2250
A pilot investigation into the use of a high-performance 0.55T scanner in CMR late gadolinium enhancement imaging of myocardial infarction1NATIONAL INSTITUTES OF HEALTH/NHLBI, BETHESDA, MD, United States
Synopsis
We demonstrate the diagnostic capabilities of a high-performance, low-field (0.55 Tesla) scanner in the acquisition and interpretation of late gadolinium enhancement (LGE) in patients referred for assessment of myocardial infarction (MI). Patients underwent paired comparison exams with breath-held gradient echo LGE imaging at 1.5T and breath-held bSSFP LGE imaging at 0.55T. The number of enhancing segments identified between each field strength was similar (59 segments at 0.55T vs 63 segments at 1.5T), and assessment of epicardial coronary artery distribution matched exactly between the two field strengths; included were two multi-vessel disease cases.
Background
The use of higher field strengths for higher signal-to-noise is attractive for magnetic resonance imaging of some organ systems. However, for the heart, higher field strengths are also associated with more artifact; additionally, there is an increased financial expense for high field strength imaging. Recently, there has been renewed interest in low-field cardiovascular magnetic resonance (CMR)1. Our group has demonstrated that a lower field strength, paired with high-performance hardware and contemporary imaging software, may be well suited to cardiac imaging2. This approach could offer reduced cost and increased accessibility of CMR. In the current study, we sought to evaluate the diagnostic capabilities of a high-performance, low-field (0.55 Tesla) scanner in the acquisition and interpretation of late gadolinium enhancement in patients referred for clinically known or suspected myocardial infarction (MI).Methods
This imaging study was approved by our local Institutional Review Board. Patients referred for clinical imaging on a 1.5 T MRI scanner (MAGNETOM Aera, Siemens, Erlangen, Germany) to assess for known or suspected myocardial infarction also underwent comparison imaging on our high-performance 0.55 T system (prototype MAGNETOM Aera, Siemens, Erlangen, Germany). Gadobutrol (Gadavist, Bayer, Leverkusen, Germany) was administered intravenously (0.15 mmol/kg) and late gadolinium enhancement imaging was performed at 10 minutes post-contrast administration. The LGE sequences were selected and optimized for each individual field strength.1.5T imaging: Standard short-axis and three long axis LGE images were acquired using a phase sensitive inversion recovery (PSIR)3 spoiled gradient recalled echo sequence. The typical parameters were a matrix size of 256 × 144, 8 mm slice thickness, TI individualized to null the myocardium, TE 3.17 ms, Echo spacing 8.2 ms, bandwidth of 140 Hz/pixel, and an excitation flip angle of 25°. PSIR LGE was a breath-held, ECG triggered, segmented acquisition with inversions every 2 R-R intervals, acquiring a proton density (PD) weighted image on alternate heartbeats. Typical segmentation was 25 phase encode lines per heartbeat at a nominal 60 beats per minute heart rate, corresponding to a breath-hold duration of 10 heartbeats including 2 discarded beats.
0.55T imaging: On a separate day, the research CMR scan was performed on the 0.55T scanner using the same contrast dose. The low-field LGE images were acquired using a breath-held (PSIR) steady-state free precession sequence. The typical parameters were a matrix size of 256 × 159, 8 mm slice thickness, TI individualized to null the myocardium, TE 1.9 ms, Echo spacing 4.88 ms, bandwidth of 250Hz/pixel, and an excitation flip angle of 120°. PSIR LGE was a breath-held, ECG triggered, segmented acquisition with inversions every 2 R-R intervals, acquiring a proton density (PD) weighted image on alternate heartbeats. Typical segmentation was 53 phase encode lines over 14 heartbeats.
Image analysis: LGE images were randomized and blinded prior to interpretation by an experienced cardiologist. Scoring consisted of the identification of abnormal LGE consistent with MI with an additional grading of the coronary distribution (left anterior descending artery, right coronary artery, left circumflex artery) whether the MI was <50% transmural extent (subendocardial) versus >50% of the transmural extent (labelled as transmural). Interpretation was performed using a 17-segment model, with interpretation blinded to clinical data. Scoring of matched subjects was separated by >1 week to avoid memory bias.
Results
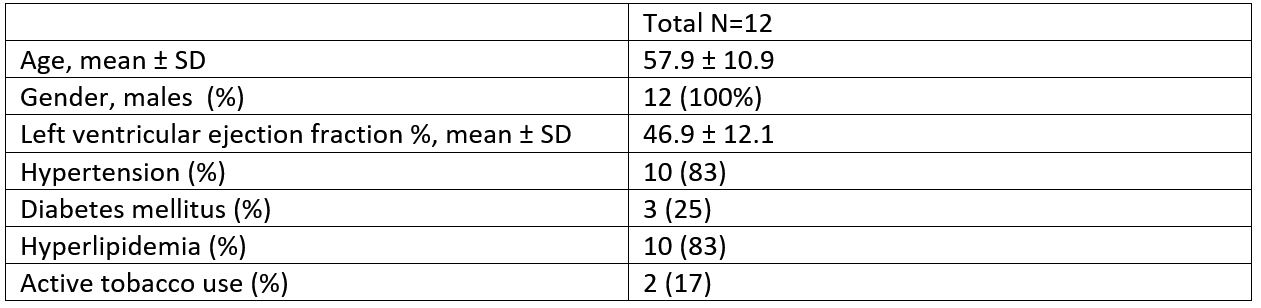
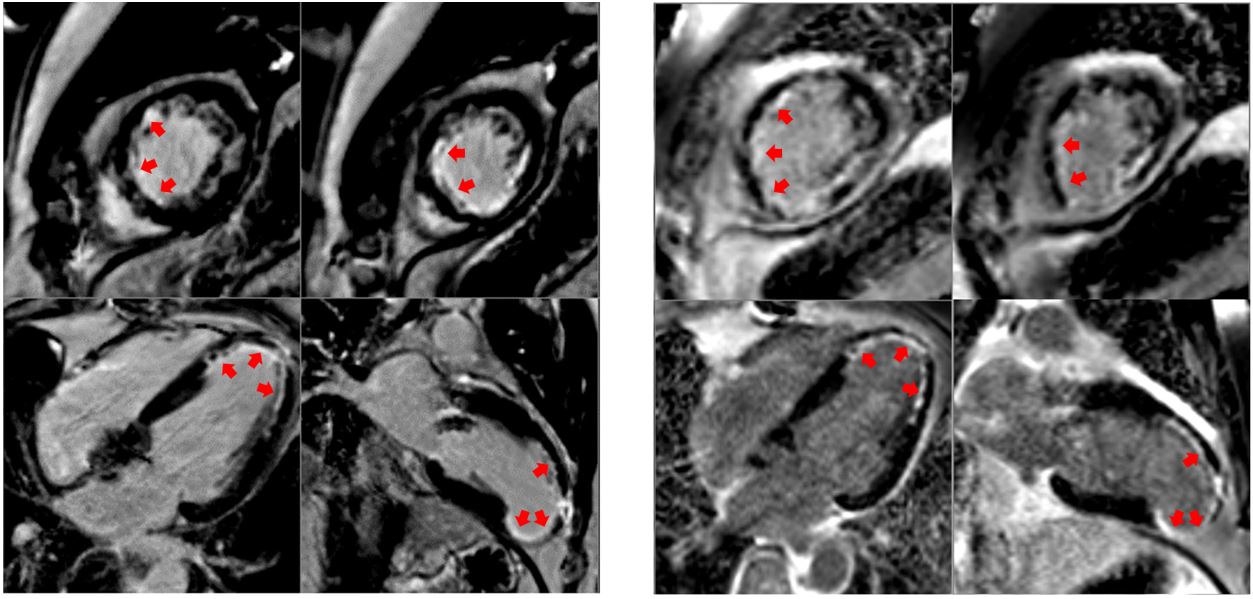
Thirteen patients were enrolled and participated in the comparison study, with mean time between scans of 44.9 ± 36 days. One study performed on the low-field scanner was deemed uninterpretable due to a hardware malfunction; therefore the presented data includes 12 subjects. Baseline characteristics are presented in Table 1.Figure 1 demonstrates a sample comparison between the clinical 1.5T scan and the research 0.55T scan in a patient with a left anterior descending artery MI. Note that the susceptibility artifact from a prosthetic aortic valve appears more prominent on the 1.5T image
Overall, the number of segments identified between each field strength was similar with the 0.55T scanner identifying a total of 59 segments with MI (50 subendocardial, 9 transmural) and the 1.5T scanner identifying a total of 63 segments with MI (53 subendocardial, 10 transmural). Assessment of epicardial coronary artery distribution matched exactly between the two field strengths; included were two multi-vessel disease cases.
Discussion
While low-field imaging is promising for CMR, the implementation and clinical evaluation of commonly used CMR techniques is still underway. In our original paper2, we reported that the relaxivity of gadobutrol was comparable between 0.55T and 1.5T field strengths, so we were able to use a comparable dose of contrast with reasonable results. We compared optimal protocols at each field strength, which were breath-held gradient echo (1.5T) and bSSFP (0.55T), for a best-to-best comparison of diagnostic ability. Future work will include the optimization of free-breathing acquisition methods. Our pilot investigation demonstrates that demanding imaging techniques such as late gadolinium enhancement imaging are feasible at 0.55T.Acknowledgements
We would like to acknowledge the assistance of Siemens Healthcare in the modification of the MRI system for operation at 0.55T under an existing cooperative research agreement (CRADA) between NHLBI and Siemens Healthcare.References
1. Simonetti OP, Ahmad R. Low-Field Cardiac Magnetic Resonance Imaging: A Compelling Case for Cardiac Magnetic Resonance's Future. Circ Cardiovasc Imaging 2017;10.
2. Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology 2019;293:384-93.
3. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med 2002;47:372-83.
Figures