2172
Cardiac magnetic resonancefeature-tracking for myocardial strain assessment in real-time cardiac cine MRI
1Radiology, Northwestern University, Chicago, IL, United States, 2Biomedical Engineering, Northwestern University, Chicago, IL, United States, 3Medicine, Northwestern University, Chicago, IL, United States
Synopsis
Cardiac magnetic resonance feature-tracking (CMR-FT) has emerged as a reference standard for the evaluation of cardiac morphology and function. But, the performance of CMR-FT may be affected by data undersampling as done in several real-time cardiac MRI techniques. In our study, we evaluated the performance of CMR-FT for myocardial strain quantification from real-time cardiac cine MRI when compared to standard cardiac cine in cardiac disease patients. We found that even though there is good agreement between the values derived from the real-time and standard cine MRI, care should be taken as measures from the real-time cine can be underestimated.
Introduction
Cardiac magnetic resonance feature-tracking (CMR-FT) has recently emerged as a useful tool for the quantitative evaluation of cardiovascular function owing to its ability to assess regional myocardial function impairment and lack of need for a separate imaging sequence such as myocardial tagging, DENSE, or SENC. CMR-FT strain measures are usually derived from ECG-gated, breath-hold balanced steady-state free precession (bSSFP) cine acquisitions. This acquisition has several limitations including long scan-times and compromised image quality in patients with arrhythmias or insufficient breath-holding capacity. Real-time cardiac MRI is an alternative technique that allows dynamic imaging of the heart without the need for ECG synchronization or breath-holding. But undersampling of the images in these real-time techniques may affect the CMR-FT algorithms that rely on recognizing features or patterns in the images. Thus, the aim of this study was to evaluate the performance of CMR-FT based myocardial strain quantification from a 16-fold accelerated, real-time cardiac cine MRI with radial k-space sampling and compressed sensing (CS) in patients with cardiac disease at 1.5T and 3T.Methods
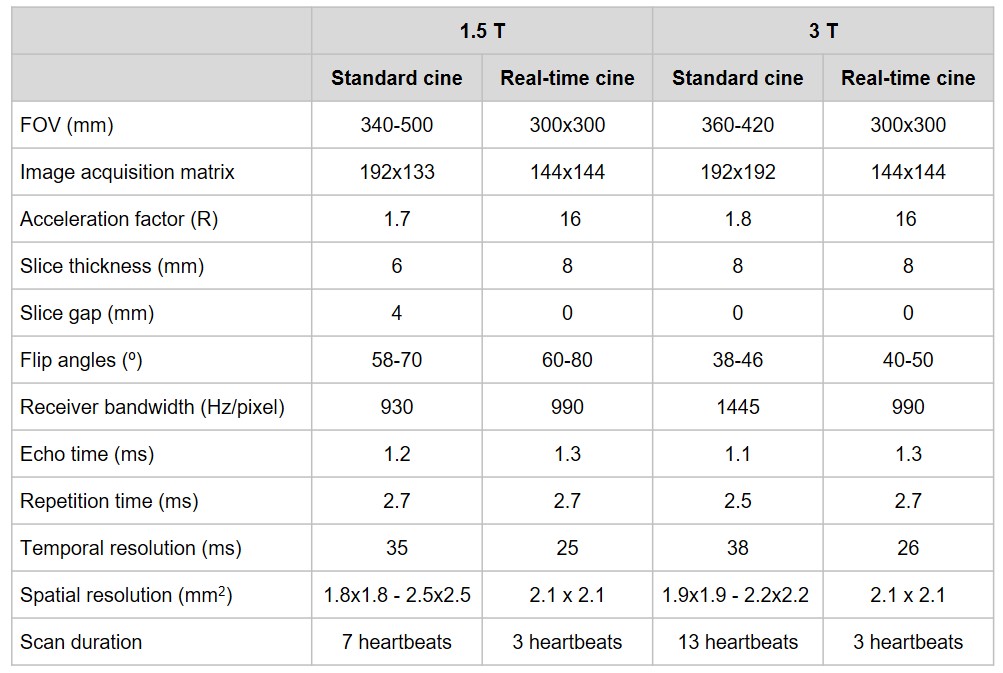
Study cohort: Thirty-four patients underwent standard breath-hold cardiac cine MRI and real-time cardiac cine MRI acquisitions. The patients imaged belonged to two disease cohorts: prior myocardial infarction group (MI; n = 15; mean age, 59.1 ± 12.6 y; male, n = 11; female, n = 4; mean heart rate, 66.9 ± 7.0 bpm; left ventricular ejection fraction, 21%–70%) and chronic kidney disease group (CKD; n = 19; mean age, 63.9 ± 16.2 y; male, n = 9; female, n = 10; mean heart rate, 65.8 ± 7.3 bpm; left ventricular ejection fraction, 46%–79%).MRI data acquisition and reconstruction: The first cohort of MI patients were scanned on a 1.5T whole‐body MRI scanner (Aera; Siemens). The second cohort of CKD patients were scanned on a 3T whole‐body MRI scanner (Skyra; Siemens). Image acquisition parameters are detailed in table 1. Undersampled data were reconstructed using the GRASP (radial CS) framework [1, 2]. GRASP reconstructions were performed offline in MATLAB (MathWorks).
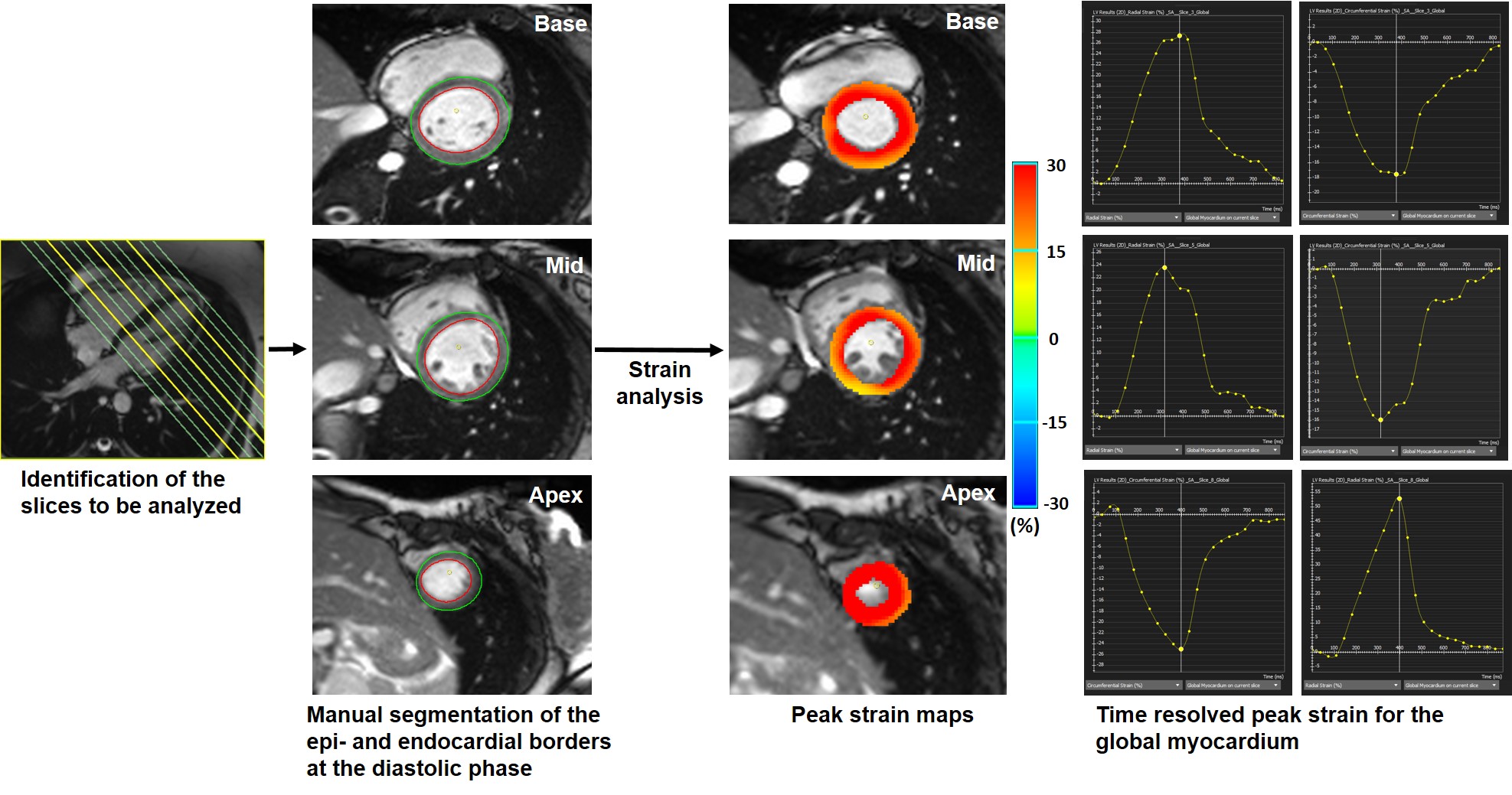
CMR-FT analysis: CMR-FT was used to measure the left ventricular myocardial peak radial strain (Err) and circumferential strain (Ecc) from the short-axes images from both these acquisitions (cvi42, Circle). On all images, the epicardial and endocardial borders were outlined in the end-diastole (figure 1). The software then automatically propagated the contours throughout the remainder of the cardiac cycle. A second investigator also evaluated 15 studies for the assessment of inter-observer reproducibility. Pearson correlation coefficients and Bland-Altman plots were used to assess agreement between the two methods. Interobserver reproducibility was assessed using Intraclass Correlation Coefficient (ICC) (SPSS, IBM).
Results
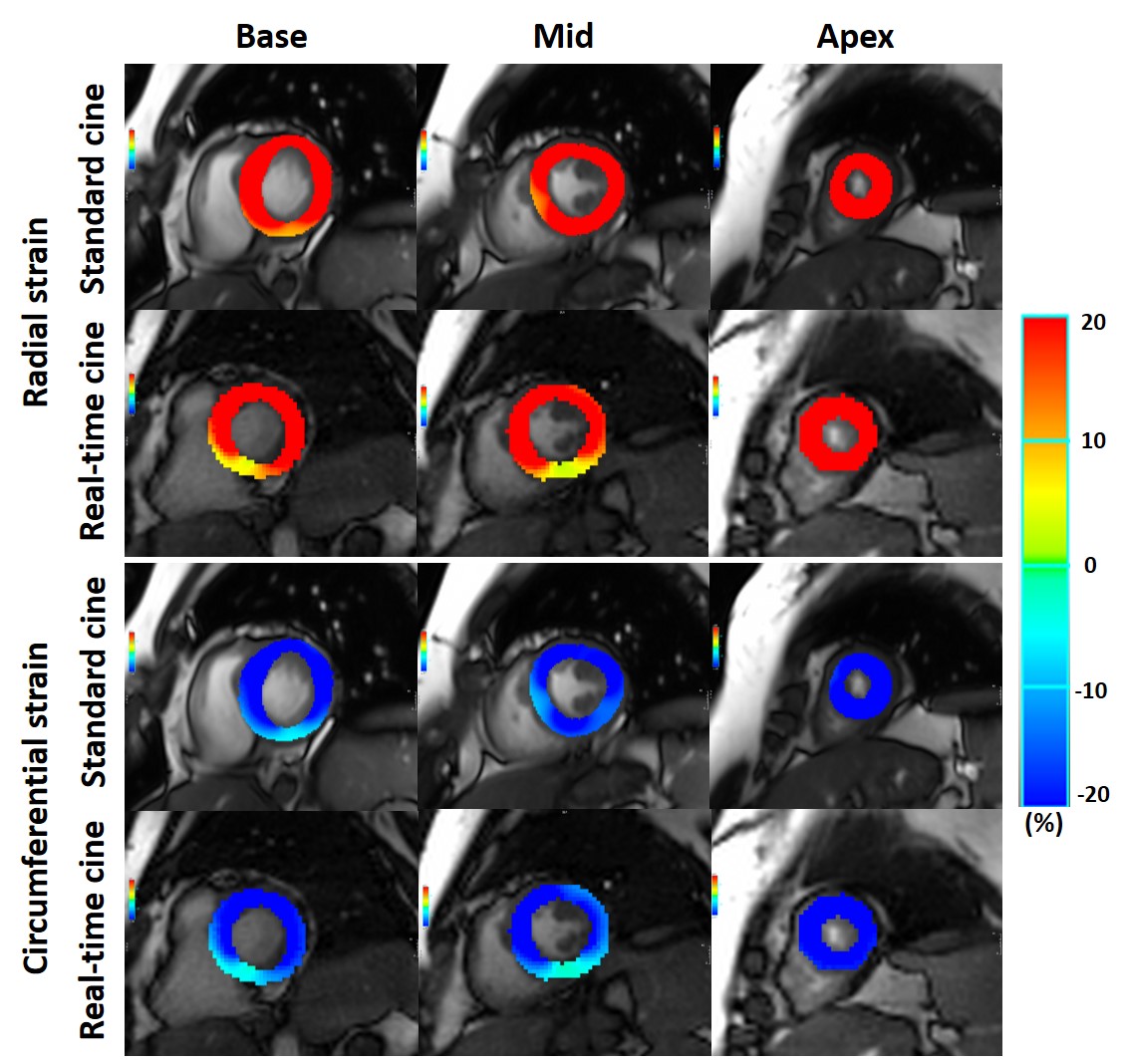
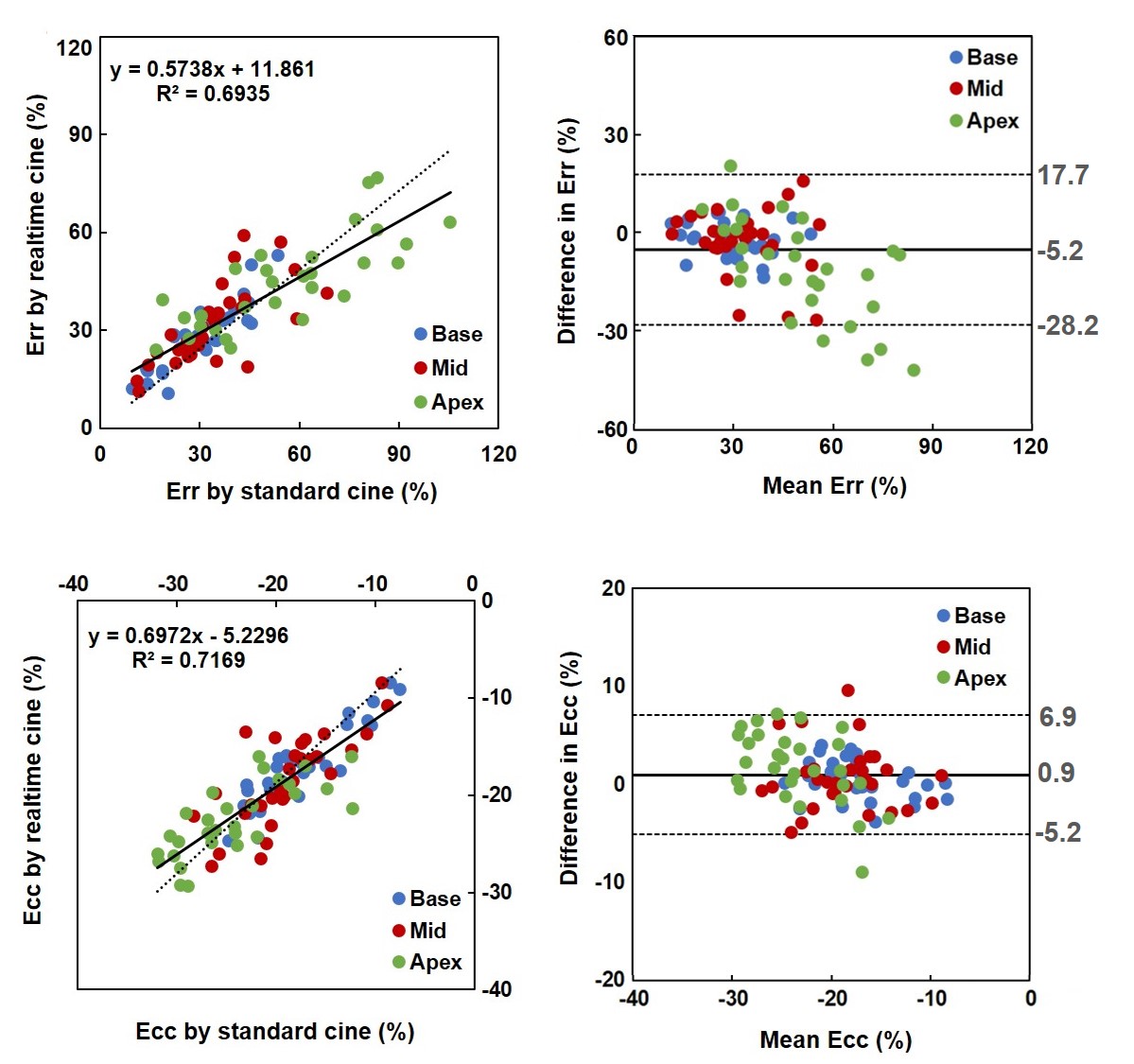
The standard breath-hold cine MRI obtained from four out of the 34 patients included in the study were not analyzable because of artifacts due to arrhythmia. The real-time cine images of these patients were artifact-free and showed reasonable strain values, but were excluded form statistical analysis. Strain plots at peak systole for a representative subject is shown in figure 2. There was good correlation and agreement between the strain measurements derived from the standard breath-hold cine and the real-time cine; Err [r2=0.69; p<.001; bias: -5.2%, 95% CI limits of agreement (LOA): -28.2 to 17.7%] and Ecc [r2=0.72; p<.001; bias: 0.9%, 95% CI limits of agreement (LOA): -5.2 to 6.9%] (figure 3). The mean Err (standard cine: 40.1±20.5%; real-time cine: 35.3±14.6%; p<.001) and Ecc (standard cine: -20.1±5.8%; real-time cine: -19.4±4.8%; p=.01) was significantly underestimated by the real-time cine compared to the standard cine. The median percentage underestimation for Err was -8.5% (IQR: -23.1% to 6.9%) and for Ecc was -3.8% (IQR: -13.0% to 3.6%). There was excellent interobserver agreement for the Err (ICC = 0.94, 95% CI LOA: 0.88 to 0.96) and Ecc (ICC = 0.93, 95% CI LOA: 0.88 to 0.96).Discussion
CMR-FT techniques falls in a general category of image post-processing methods known as optical flow [3, 4]. The tracking method identifies a relatively small tracking window on one image and then searches for the most comparable image pattern in a window of the same size in the subsequent frame. In CS reconstruction, regularization may suppress features that are necessary for optical flow to track, reducing accuracy of measurements. Low temporal resolution and spatial resolution also negatively affects the tracking efficiency. Radial strain is computed on the small distance between endo and epicardium, and was affected more than circumferential strain that are computed over larger regions [5].Conclusion
This study demonstrates that CMR-FT derived strain measurements from a 16-fold accelerated, real-time cine MRI with compressed-sensing is comparable to the measures derived from standard breath-hold cine MRI. Although good agreement was found between the two sequences, it should be kept in mind that strain measurements from undersampled cardiac MRI can be underestimated and is dependent on the spatiotemporal resolution of the sequence and regularization induced by CS.Acknowledgements
No acknowledgement found.References
1. Feng, L., et al., Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med, 2014. 72(3): p. 707-17.
2. Haji-Valizadeh, H., et al., Validation of highly accelerated real-time cardiac cine MRI with radial k-space sampling and compressed sensing in patients at 1.5T and 3T. Magnetic Resonance in Medicine, 2018. 79(5): p. 2745-2751.
3. Singh, A., Optic flow computation : a unified perspective. 1991, Los Alamitos, Calif.: New York : IEEE Computer Society Press, Institute of Electrical and Electronics Engineers.
4. Barron, J.L., D.J. Fleet, and S.S. Beauchemin, Performance of optical flow techniques. International Journal of Computer Vision, 1994. 12(1): p. 43-77.
5. Langeland, S., et al., Experimental assessment of a new research tool for the estimation of two-dimensional myocardial strain. Ultrasound Med Biol, 2006. 32(10): p. 1509-13.
Figures