2202
Inflow inversion recovery of transplant renal artery stenosis: a validation study1radiology, the second hospital of shandong university, Jinan, China, 2GE Healthcare, MR Research China, Beijing, China
Synopsis
Transplant renal artery stenosis(TRAS) was frequently occurred among patients after renal transplantation. The main goal of this study was to evaluate the feasibility of inflow inversion recovery (IFIR) technique in the assessment of TRAS by using digital subtraction angiography(DSA) as a reference. We measured the stenosis degrees of transplant renal arteries with IFIR and DSA, respectively. We obtained a strong correlation between IFIR and DSA, and no significant difference was found between these two techniques. Therefore, IFIR can been demonstrated as a noninvasive, accurate and valuable method in the diagnosis and evaluation of TRAS.
Transplant renal artery stenosis(TRAS) was frequently occurred among patients after renal transplantation. Most TRAS cases are prone to progress to transplant renal loss, which however remains difficult to detect because of its nonspecific clinical manifestations. So, an early and accurate diagnosis of TRAS is essential. Digital subtraction angiography (DSA) is considered the gold standard for TRAS examination. However, DSA is an invasive and expensive procedure, and requires the use of nephrotoxic-iodinated contrast media. Alternatively, inflow inversion recovery (IFIR), as a novel magnetic resonance imaging technology, is gradually applied to assess artery stenosis for transplant renal [1]. This technique does not require the usage of contrast agent and can thus avoid kidney injury effectively. Moreover, short examination time of this technique also allows for repeated applications in the follow-up examinations. With this technique, some researchers have evaluated renal artery stenosis. Highly comparable performance was found by comparing with DSA [2]. However, it remains unknown if this technique is also feasible for evaluating renal artery stenosis after transplantation. The main goal of this study was to evaluate the feasibility of IFIR technique in the assessment of TRAS by using DSA as a reference.
Materials and Methods
Subjects
165 patients(158 men and 37 women; median age 43 years old) performed with IFIRs between January 1, 2015 and December 31, 2018 were retrospectively reviewed for the assessment of transplant renal artery stenosis. Twenty-seven patients were performed with DSA after IFIR.
MRI and DSA examination
All IFIR measurements were performed at a 3.0T whole-body scanner(GE Discovery 750, Milwaukee, WI, USA) with a standard 8-channel phased-array body coil. The IFIR imaging, based on the fast imaging employing steady-state acquisition(FIESTA) sequence, was added into this clinical protocol after anatomical scanning and was carried out in the axial plane. The imaging sequence was performed with breath-hold. The scan parameters were applied as follows: echo time (TE) 1.5 ms, repetition time (TR) 3.10 ms, flip angle 60°, receiver bandwidth 125 Hz/pixel; field of view (FOV)340x255 mm for covering both kidneys, slice thickness 2.4 mm, number of slices 32, matrix size = 224 x 160 and number of excitations 1. The acquisition time was 10-12 seconds. DSA was performed with a GE DSA system (Innova; GE Healthcare, Waukesha, Wis).
Data analysis
The IFIR images were judged to be of excellent, good, moderate, and not diagnostic. Each transplant renal artery of patients was divided into four grades, i.e., grade 1(0-24%), grade 2(25-49%), grade 3(50-74%), and grade 4(75-100%) according to the stenosis degree of artery. All statistical analyzes were performed in SPSS 17.0 software (SPSS Inc., Chicago, IL, USA). Non-parametric Wilcoxon signed-rank test was used to compare IFIR with DSA images. In addition, the Spearman correlation analysis was used to estimate the relationship between IFIR and DSA measurements. Significance threshold was set as p<0.05.
Results
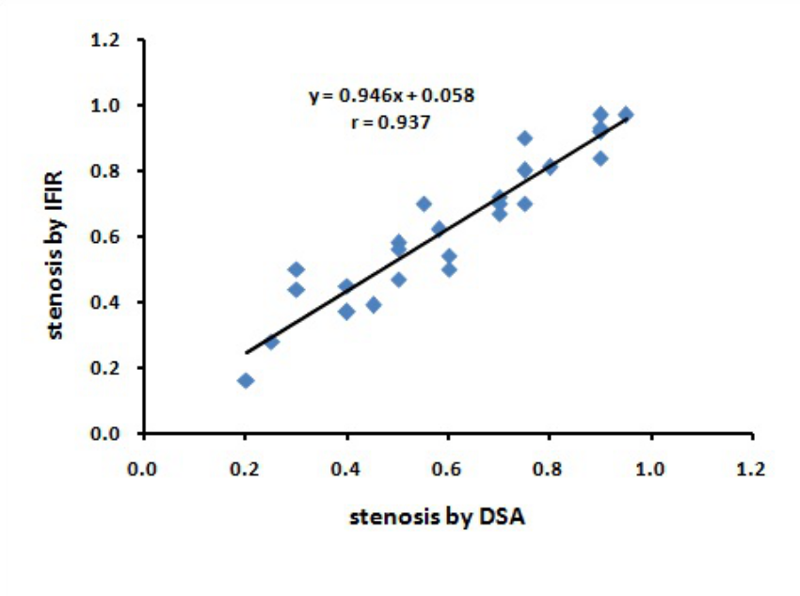
Our study included 165 patients which collectively had images of 195 transplant renal arteries. Of these, 100 arteries were found with TRAS and the rest 95 were not. The IFIR images for 194/195 (99.5 %) arteries were judged to be of excellent, good, and moderate-quality(Table1).Twenty-seven patients had undergone DSA measurements. All acquired DSA images (100%) were assessed with excellent, good, or moderate-quality. Using DSA images, the stenosis degrees of renal arteries in 27 patients have been estimated as grade 1(n = 2, 7.4%), grade 2 (n = 8, 29.6%), grade 3 (n = 10, 37.0%), and grade 4 (n = 7, 25.9%). In comparison, based on the IFIR images, similar categories for these arteries have been shown: grade 1 (n = 1, 3.7%), grade 2 (n = 8, 29.6%), grade 3 (n = 9, 33.3%), and grade 4 (n = 9, 33.3%)(Table 2,Figure1-2). In addition, strong correlation was found (r = 0.937) between IFIR and DSA measurements for TRAS, and no significant difference was found between these two techniques (P=0.414)(Figure 3).
Discussion
In this study, we systematically investigated the stenosis degrees of transplant renal arteries with IFIR and DSA, respectively. Relative to the reference DSA, largely comparable performance has been shown with IFIR in the depiction of TRAS. In our study, the FIESTA based IFIR technique was used, which is a non-enhanced bright blood MR angiography technique. This examination does not require contrast agents, which not only reduces the cost of the test but also, more importantly, avoids the transplanted renal function jeopardized. Moreover, IFIR could present accessory renal artery as clearly as shown in DSA images(Fig 1). IFIR could also be performed longitudinally to further monitor the postoperative recovery after renal transplantation(Fig 2). All results obtained can demonstrate that IFIR is a noninvasive, accurate, repeatable method in the diagnosis and evaluation of TRAS.
Conclusions
In conclusion, TRAS was frequently occurred among patients after renal transplantation in our study. In this study, IFIR technique has shown accurate information in diagnosing TRAS without use of contrast agents and produced a satisfied concordance with DSA. In addition, due to no renal damage, IFIR can be used for follow-up examinations. Therefore, this technique can be suggested as a valuable method for renal transplant patients.
Acknowledgements
No acknowledgement found.References
1. Gaudiano C, Busato F, Ferramosca E, Cecchelli C, Corcioni B, De Sanctis LB, Santoro A, Golfieri R (2014). 3D FIESTA pulse sequence for assessing renal artery stenosis:is it a reliable application in unenhanced magnetic resonanceangiography?Eur Radiol; Dec;24(12):3042-50.
2. Yamuna J, Chandrasekharan A, Rangasami R, Ramalakshmi S, Joseph S (2017). Unenhanced renal magnetic resonance angiography in patients with chronic kidney disease & suspected renovascular hypertension: Can it affect patient management? Indian J Med Res; Nov;146(Supplement):S22-S29.
Figures

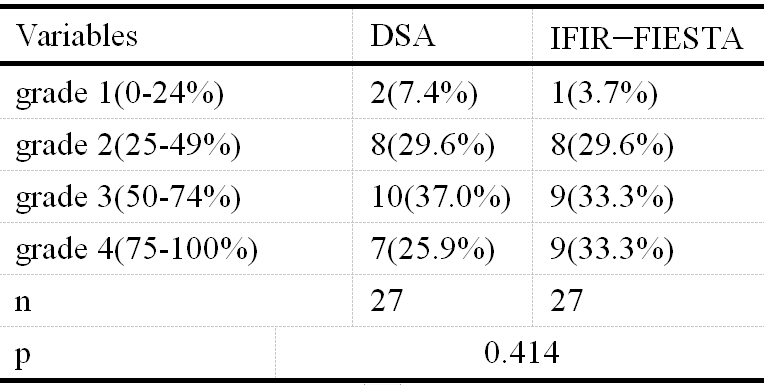
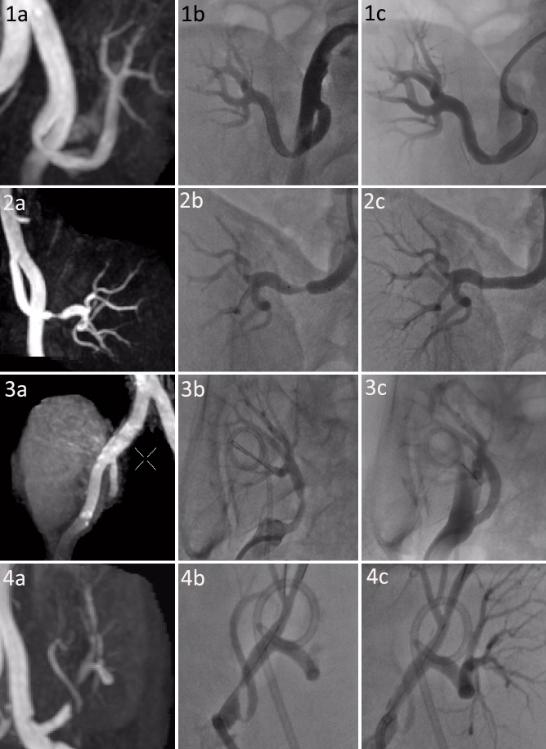
Fig 1: 1-4 Four patients with ages of 60, 48, 50, 36 respectively:
a, represents IFIR of patients before DSA;
b, DSA images confirmed the findings of IFIR;
c represents DSA after balloon dilatation and stent implantation.
1-2: stenosis degree of DSA images were same with IFIR;
3-4: IFIR images showed occlusion distal to the anastomotic stoma of the transplant renal artery; DSA images showed severe stenosis of transplant renal artery, IFIR images overestimated the stenosis.
4a, 4b: An accessory renal artery was seen with initial stenosis, and IFIR produced a satisfied concordance with DSA.

Fig 2
1a-d: A 40-year-old TRAS patient. IFIR (1a) before DSA showed anastomotic stenosis. DSA (1b) showed the extent of stenosis alleviating after balloon dilation. IFIR (1c, 1d) were performed after balloon dilation, which showed no evident stenosis of the transplant renal artery.
2a-d: A 51-year-old patient with TRAS. IFIR image (2a) showed apparent arterial stenosis, which was demonstrated by DSA (2b), and balloon dilation and stent implantation were performed (2c). IFIR image (2d) showed that arterial stenosis still existed after balloon dilation and stent implantation.