2213
Intra-cardiac flow kinetic energy assessment from 4D flow CMR imaging in pediatric and adult repaired Tetralogy of Fallot1National Heart Centre Singapore, Singapore, Singapore, 2Shanghai Children’s Medical Centre, Shanghai Jiaotong University School of Medicine, ShangHai, China, 3Duke-NUS Medical School, Singapore, Singapore, 4National University Hospital Singapore, Singapore, Singapore, 5KK Women’s and Children’s Hospital, Singapore, Singapore, 6Philips Germany, Humburg, Germany, 7Department of Radiology, Leiden University Medical Center, Leiden, Netherlands
Synopsis
Whole-heart 4D cardiovascular magnetic resonance (CMR) phase-contrast flow measurement enables qualitative and quantitative assessment of intra-cardiac flow. Its feasibility was investigated in 12 pediatric and 13 adult patients with repaired Tetralogy of Fallot (rTOF). Left ventricular (LV) kinetic energy (KE) and pathline-derived flow components were analyzed. KE parameters were significantly correlated with age, but only LV systolic KE remained significantly different after indexing to LV end-diastolic volume. Pediatric rTOF patients had similar LV ejection fraction, indexed LV volumes and mass, but significantly reduced indexed LV systolic KE, retained inflow and increased delayed ejection flow compared with adults.
Introduction
Current whole-heart 4D cardiovascular magnetic resonance (CMR) phase-contrast flow measurement (4Dflow) yields qualitative and quantitative flow information without need for breath-holding or respiratory gating1. We performed 4Dflow in pediatric and adult patients with repaired Tetralogy of Fallot (rTOF) and compared left ventricular (LV) kinetic energy (KE) parameters and flow components.Methods
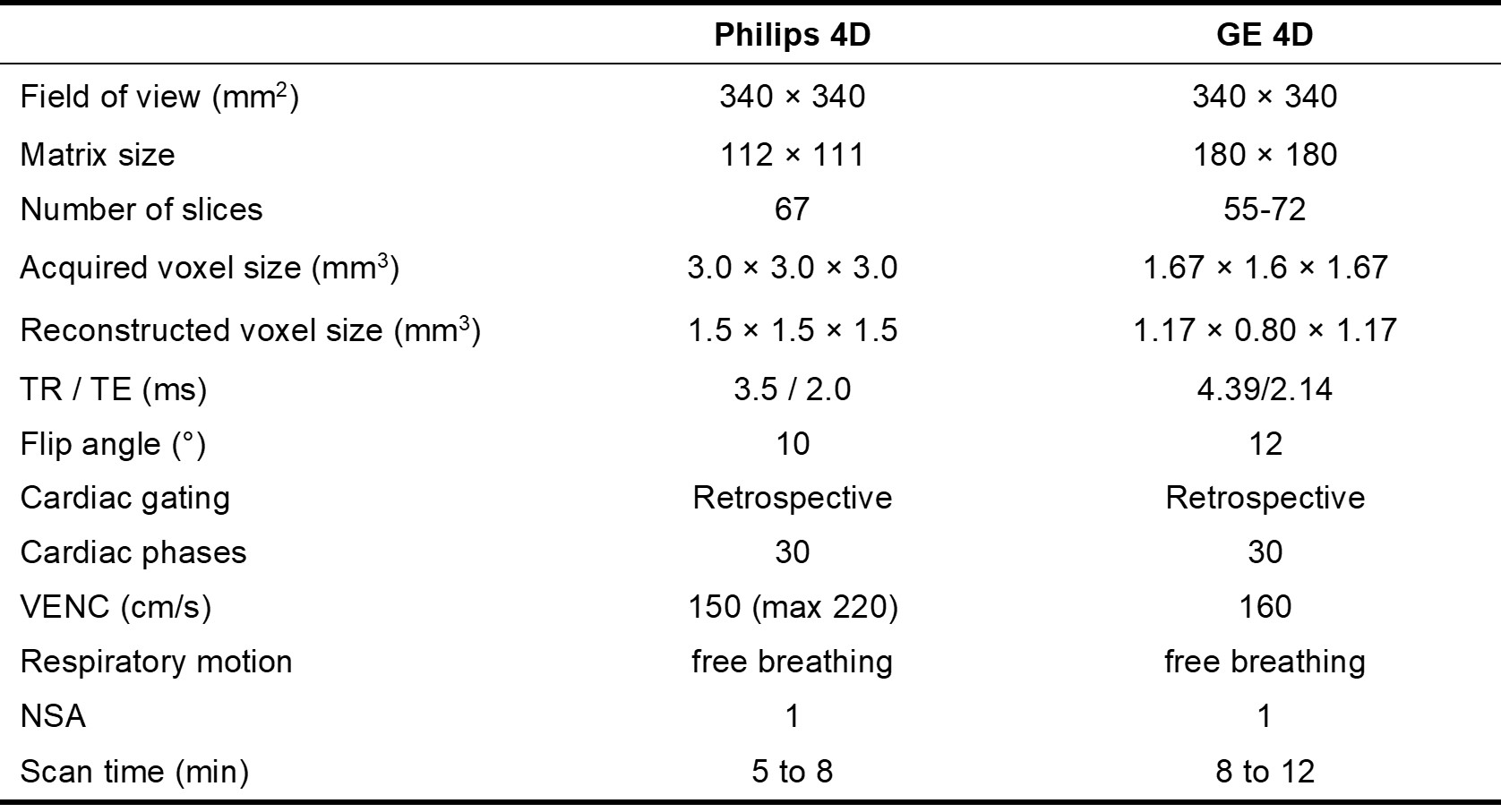
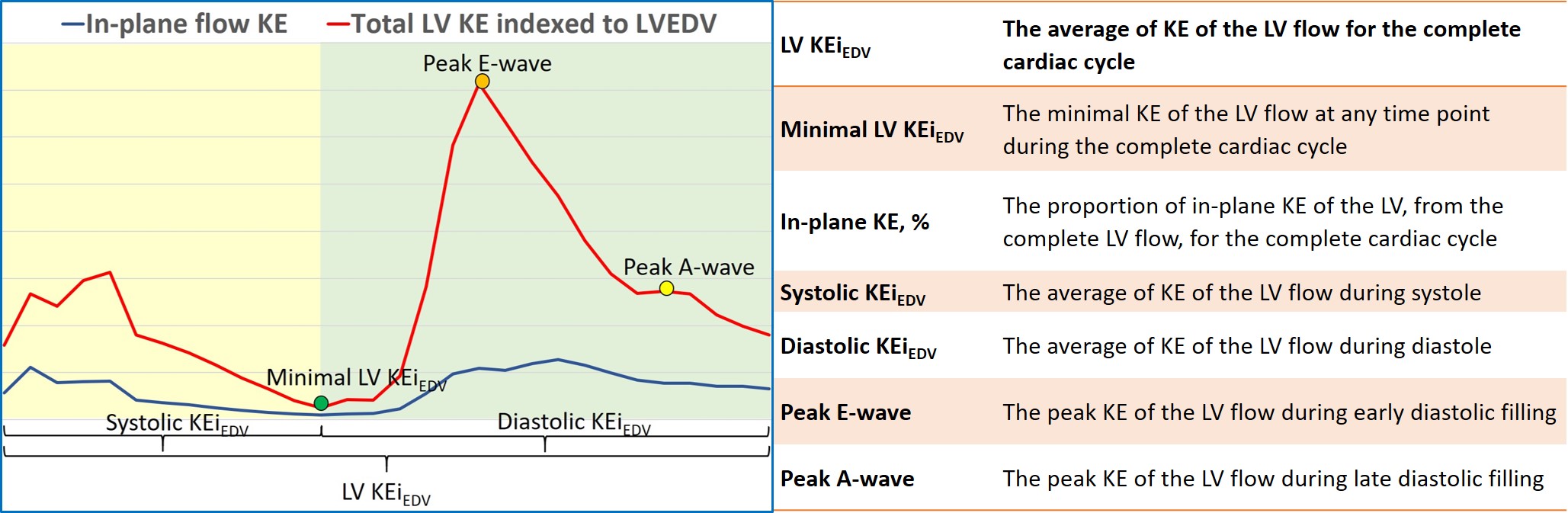
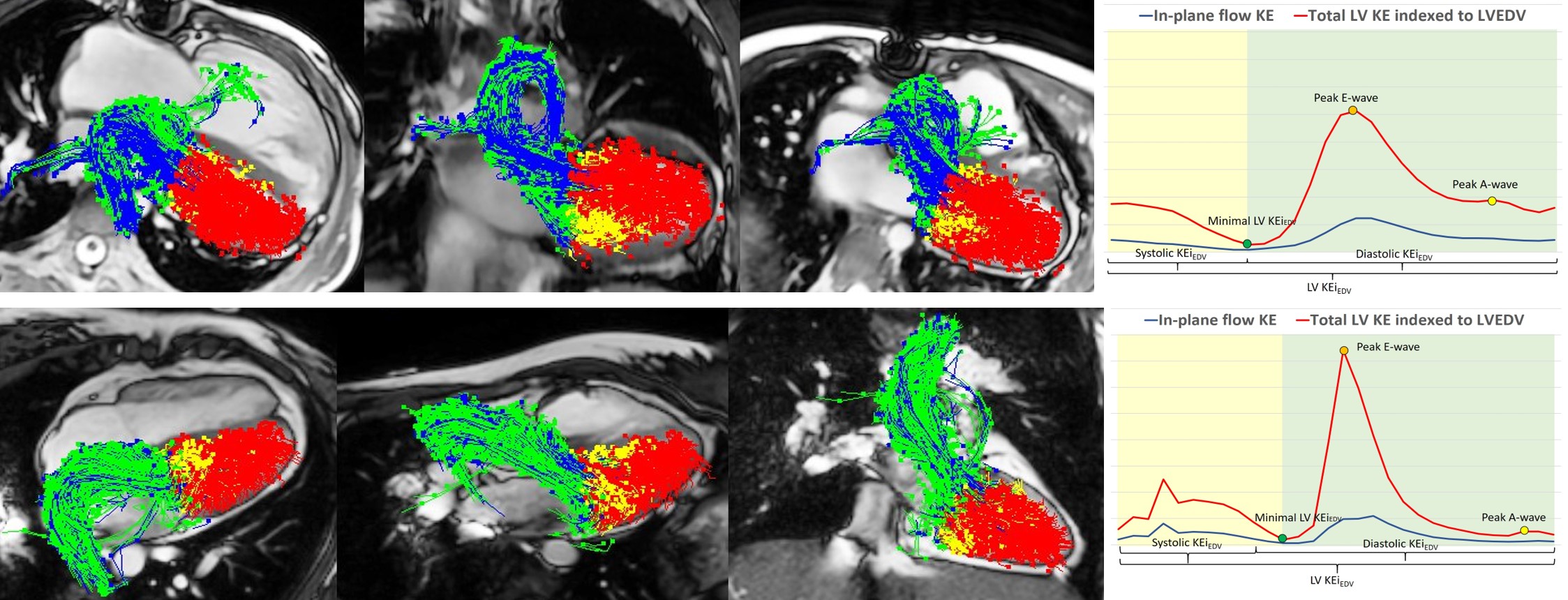
12 pediatric (8 ± 4 years) and 13 adult rTOF patients (28 ± 12 years) were recruited from two centers. Pediatric rTOF patients underwent 4Dflow on a 3T scanner (MR750, GE Healthcare, Waukesha) with k-t space broad-use linear acquisition speed-up technique (k-t BLAST) and adult rTOF patients on a 3T scanner (Philips Ingenia). Detailed imaging parameters are summarized in Figure 1, according to ISMRM recommendation2. Left ventricular (LV) blood flow was analyzed using MASS software (Leiden University Medical Center, Leiden, The Netherlands). For each voxel, kinetic energy (KE) was calculated as KE=1/2·ρblood·Vvoxel·v2, where ρblood is blood density (1.06 g/cm3); Vvoxel, voxel volume; and v, velocity magnitude. At each phase, total KE within the LV was obtained by summation of KE of all voxels. Additionally, time-resolved KE energy curves were generated to derive physiologically relevant parameters. LV blood flow KE parameters for the entire cardiac cycle are detailed in Figure 2. Additionally, individual pathlines were generated from velocity vectors for all voxels found within segmented LV endocardial borders. Depending on pathline trajectories within the LV during the analyzed single cardiac cycle, four flow components were discernible: (1) direct flow: blood that enters and exits the LV in the analyzed cardiac cycle; (2) retained inflow: enters but does not exit the LV during the analyzed cycle; (3) delayed ejection flow: starts within the LV and exits during the analyzed cycle; and (4) residual volume: blood that remains in the LV for at least two cardiac cycle. Each component was expressed as a proportion of LV end-diastolic volume. Examples of LV flow components at the end-systolic phase and LV KE curves for one pediatric and one adult rTOF are given in Figure 3. Statistical analysis was performed using SPSS 22, and P value <0.05 was considered significant.Results
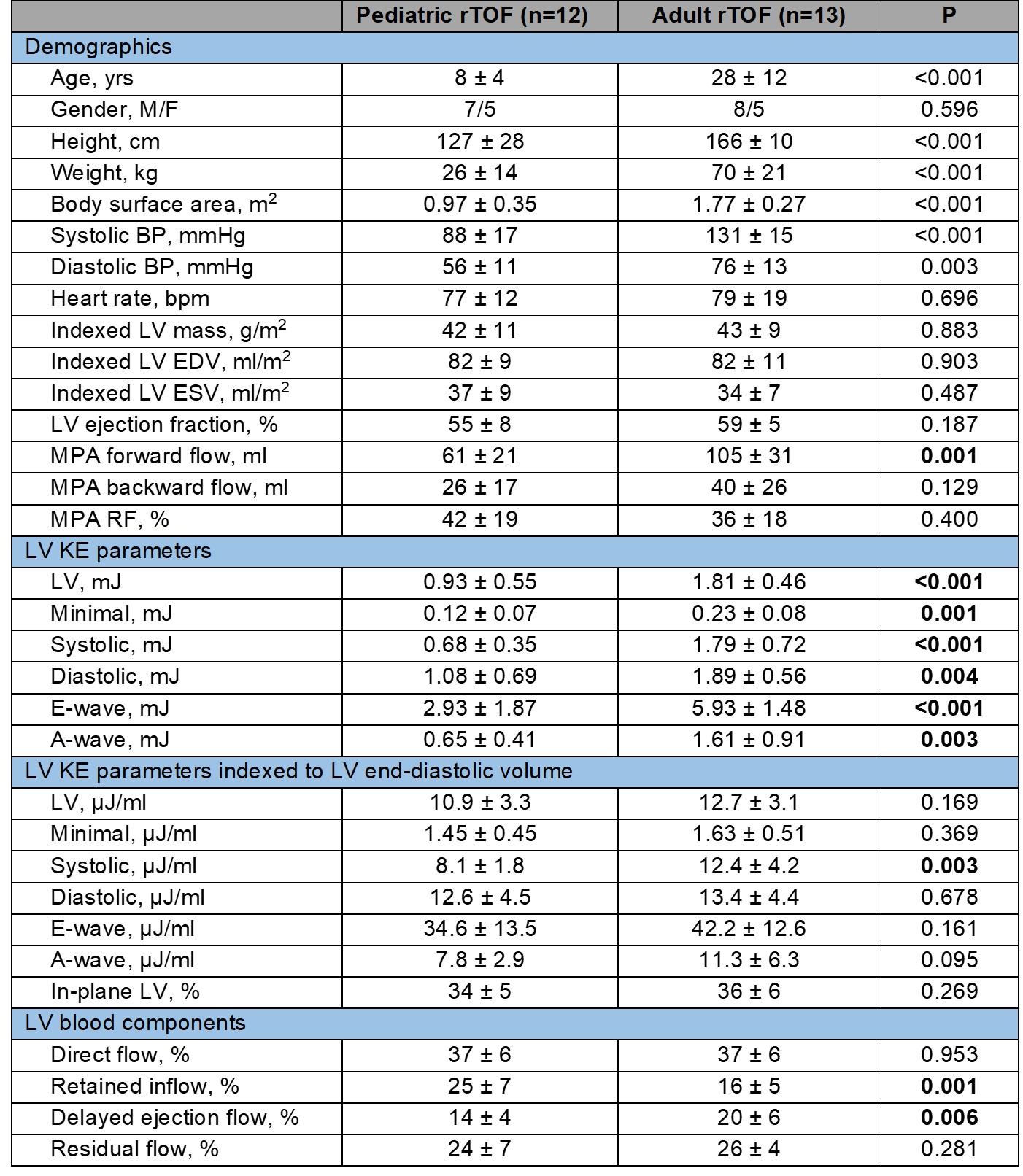
4Dflow and analysis were feasible in all subjects. Demographics and LV flow analysis parameters in pediatric and adult rTOF are tabulated in Figure 4. No significant difference was found for LV ejection fraction, indexed LV end-diastolic volume (EDV), end-systolic volume and LV mass. Pediatric rTOF group had significantly reduced LV KE, minimal KE, systolic KE, diastolic KE, peak E-wave and peak A-wave KEs (all P ≤0.004) versus adult rTOF, and the corresponding correlation coefficients with age were r=0.721, 0.674, 0.854, 0.567, 0.498 and 0.801, respectively. When these parameters were indexed to LVEDV, only systolic KE remained significantly different with significant association with age (r=0.776, P<0.01). Pediatric rTOF patients had significantly increased reduced retained inflow and delayed ejection flow compared with adult rTOF.Conclusion
Children with rTOF had similar LV ejection fraction, indexed LV volumes and mass, but significantly reduced LV systolic KE (indexed to LVEDV), retained inflow and increased delayed ejection flow compared with adult rTOF. 4Dflow is feasible in rTOF, and analysis of LV hemodynamics must consider effects of both age and LVEDV.Acknowledgements
This study received funding support from the National Medical Research Council (NMRC/OFIRG/0018/2016).References
1. Kanski M et al. BMC Medical Imaging (2015) 15:20.
2. Zhong L et al. J Magn Reson Imaging 2019;50:677-681.
Figures