2159
Improved visualization of non-contrast-enhanced MRA of the foot using REACT with balanced SSFP-DIXON (bREACT) at 1.5T1Department of Radiological Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
In this study we demonstrated the feasibility of dual-echo balanced SSFP-DIXON sequence with REACT technique for the foot MRA at 1.5T. bREACT dramatically increased the SNR compared to conventional REACT and it could provide excellent contrast between blood vessels and background tissues with high robustness compared with other conventional non-contrast-enhanced MRA methods. This technique would be helpful to assess peripheral blood vessels in the diabetic patients.
Introduction
Evaluating blood flow at the foot is important for diagnosing peripheral artery disease (PAD), especially for making decision of amputation of diabetic foot lesions in the patients of diabetes mellitus.1 Although conventional contrast-enhanced or non-contrast-enhanced MRA techniques could stably depict arteries from the aortic bifurcation to the foot dorsal artery, it is often difficult to visualize peripheral foot blood vessels. MR digital subtraction angiography (MR-DSA) using contrast agent is most established method. However diabetic patients are often co-occurring kidney disorder, so it is difficult to use the contrast agents2-5. On the other hand, non-contrast-enhanced techniques, such as TOF-MRA and phase-contrast (PC) have also some limitation for foot MRA because of their image quality and/or long acquisition time. Recently, a new non-contrast-enhanced, relaxation-based, flow-independent MRA method, called Relaxation-Enhanced Angiography without Contrast and Triggering (REACT) for vascular imaging in various body parts with large anatomical coverage6. Since REACT utilizes the difference in relaxation times, it detects venous signals as well as arteries, but it enables to visualize stably blood vessels as a whole. One of the challenges of REACT is its relatively low signal-to-noise ratio (SNR) at 1.5T unlike the 3.0T, because REACT is based on DIXON spoiled-gradient echo sequence and it requires very high readout bandwidth to prevent prolongation of TR/TE. Such low SNR should adversely affect in depiction of peripheral vessel at the foot. In this study, we attempted to combine dual-echo balanced SSFP-DIXON sequence with REACT technique to gain the SNR for the foot MRA at 1.5T. The purpose of this study was to investigate the feasibility of balanced SSFP-DIXON REACT (bREACT) by comparing with other conventional methods.Methods
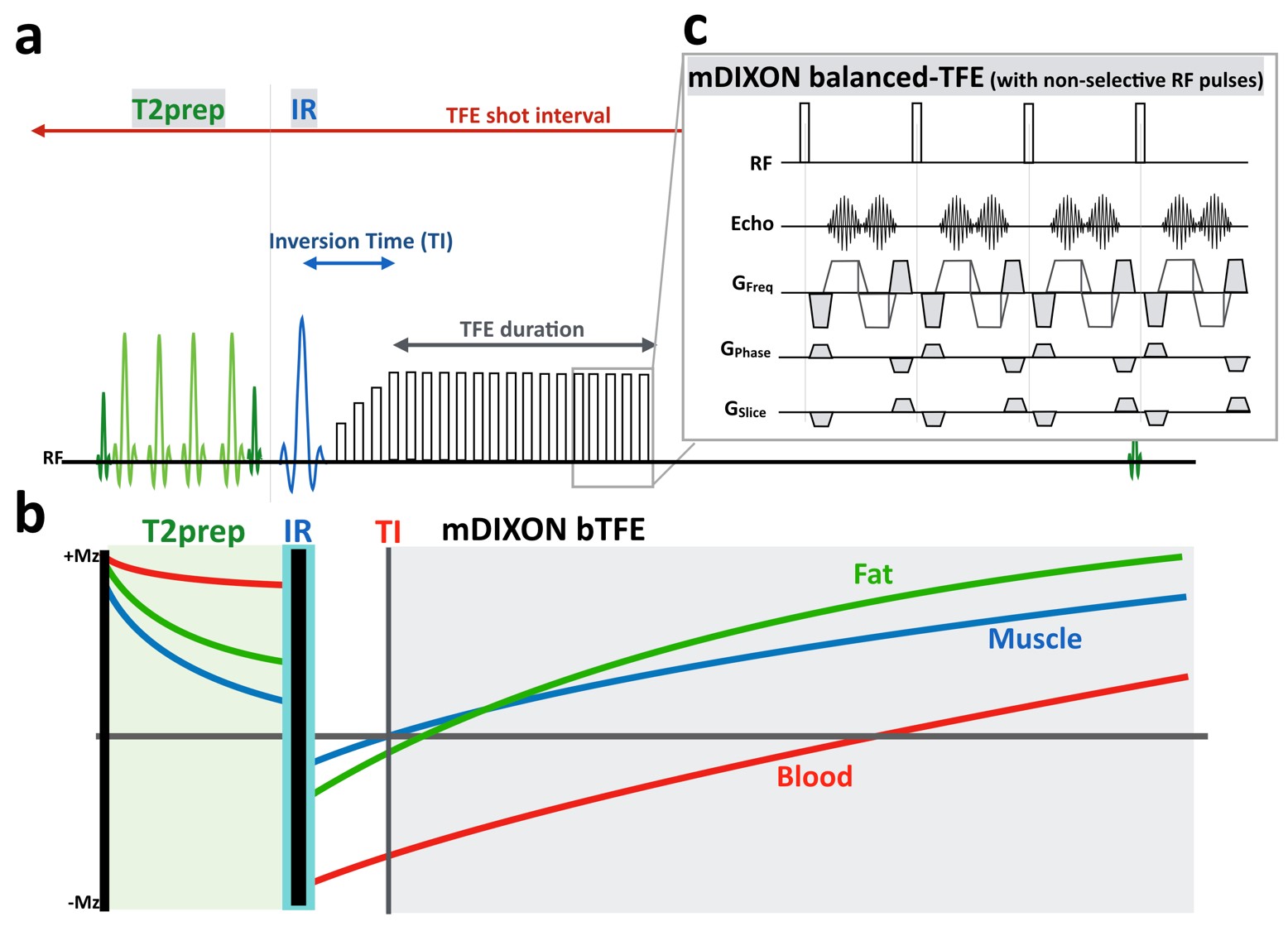
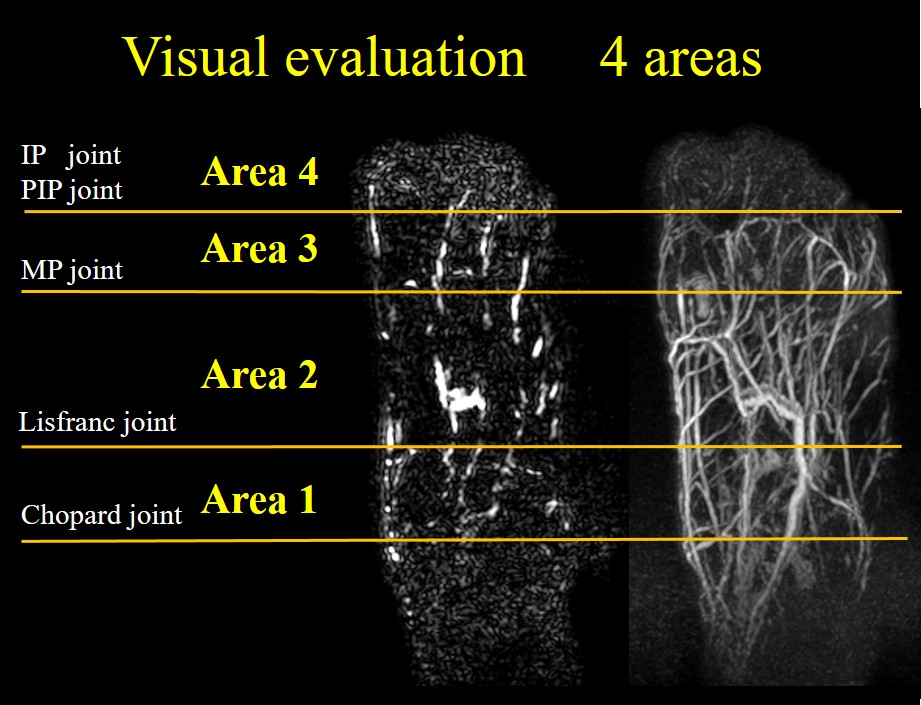
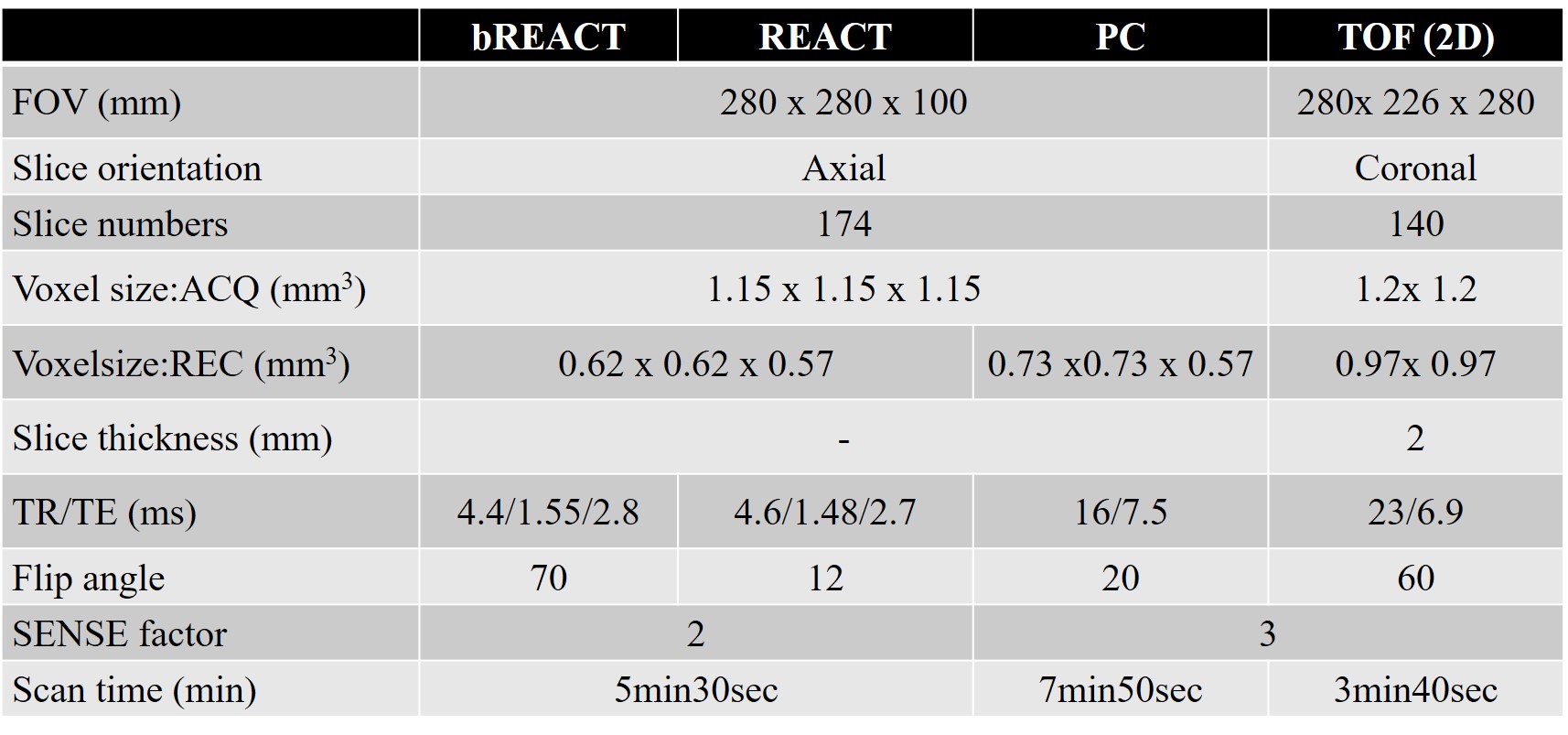
A total of five volunteers (4 men, 1 woman, age range 25 to 45) were examined on a 1.5T MRI (Ingenia CX, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. Scheme of the bREACT sequence is shown in Figure 1. REACT basically consists of a 3D dual-echo Dixon segmented spoiled gradient echo (turbo field-echo: TFE) and magnetization preparation with a T2prep pulse and a non-selective inversion recovery (IR) pre-pulse [Fig.1a]. Magnetization preparation pulses were implemented to suppress signal from static tissues, such as muscles, nerves and organs, and to enhance blood-to-tissue contrast based on their difference in relaxation times. A T2-prep pulse was applied to reduce signal from tissues with short T2. Immediately after that an IR pulse was applied with a short inversion time (TI) to suppress tissues with short-to-intermediate T1 and T2 [Fig.1b]. In this study, we just replaced TFE-DIXON sequence to balanced-TFE DIXON sequence [Fig.1c] while keeping other pulse sequence design. Furthermore, we also applied 3D non-selective excitation pulses, which has already been demonstrated to improve the image quality of 3.0T bSSFP coronary MRA7.8, for balanced-TFE DIXON to shorten the TR/TE as much as possible. To validate the usefulness pf bREACT in the foot, we compared image quality, especially for the depiction of the blood vessels at the toe, among TOF, PC MRA, REACT, and bREACT using visual assessment which was performed by three radiologists/technologists. The assessment of toe blood vessels from the proximal to the distal be dividing segments with the joint as the boundary, and the evaluation of the blood vessels on a 5-point scale was performed [Figure 2]. Imaging parameters for respective MRA techniques are shown in Table 2.Results and Discussion
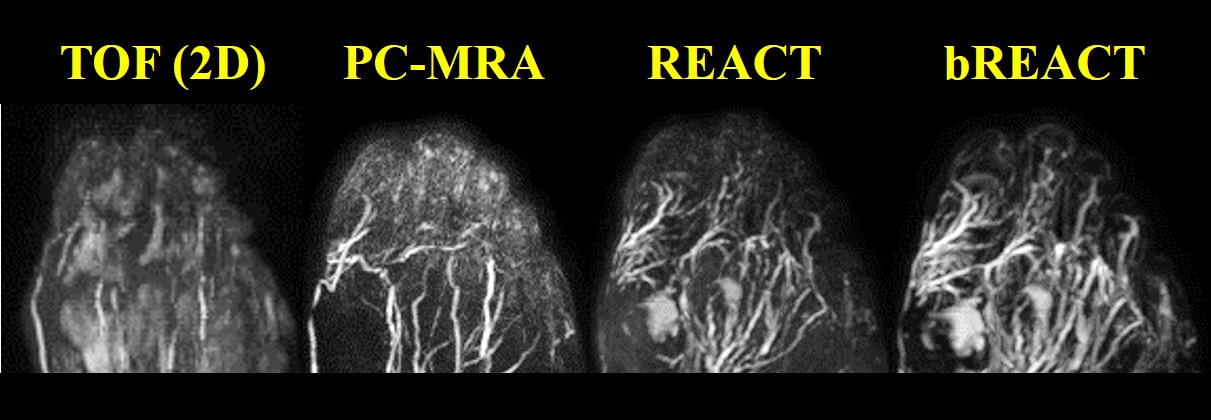
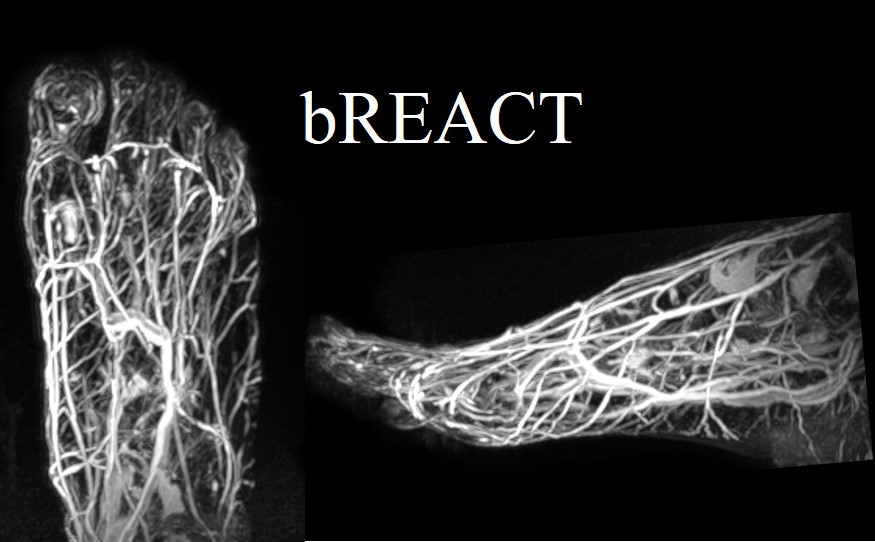
In visual evaluation, Area 1 and 2 could be well visualized by PC-MRA, REACT, and bREACT, but not visualized by TOF. In Area 3, REACT and bREACT well visualized all vessel structures, but TOF and PC-MRA poorly visualized the vessels. Finally, in area 4, bREACT well visualized all vessel structures, but other three methods poorly visualized the vessels. Representative MRA images at the toe with respective techniques are shown in Figure 3. The overall image quality of TOF was poor and the visual score was significantly lower than that of compared to other sequences because the inflow effect of the blood vessels of the toes is weak, unlike the head and neck. PC-MRA could not depict peripheral vessels consistently probably due to the difficulties of optimal flow velocity settings. In REACT, peripheral blood vessels were well visualized superior to the PC-MRA. Furthermore, bREACT could depict well even more peripheral blood vessels thanks to its substantially increased SNR. Since REACT an bREACT applies the difference in relaxation time independent to flow velocities, it should be needed further clinical evaluation in the diabetic patents whether such technique provides clinically useful information with high robustness.Conclusion
In this study we demonstrated the feasibility of dual-echo balanced SSFP-DIXON sequence with REACT technique for the foot MRA at 1.5T. bREACT dramatically increased the SNR compared to conventional REACT and it could provide excellent contrast between blood vessels and background tissues with high robustness compared with other conventional non-contrast-enhanced MRA methods. This technique would be helpful to assess peripheral blood vessels in the diabetic patients.Acknowledgements
No acknowledgements found.References
1. Forsythe RO, et al. Peripheral arterial disease and revascularization of the diabetic foot. Diabetes Obes Metab. 2015 May;17(5):435-44.
2. Zhang L, et al. Non contrast MRA of pedal arteries in type II diabetes: effect of disease load on vessel visibility. Acad Radiol. 2015 Apr;22(4):513-9.
3. Schubert T, et al. Non-enhanced, ECG-gated MR angiography of the pedal vasculature: comparison with contrast-enhanced MR angiography and digital subtraction angiography in peripheral arterial occlusive disease. European Radiology August 2016, Volume 26, Issue 8, pp 2705–2713
4. Cambria RP, et al. Magnetic resonance angiography in the management of lower extremity arterial occlusive disease : a prospective study. J Vasc Surg. 1997 Feb;25(2):380-9.
5. Liu X, et al. Unenhanced MR angiography of the foot: initial experience of using flow-sensitive dephasing-prepared steady-state free precession in patients with diabetes. Radiology. 2014 Sep;272(3):885-94.
6. Yoneyama M, et al. Free-breathing non-contrast-enhanced flow-independent MR angiography using magnetization-prepared 3D non-balanced dual-echo Dixon method: A feasibility study at 3 Tesla. Magnetic Resonance Imaging 2019 Aug 16;63:137-146
7. Kodaira K, et al. Acceleration of whole-heart coronary MR angiography using 3D non-selective bSSFP with Compressed SENSE. Proc. ISMRM:2019.2063
8. Shiina I, et al. Whole heart coronary MRA using non-selective balanced SSFP sequence at 3.0T: comparison of image quality. Proc. ISMRM:2019.2073
Figures