2164
Preventive fraction of long-term cardiac function with cardiorespiratory fitness and physical activity in childhood leukemia survivors.
Delphine Perie1, Maxime Caru2, Marianna Gamba1, Louise Leleu1, and Daniel Curnier2
1Mechanical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Kinesiology, University of Montreal, Montreal, QC, Canada
1Mechanical Engineering, Polytechnique Montreal, Montreal, QC, Canada, 2Kinesiology, University of Montreal, Montreal, QC, Canada
Synopsis
In childhood leukemia survivors, doxorubicin leads to dose-dependent cardiotoxicity, despite early diagnosis with both echocardiography and MRI investigations. Physical activity has the potential to reduce the chronic disease risk, but it is currently unknown whether a good cardiorespiratory fitness or the regular practice of physical activity is enough to induce a preventive action on the cardiac function. This study included 81 ALL survivors and found that a good cardiorespiratory fitness was associated with a better preventive fraction, similarly to a good physical activity level. It would be more than 80% of the survivors who could benefit from these long-term effects.
Introduction
Over the past four decades, the progress in treatments for childhood acute lymphoblastic leukemia (ALL) has made it possible to achieve a five-year survival rate of over 90%. Unfortunately, doxorubicin leads to dose-dependent cardiotoxicity [1] and although both echocardiography and MRI investigations can diagnose these effects, it results in late detection, even when using strain quantification. The use of contrast-enhanced T1 imaging would allow early detection of doxorubicin-induced cardiotoxicity [2,3], especially since mechanical properties of the myocardium are considered as early biomarkers of subtle changes in cardiomyopathy. Recently, it has been observed that physical activity has the potential to reduce the chronic disease risk, in addition to inducing a positive remodeling in heart failure patients. However, it is currently unknown whether a good cardiorespiratory fitness or a regular practice of physical activity is enough to induce a preventive action on late adverse effects of the cardiac function in childhood ALL survivors.Methods
A total of 81 childhood ALL survivors (Table 1) underwent a maximal cardiopulmonary exercise test, completed a physical activity questionnaire and a battery of clinical examinations. We calculated the odds ratio to obtain the preventive fraction (PF) to evaluate the effects of the cardiorespiratory fitness and physical activity levels on cardiac outcomes if all the cohort had a good fitness or physical activity. The association between cardiorespiratory fitness and cardiac magnetic resonance (CMR) parameters was studied using the median of the cardiorespiratory fitness (< or ≥ 31.4 mL.kg-1.min-1). Survivors were considered active if they had practiced ≥150 minutes per week of moderate to vigorous physical activity (MVLPA). The CMR acquisitions were performed on a Siemens Skyra 3T MR system using a 18-channel phased array body matrix coil and included a MOLLI sequence for T1 mapping, a T2-prepared TrueFISP sequence for T2 mapping at apical, mid-ventricular and basal levels (pixel resolution 1.4mmx1.4mmx8.0mm), and an ECG-gated cine TruFISP sequence (14 slices in short axis and 5 slices in long axis, slice thickness 8mm, repetition time 34.6ms, effective echo time 1.2ms, flip angle 38°, iPAT factor 3, matrix 208x210 and in-plane pixel size 1.25x1.25 mm).Results
Based on survivor’s cardiopulmonary exercise test, we obtained a mean O2 peak of 31.6±7.8 mL∙kg-1∙min-1 and a mean MVLPA of 24.7±34.1 min/day (Table 2). The associations between a higher cardiorespiratory fitness and the prevalence of each CMR parameters were evaluated using the preventive fraction obtained from the odds ratio (Table 3). From analyses based on the cardiorespiratory fitness level above the median, we observed significant preventive fractions in left ventricle and in right ventricle function: LV_EDV (84%; p<0.001), LV_ESV (80%; p<0.001), LV_SV (75%; p<0.001), RD_EDV (75%; p<0.01), RV_ESV (88%; p<0.001), RV_SV (69%; p<0.01). Also, significant preventive fractions was observed in T1gd (88%; p<0.001), LG3E_volume (82%; p<0.001) and LGE5_volume (82%; p<0.001). When analyses were adjusted with age, sex, age at diagnosis, time since the diagnosis, doxorubicin and dexrazoxane, we observed significant preventive fractions in left ventricle and in right ventricle function: LV_EDV (88%; p<0.05), LV_ESV (85%; p<0.05), RD_EVD (88%; p<0.05) and RV_ESV (92%; p<0.05). Also, significant preventive fractions were observed in T1gd (97%; p<0.01), LG3E_volume (90%; p<0.05), and LGE5_volume (90%; p<0.05). Although the preventive fraction for a few variables was not significant, they all indicated a positive impact of a higher O2 peak.Discussion
This study explores the association between cardiorespiratory fitness and physical activity levels on various cardiac function variables. We showed that a good cardiorespiratory fitness was associated with a better preventive fraction, similarly to a good physical activity level. In this sense, this study demonstrates the importance of physical activity and a good cardiorespiratory fitness in the management of long-term adverse effects measured by CMR parameters of the left and right heart (T1gd, LG3E_volume, LGE5_volume, T1gd and ESV). This study also confirms the results of previous studies, especially in childhood ALL survivors. This is all the more important that the use of the preventive fraction allows us to understand the scope of these associations due to their expression in percentage. Thus, with a good cardiorespiratory fitness and a good physical activity level, it would be more than 80% of the survivors who could benefit from these long-term effects.Conclusion
The association between cardiorespiratory fitness and CMR parameters demonstrated that a good cardiorespiratory fitness and a good physical activity level were associated with a higher preventive fraction for most cardiac function variables in ALL survivors. This study provides additional evidence regarding the benefits of exercise for cancer survivors, while CMR could be used to evaluate changes induced by exercise programs and to check their safety. Moreover, the use of quantitative parameters would better understand the mechanisms involved in the cardiac remodeling induced by the exercise and to open the discussion.Acknowledgements
This work was supported by the Institute of Cancer Research (ICR) of the Canadian Institutes of Health Research (CIHR), in collaboration with C17 Council, Canadian Cancer Society (CCS), Cancer Research Society (CRS), Garron Family Cancer Centre at the Hospital for Sick Children, Ontario Institute for Cancer Research (OICR) and Pediatric Oncology Group of Ontario (POGO). This research was also supported in part by PhD study grants from Cole Foundation, Fonds de Recherche du Québec – Santé (FRQS), Sainte-Justine University Hospital Center Foundation and Foundation of Stars. We also thank the NSERC and Polytechnique Montreal for the financial support, as well as researchers from the PETALE study for the opportunity to perform this complementary analyses in the childhood ALL survivors cohort.References
1- Aissiou M, Périé D, Cheriet F, Dahdah NS, Laverdière C, Curnier D. Imaging of early modification in cardiomyopathy: the doxorubicin-induced model. Int J Cardiovasc Imaging. 2013; 29(7):1459-76. 2- Perel RD, Slaughter RE, Strugnell WE. Subendocardial late gadolinium enhancement in two patients with anthracycline cardiotoxicity following treatment for Ewing's sarcoma. JCMR 2006;8(6):789-791. 3- Wassmuth R, Lentzsch S, Erdbruegger U, et al. Subclinical cardiotoxic effects of anthracyclines as assessed by magnetic resonance imaging-a pilot study. American heart journal 2001;141(6):1007-1013.Figures
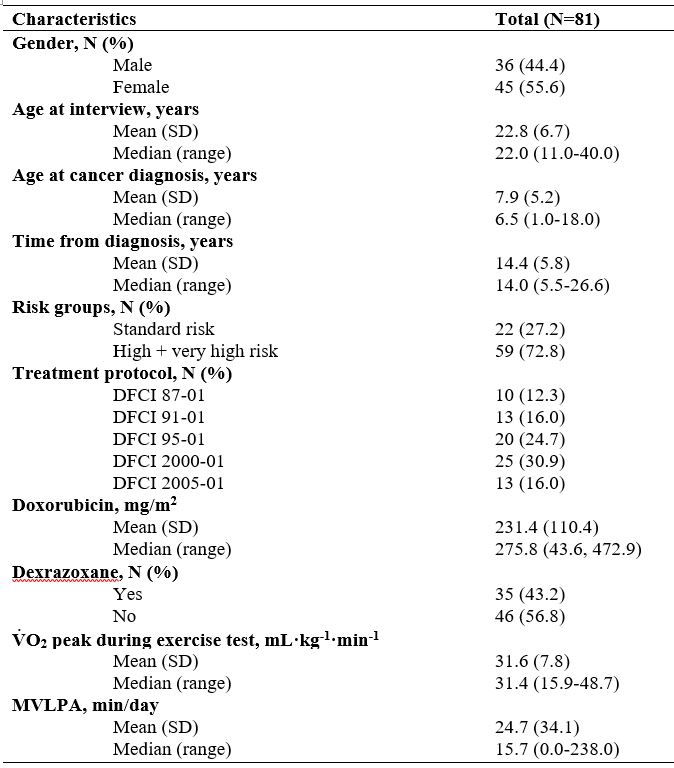
TABLE 1. Clinical Characteristics of Childhood ALL
Survivors. DFCI: Dana Farber Cancer Institute; VO2 peak: maximum
oxygen consumption; MVLPA: moderate
and vigorous leisure physical activities.
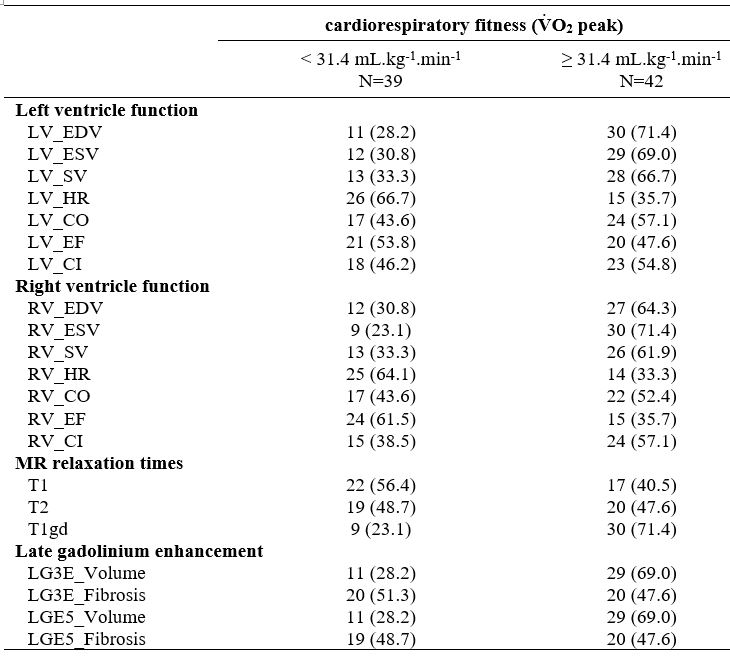
TABLE 2. Prevalence of CMR
Parameters among Childhood ALL Survivors. VO2 peak: maximum oxygen consumption; MVLPA: moderate
and vigorous leisure physical activities.
The prevalence was given according to the survivors with scores on cardiac
magnetic resonance imaging parameters above the median of our cohort.
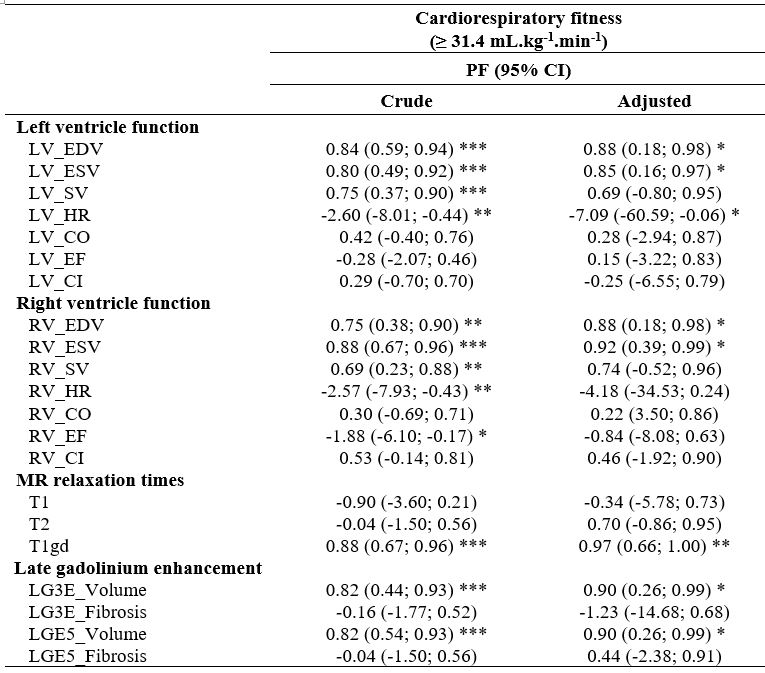
TABLE 3. Crude and Adjusted Logistic Regression for Cardiac Magnetic
Resonance Imaging Parameters Associated with Cardiorespiratory Fitness. PF:
preventive fraction; CI: confidence interval; VO2 peak:
maximum oxygen consumption; MVLPA: moderate and vigorous
leisure physical activities. *p<0.05 **p<0.01 ***p<0.001. Models for all outcome
variables were adjusted for age, sex, age at diagnosis, time since the
diagnosis, doxorubicin, dexrazoxane.