2205
Evaluating the Vessel Wall Permeability of Abdominal Aortic Aneurysm using 3D DynamicContrastEnhancedMRI: a feasibility study1Radiology, Changhai hospital, Shanghai, China, 2Changhai hospital of Shanghai, Shanghai, China, 3UCSF, San Francisco, CA, United States
Synopsis
The feasibility of 3D DCE on AAA was demonstrated in our study.
Purpose:
This study aims to 1) investigate the feasibility of 3D dynamic contrastenhanced(DCE) MRI to evaluate the vessel wallpermeability of abdominal aortic aneurysm(AAA), and 2) assess the relationship between Ktrans and AAAdiameter/intraluminal thrombus (ILT).Methods:
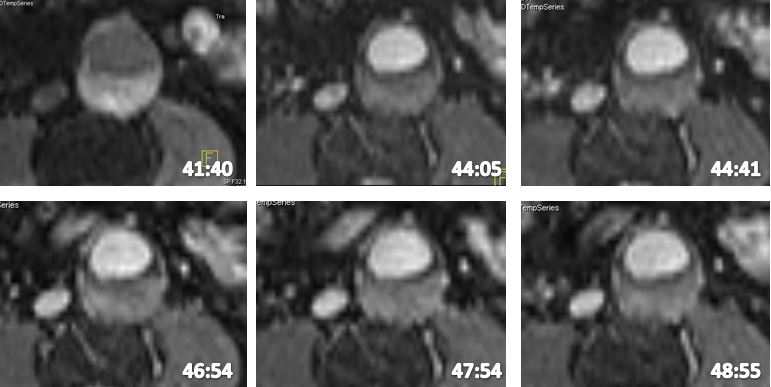
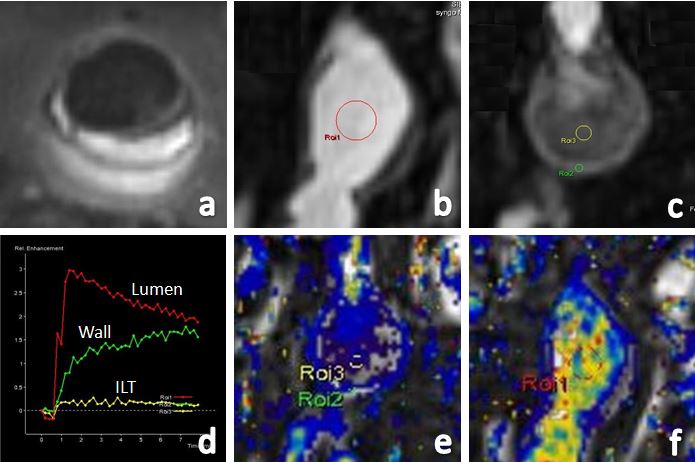
13 patients with AAAs (diameter 4.85 ± 0.94cm) were scanned on a 3T Siemens Skyra scanner. MRI was acquired using 1) apreviously developed 3D T1weightedblack blood fastspinechosequence [1]and 2) a 3D DCE sequence using fast gradientecho(VIBE). TR/TE: 6.30/2.90ms. 3mm slice thickness, 1.5mm inplaneresolution, 40 slices; temporal resolution 13s, a total of40 phases. AAA diameter was measured on black blood MRI images using our previous published method [1]. ILT thicknesswas measured on the transverse slice of maximal aneurysm diameter and maximal ILT diameter was used. Based on thevolume distribution of ILT on the black blood MRI, two types of ILT were divided into two types for patients with ILT: Type 1:Fresh ILT was present (high signal ILT >1.2 times of adjacent muscle); Type 2: Without fresh ILT (only old ILT was present). 3DDCE MRI images were analyzed on the work station of the Siemens scanner using 4D Tissue software. ROIs were carefullydrawn on aneurysm wall and ILT (if present) of AAA and Ktrans was obtained for both aneurysm wall and ILT. Ktrans wasderived based on the previous published model [2] and the arterial input function was from the same scan. Spearman’s r wasused to evaluate the correlation of DCE Ktrans with AAA diameter and ILT thickness. MannWhitneytest was used to compareDCE Ktrans between aneurysm wall and ILT. DCE Ktrans differences were also investigated as a function of ILT types (withfresh ILT and without fresh ILT).Results:
11/13 patients were found to have ILT (Type1:8 and Type2:3) and [3/13 patients’ AAA diameter was ≥5.5cm.] There was apositive correlation between Ktrans and AAA diameter (r=0.57;P=0.01). A relatively weak, nonsignificantnegative correlationwas found between Ktrans and ILT thickness (r=0.32;P=0.34). DCE Ktrans of aneurysm wall [0.11(0.05,0.18) min1]wassignificantly higher than that of ILT [0.04(0.02,0.05) min1](P=0.01). There was no significant difference of DCE Ktrans betweendifferent types of ILT (with fresh ILT [0.09(0.04,0.15) min1]vs. without ILT [0.14(0.06,0.18) min1],p=0.31).Discussion:
DCE has rarely been studied for AAA.Previous 2D DCE studies of AAAs had temporal resolution of 18s, and spatial resolution 1.6mm×1.6mm×6mm [2,3]. In ourstudy, we improved the temporal resolution to 13s, and spatial resolution to 1.5mm×1.5mm×3mm. In the past decade, it hasbeen shown that DCE MRI is able to quantify the microvasculature of the vessel wall in carotid arterial occlusive disease, andDCE parameters were correlated to clinical outcome and treatment effect [4,5]. Although AAA diameter is used for clinicalmanagement decisions, it has some limitations. From our study, we found Ktrans values of aneurysm wall was negativelycorrelated with AAA diameter. DCE may be another important method for evaluation of AAA risk but needs to be tested in alarger cohort of patients.ILT is a common feature in AAAs and has been studied as a potential marker of progressive AAA disease. Previous studiesshowed thick ILT can induce localized hypoxia and inflammation, and weaken the arterial wall. Although the presence of ILTmay indicate higher risk, the role of ILT thickness is still unclear. A recent study found that ILT thickness was smaller in rupturedAAAs than unruptured ones [6]. We also found no clear relationship between ILT thickness and Ktrans. Furthermore, anotherimportant finding was that the Ktrans value of aneurysm wall was significant higher than that of ILT. This agree with histologystudies that vasa vasorum is present in the adventia, but not present in ILT [7].
Previous studies also found AAAs with fresh ILT grew two times as fast as AAAs without fresh ILT [7]. However, there was nosignificant difference of DCE Ktrans between AAAs with different types of ILT in our study. The reason may be due to smallpatient numbers, and a further larger scale study is needed.
Conclusion:
3D DCE MRI can be used to evaluate the vessel wall permeability of AAA with high temporal and spatial resolution.Acknowledgements
NoneReferences
[1] Zhu C, Tian B, Leach JR, et al. Noncontrast3D black blood MRI for abdominal aortic aneurysm surveillance comparisonwith CT angiography. Eur Radiol. 2017;27(5):17871794.doi: 10.1007/s0033001645590.
[2] Nguyen VL, Backes WH, Kooi ME, et al. Quantification of Abdominal Aortic Aneurysm Wall Enhancement With DynamicContrastEnhancedMRI: Feasibility, Reproducibility, and Initial Experience. J Magn Reson Imaging. 2014;39(6):144956.doi:10.1002/jmri.24302.
[3] Nguyen VL, Kooi ME, Backes WH, van Hoof RH, et al. Suitability of Pharmacokinetic Models for Dynamic ContrastEnhancedMRI of Abdominal Aortic Aneurysm Vessel Wall: A Comparison. PLoS One. 2013;8(10):e75173. doi:10.1371/journal.pone.0075173.
[4] Wang J, Chen H, Sun J, et al. Dynamic contrastenhancedMR imaging of carotid vasa vasorum in relation to coronary andcerebrovascular events. Atherosclerosis. 2017;263:420426.doi: 10.1016/j.atherosclerosis.
[5] Dong L, Kerwin WS, Chen H, et al. Carotid Artery Atherosclerosis: Effect of Intensive Lipid Therapy on the Vasa VasorumEvaluationby Using Dynamic ContrastenhancedMR Imaging. Radiology. 2011;260(1):22431.doi: 10.1148/radiol.11101264.
[6] Siika A, Lindquist Liljeqvist M, Hultgren R, et al. Aortic Lumen Area Is Increased in Ruptured Abdominal Aortic Aneurysmsand Correlates to Biomechanical Rupture Risk. J Endovasc Ther. 2018:1526602818808292. doi:10.1177/1526602818808292.
[7] Nguyen VL, Leiner T, Hellenthal FA et al. Abdominal aortic aneurysms with high thrombus signal intensity on magneticresonance imaging are associated with high growth rate. Eur J Vasc Endovasc Surg, 2014;48:676684.
Figures