (Table 3) show a dramatic increase (or decrease) from TP1 to TP2, followed by a decrease (or increase) in TP3. However, for both CBF and iCafe features, TP3 remains slightly larger (or smaller) than TP1. The iCafe features do not correlate with CBF in TP1, while the total length and total number of branches have moderate correlation with CBF in TP2, and total volume has moderate correlation with CBF in TP3 (Table 4). Figure 1 shows the TOF MRA images, iCafe tracing results and CBF maps of an example case.Discussion and Conclusion
The results (Table 2-3) suggest that iCafe features derived from TOF have similar behaviors as ASL CBF in terms of characterizing the flow change induced by carotid revascularization surgery, implying the feasibility of iCafe features as surrogate markers of cerebral blood flow, especially when a real flow imaging is not available. The lack of statistically significant correlation between iCafe features and CBF at TP1 may be explained by the limited sample size and narrow data spread (i.e. the CBF values are clustered). In this population, we also noted that TOF imaging is more robust than ASL, in that ASL was susceptible to labeling efficiency decrease caused by presence of a carotid stent or large velocity disturbance.Acknowledgements
This research is supported by grants from the National Institutes of Health (R01NS070308).References
1. Chen, L., et al., Development of a quantitative intracranial vascular features extraction tool on 3D MRA using semiautomated open-curve active contour vessel tracing. Magn Reson Med, 2018. 79(6): p. 3229-3238.
2. Chen, L., et al., Quantitative assessment of the intracranial vasculature in an older adult population using iCafe. Neurobiol Aging, 2019. 79: p. 59-65.
3. Shirakawa, M., et al. Quantitative assessment of cerebrovascular structure after carotid revascularization using intraCranial Artery Feature Extraction (iCafe) Technique. in Proceedings of the 27th Annual Meeting of ISMRM. 2019. Montreal, QC, Canada.
4. Alsop, D.C., et al., Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med, 2015. 73(1): p. 102-116.
Figures