2190
Free-Breathing Cardiac Cine MRI with Compressed Sensing Real-Time Imaging and Retrospective Motion Correction1Siemens Medical Solutions USA Inc., Chicago, IL, United States, 2Siemens Medical Solutions USA Inc., Houston, TX, United States, 3Siemens Medical Solutions USA Inc., Los Angeles, CA, United States, 4Siemens Healthcare, Erlangen, Germany, 5Texas Children's Hospital, Houston, TX, United States
Synopsis
Free-breathing cardiac cine imaging is desirable for improving patient experience, expanding CMR eligibility, achieving robust image quality for uncooperative subjects, and simplifying CMR workflow. In this work, we propose a prototype technique, RTCSCineMoCo, that combines highly accelerated real-time acquisition, compressed sensing reconstruction, and retrospective, fully automated respiratory motion correction. In a preliminary evaluation on four volunteers, RTCSCineMoCo achieved similar spatiotemporal resolution, visually comparable image quality, and consistent LV function parameters as the reference breath-hold technique. RTCSCineMoCo is a promising option for free-breathing cardiac cine imaging, and further studies are warranted to evaluate its feasibility and utility in a clinical setting.
Introduction
Cine MRI is the gold standard for evaluating biventricular cardiac function1,2 and essential to most cardiac MR (CMR) programs. The current reference approach, 2D segmented acquisition with retrospective ECG gating3, requires patients to hold their breath for several seconds during data acquisition. This maneuver is typically repeated 10-20 times, with breaks in between, to acquire all desired slice orientations. However, breath-holding is uncomfortable, and often not possible for many patients such as those with heart failure. It is also undesirable for sedated subjects. In turn, such individuals may be less likely referred for CMR. Breath-holding also complicates the exam workflow, as the operator has to repeatedly give breath-hold commands and reattempt the scan should image quality be unsatisfactory. Therefore, free-breathing cine MRI is desirable for improving the patient experience, expanding CMR eligibility, achieving robust image quality for uncooperative subjects, and simplifying the CMR workflow.Several approaches have been proposed for free-breathing cardiac cine imaging, including segmented acquisition with respiratory gating using external respiratory signal4 or retrospective self-gating5,6, and multi-beat real-time acquisition and retrospective motion correction and data combination7,8. Limitations of these existing methods include lengthy acquisition time, compromised spatiotemporal resolution, or the need for external respiratory signal. In this work, we propose and preliminarily evaluate a prototype free-breathing cardiac cine imaging technique (RTCSCineMoCo) that addresses these limitations through a combination of highly accelerated real-time acquisition, compressed sensing (CS) reconstruction9, and retrospective, fully automated respiratory motion correction.
Methods
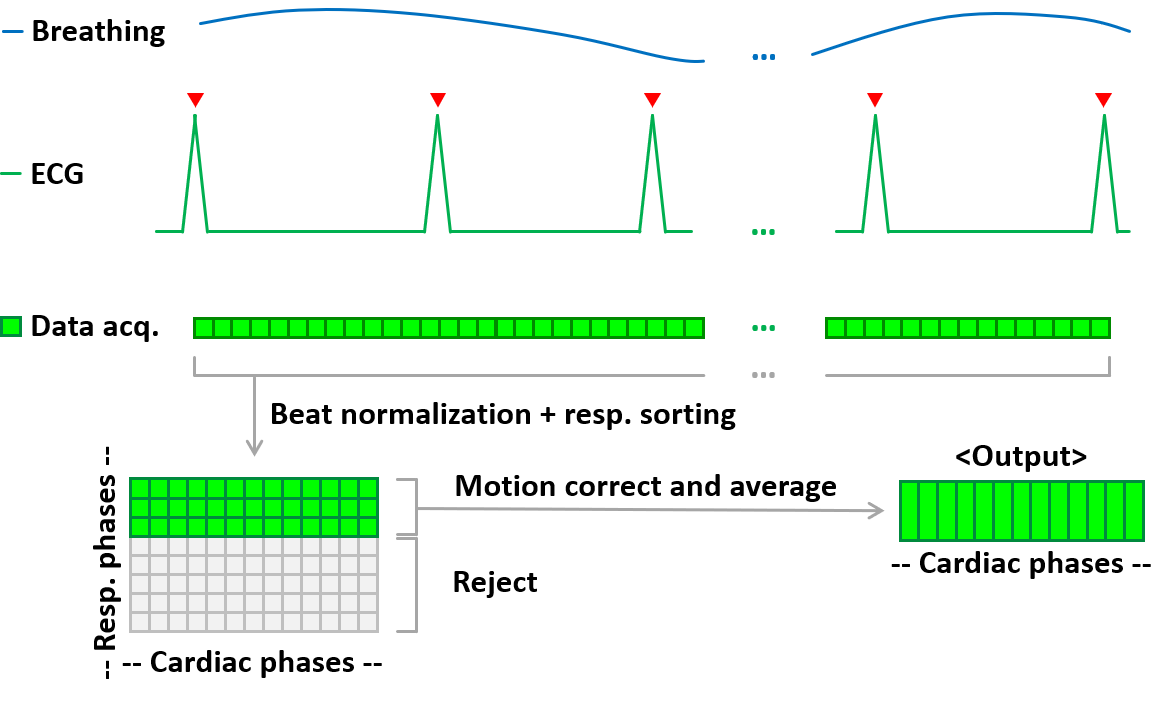
With institutional IRB approval and written consent, both breath-hold segmented cine with retrospective ECG gating (SegBH) and free-breathing RTCSCineMoCo images were acquired on four volunteers (59.5±13.0 years, two males) using a clinical 1.5T MR scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Full short-axis stacks were acquired for each patient using both techniques. The acquisition parameters were matched between the two wherever possible: balanced steady-state free precession readout, flip angle = 77-90°, TR = 32.9-36.7 ms, 25-26 cardiac phases, in-plane resolution = 1.8-2.0 mm interpolated to 0.9-1.0 mm, slice thickness = 8.0 mm; GRAPPA factor = 2 for SegBH; CS acceleration factor = 13.0-14.2 for RTCSCineMoCo; acquisition time = 11-12 heartbeats for SegBH (9.5-10.7 s) and 10.0-15.0 s for RTCSCineMoCo; the RTCSCineMoCo reconstruction is implemented inline including the following steps (Fig. 1): (1) normalization of each acquired beat via trigger time-based k-space rebinning; (2) CS reconstruction of the multi-beat real-time images; (3) ranking of the acquired beats based on respiratory motion estimation and setting the best beat as reference; (4) aligning a subset of the top-ranked beats (20-40% of the total number of beats acquired) to reference via non-rigid registration; (5) averaging the selected and aligned beats and outputting the result. Both SegBH and RTCSCineMoCo images were manually analyzed (Argus Function, Siemens Healthcare, Erlangen, Germany) to measure left ventricular (LV) end diastolic and systolic volumes (EDV, ESV), ejection fraction (EF), and stroke volume (SV).Results
LV function parameters derived from both SegBH and RTCSCineMoCo are summarized in Table 1. Overall the two techniques yielded similar results, with percentage differences ranging from -6.4%-+8.6%, -7.3%-+31.1%, -4.1%-+5.1%, -8.9%-+4.5% for EDV, ESV, EF, and SV, respectively. Example images from subjects 1-3 are shown in Figs. 2-4.Discussion
In this work, we developed and preliminarily evaluated a free-breathing cardiac cine imaging technique, RTCSCineMoCo, that combines highly accelerated real-time acquisition, compressed sensing reconstruction, and retrospective, fully automated respiratory motion correction. RTCSCineMoCo offered image quality visually comparable to the reference breath-hold technique, and yielded consistent LV function parameters (EDV, ESV, EF, SV). The free-breathing scan time was empirically set based on the estimated breathing rate to capture at least one heartbeat during the end-expiratory phase. From our preliminary experience, 10-15 seconds seemed appropriate for the adult subjects included in this abstract. Further studies are warranted to evaluate the feasibility and utility of RTCSCineMoCo in a clinical setting.Conclusion
Compressed sensing real-time imaging with motion correction is a promising method for robust free-breathing cardiac cine imaging.Acknowledgements
No acknowledgement found.References
[1] Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, Klein HU, Pennell DJ. Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two-dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. The American journal of cardiology. 2002 Jul 1;90(1):29-34.
[2] Grothues F, Moon JC, Bellenger NG, Smith GS, Klein HU, Pennell DJ. Interstudy reproducibility of right ventricular volumes, function, and mass with cardiovascular magnetic resonance. American heart journal. 2004 Feb 1;147(2):218-23.
[3] Carr JC, Simonetti O, Bundy J, Li D, Pereles S, Finn JP. Cine MR angiography of the heart with segmented true fast imaging with steady-state precession. Radiology. 2001 Jun;219(3):828-34.
[4] Krishnamurthy R, Pednekar A, Atweh LA, Vogelius E, Chu ZD, Zhang W, Maskatia S, Masand P, Morris SA, Krishnamurthy R, Muthupillai R. Clinical validation of free breathing respiratory triggered retrospectively cardiac gated cine balanced steady-state free precession cardiovascular magnetic resonance in sedated children. Journal of Cardiovascular Magnetic Resonance. 2015 Dec;17(1):1.
[5] Larson AC, Kellman P, Arai A, Hirsch GA, McVeigh E, Li D, Simonetti OP. Preliminary investigation of respiratory self‐gating for free‐breathing segmented cine MRI. Magnetic Resonance in Medicine. 2005 Jan;53(1):159-68.
[6] Hu P, Hong S, Moghari MH, Goddu B, Goepfert L, Kissinger KV, Hauser TH, Manning WJ, Nezafat R. Motion correction using coil arrays (MOCCA) for free‐breathing cardiac cine MRI. Magnetic resonance in medicine. 2011 Aug;66(2):467-75.
[7] Xue H, Kellman P, LaRocca G, Arai AE, Hansen MS. High spatial and temporal resolution retrospective cine cardiovascular magnetic resonance from shortened free breathing real-time acquisitions. Journal of Cardiovascular Magnetic Resonance. 2013 Dec;15(1):102.
[8] Rahsepar AA, Saybasili H, Ghasemiesfe A, Dolan RS, Shehata ML, Botelho MP, Markl M, Spottiswoode B, Collins JD, Carr JC. Motion-Corrected Real-Time Cine Magnetic Resonance Imaging of the Heart: Initial Clinical Experience. Investigative radiology. 2018 Jan 1;53(1):35-44.
[9] Kido T, Kido T, Nakamura M, Watanabe K, Schmidt M, Forman C, Mochizuki T. Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold. Journal of Cardiovascular Magnetic Resonance. 2016 Dec;18(1):50.
Figures