2184
Real-time cardiac imaging without ECG gating and respiratory control to monitor arrhythmia1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Neusoft Medical Systems, Shanghai, China, 3Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Chalestown, MA, United States, 4Department of Radiology, Harvard Medical School, Boston, MA, United States
Synopsis
Non gated real-time cardiac MR imaging with Partial Separable model provides a promising way to overcome the limitation of conventional cine imaging. The new method is able to capture the beat by beat variation, which is especially suitable for arrhythmia. In this study, we have 2 aims. First, to evaluate the consistency of parameters between the conventional cine method and the PS model based real-time method, and second, to capture beat by beat variation in arrhythmia patient.
Introduction
Heart disease is the leading cause of death around the world. Cardiovascular magnetic resonance (CMR) has made great contributions to evaluate the cardiac function. Recently, real-time cardiac MR imaging provides a promising way to overcome the limitation of conventional cine imaging. For example, the new method with Partial Separable model [1, 2, 3] is able to capture the beat by beat variation, which is especially suitable for arrhythmia. Without electro-cardiogram (ECG) gating and breath-hold, the technique is easy to scan. However, the accuracy of the method remains to be proved. In this study, we have 2 aims. First, to evaluate the consistency of parameters between the conventional cine method and the PS model based real-time method, and second, to capture beat by beat variation in arrhythmia patient.Materials and Methods
Subjects: Four healthy volunteer (4 males, age: 22-27 years, median: 24.5 years) with no symptoms of cardiovascular disease and one patient with cardiac arrhythmia (female, 26 years old) was were included. MRI Scan: Imaging experiments were conducted on a 3.0 T whole-body MR scanner (Ingenia, Philips Medical System, Best, The Netherlands). The scan region involved seven short axis slices from apex to base of the heart. A 32-channel cardiovascular coil with T1-TFE sequence was used for scan. Both cine method and real-time method were applied with the following scan parameters: field of view (FOV) = 300mm×264mm (RL/AP), spatial resolution = 2.0mm×2.4mm, matrix size = 152×220, TR = 5.5ms, TE = 3.3ms, flip angle (FA) = 15°. The scan duration for each slice was 18 seconds with breath hold and ECG gating for cine method, and 50 seconds without any gating for real-time method. Temporal resolution = 33ms (for cine) / 11ms (for real-time). The acquisition trajectory for real-time method was the same as reference [1]. Reconstruction: Images of real-time were reconstructed with PS model. For cine image, sum of squares (SOS) was applied. Image analysis: Since images of real-time method included a long period with multiple cardiac cycles, three cycles were selected randomly for evaluation. The endocardium and epicardium of left ventricle (LV) were circled in the end systolic and end diastolic. Clinical parameters including ejection fraction (EF), cardiac output (CO), stroke volume index (SVI) and left ventricle mass (LVM) were calculated for both cine cycles and three real-time cycles. Statistical analysis: The area of endo and epi and clinical parameters were evaluated with Bland-Altman comparison between cine results and averaged real-time results. Correlation coefficient were calculated to verify the consistency of two methods. All statistical results were acquired from the MedCalc (Version 18.2.1, MedlCalc Software, Ostend, Belgium).Results
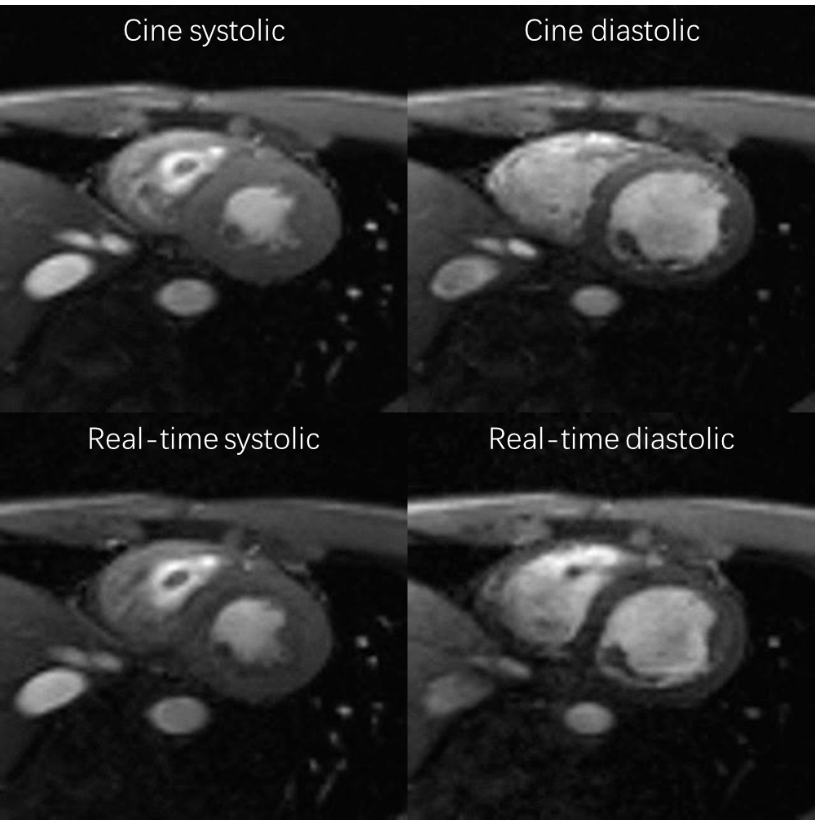
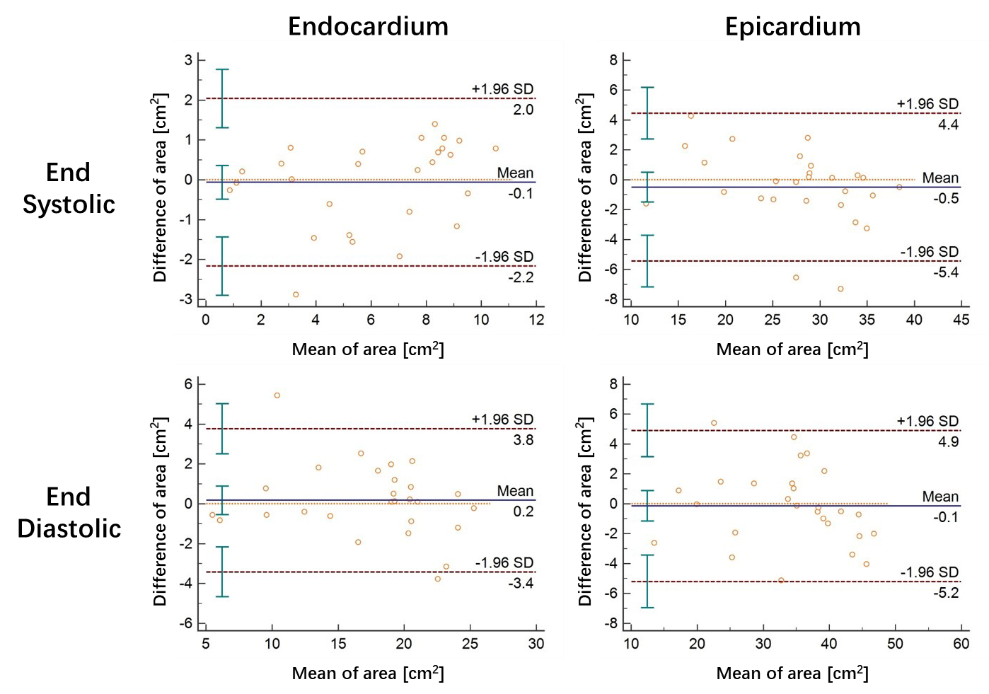
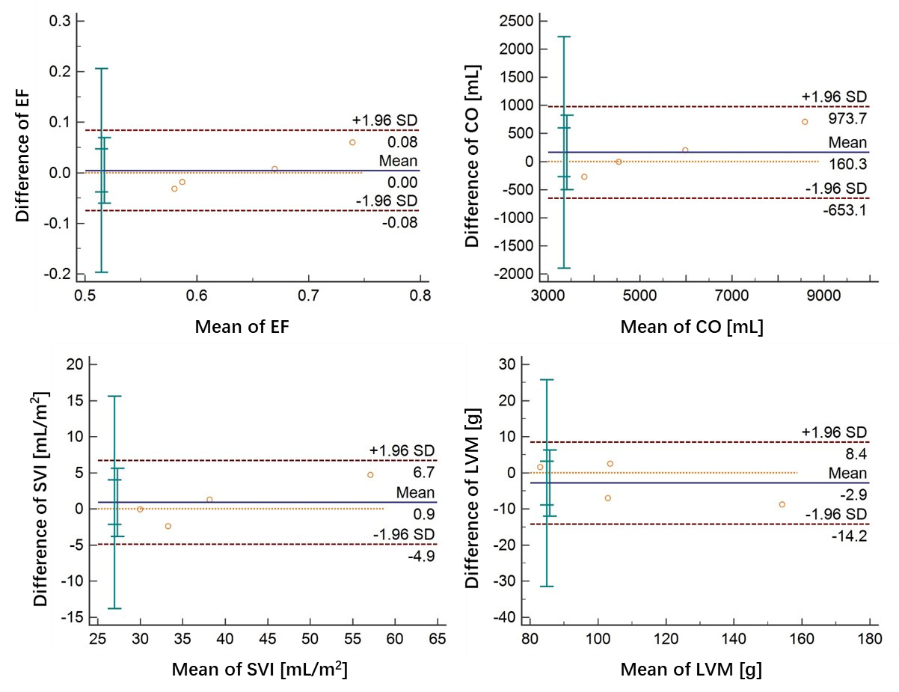
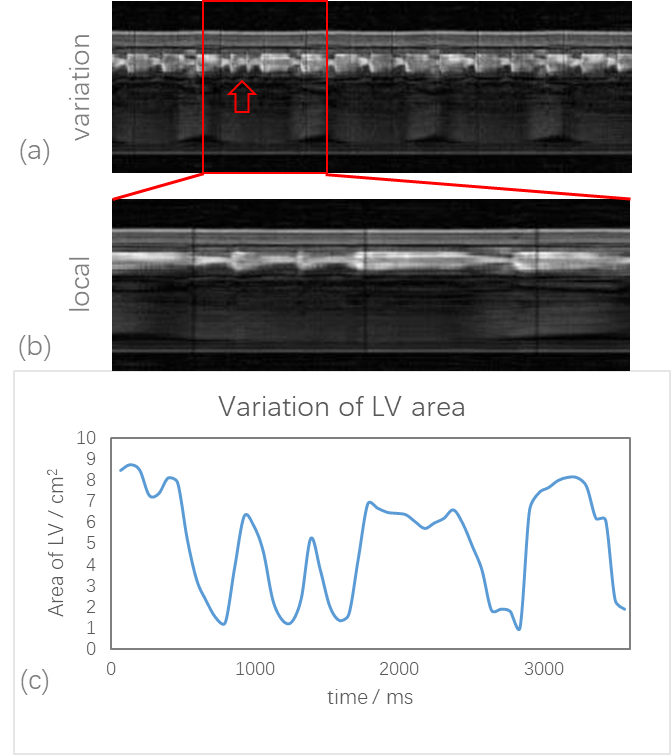
Figure 1 showed the end systolic and end diastolic images for both cine and real-time methods of one slice. The morphology of cardiac for the two methods was similar to each other. The Bland-Altman comparison for area of endo and epi in end systolic and end diastolic of each slice between cine and real-time methods were shown in Figure 2. As can be seen, the area of real-time method was in great agreement with cine method in different cardiac phase. Figure 3 showed the Bland-Altman analysis of EF, CO, SVI and LVM to compare the clinical parameters between the two methods. They all in great consistency. Figure 4 showed the median and standard deviation of the clinical parameters for cine and real-time methods. In addition, correlation coefficient was calculated, which demonstrated the consistency of clinical parameters. Some results of arrhythmia were shown in Figure 5. The variation with time of one line across the LV showed the different cardiac cycles. The arrhythmia cycles were marked with arrow. The variation of LV area also indicated the happening of arrhythmia.Discussion
The consistency between cine and real-time cardiac imaging methods was investigated in this study. These results indicated that the novel real-time method can acquired comparable images and clinical parameters as conventional cine method. In particular, the irregular cycles when arrhythmia occurs can be captured by the new method, which can provide extra information for diagnosis. Future research will enlarge the number of subjects and make further evaluation about arrhythmia.Conclusion
In this study, real-time cardiac imaging, without ECG gating and respiratory control, was proved to be consistent with conventional cine method. Particularly, the new method can capture irregular cardiac cycles, which is beneficial for diagnosis of cardiac diseases.Acknowledgements
No acknowledgement found.References
[1] Sun A, Zhao B, Li Y, et al. Real-time phase-contrast flow cardiovascular magnetic resonance with low-rank modeling and parallel imaging[J]. Journal of Cardiovascular Magnetic Resonance, 2017, 19(1): 19.
[2] Zhao B, Haldar J P, Brinegar C, et al. Low rank matrix recovery for real-time cardiac MRI. In Proceedings of 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, 2010: 996-999.
[3] Liang Z.-P, Spatiotemporal imaging with partially separable functions, IEEE International Symposium on Biomedical Imaging, 2007, pp. 988-991.
Figures