2152
Rapid diastolic-phase only TRANCE non-contrast MR angiography in screening of systemic artery aneurysm in patients with Kawasaki disease1Department of Radiological Technology, Tsuchiya General Hospital, Hiroshima, Japan, 2Philips Japan, Tokyo, Japan, 3Department of Pediatrics, Tsuchiya General Hospital, Hiroshima, Japan, 4Nitta Pediatric Clinic, Hiroshima, Japan, 5Department of Health Care, North Hiroshima Hospital, Hiroshima, Japan, 6Department of Radiology, Tsuchiya General Hospital, Hiroshima, Japan
Synopsis
The purpose of this study was to demonstrate the clinical feasibility and utility of diastolic-phase only ECG-triggered non-contrast-enhanced MR angiography (TRANCE) in screening of systemic artery aneurysms (SAA) in Kawasaki disease patients. Diastolic-phase only TRANCE provided consistent high image quality for evaluating main arteries in children with the average scanning time around 155sec in addition to routine coronary MRA screening. Diastolic-phase only TRANCE could be useful in SAA screening without significant prolongation of examination time.
Introduction
Kawasaki disease (KD) is an acute systemic vasculitis of medium sized arteries1. In particularly KD affects the coronary arteries but in approximately 2% of untreated patients, KD also causes systemic artery aneurysms (SAA).2 However, almost no screening of SAA for KD has been performed, and many reported modalities are x-ray angiography2 and computed tomography3. If coronary aneurysms and SAA could be evaluated simultaneously within the same examination by using non-contrast enhanced MRA, it will be non-invasive and ideal. To that end, it is necessary to acquire robust non-contrast MRA within a short scan time which could easily be added to the coronary examination. We focused on the diastolic-phase ECG-triggered non-contrast-enhanced MR angiography (TRANCE) 4, which visualizes both arteries and veins, but the scan time can be halved and it basically robust for magnetic field inhomogeneities and thus achieves wide field-of-view coverage. The purpose of this study was to investigate the feasibility of diastolic-phase only TRANCE as an additional scan of coronary MRA examination in screening of SAA in KD patients.Methods
Thirty one patients (2-33 years, mean 12.8 years) with KD underwent non-contrast-enhanced coronary MRA examinations (between December 2017 and October 2019) on a 1.5-T MRI clinical imager (Ingenia, Philips Healthcare, Best, The Netherlands) with Torso coil and/or Posterior coil. The diastolic-phase only TRANCE was used to assess the image quality of aorta, subclavian - brachial artery, renal artery and iliac artery. Imaging parameters were set as follows: TR 1090 - 2000 ms (2 heart rate); TE 56 - 74 ms (shortest); FOV 380-550 mm2; matrix 320 × 256; slice thickness 3.4 - 4.4 mm; number of slice 44-55; echo train length (ETL) 36-48; inversion time (TI) 165 ms; SENSE factor 1.5-2.0. The images were independently assessed to two pediatric cardiologists using visualization of 3-point scale (3 = excellent, 2 = acceptable, 1 = unacceptable) and evaluated the presence or absence of SAA. The average scanning time of the diastolic-phase only TRANCE was 155.5±34.0 sec.Results and Discussion
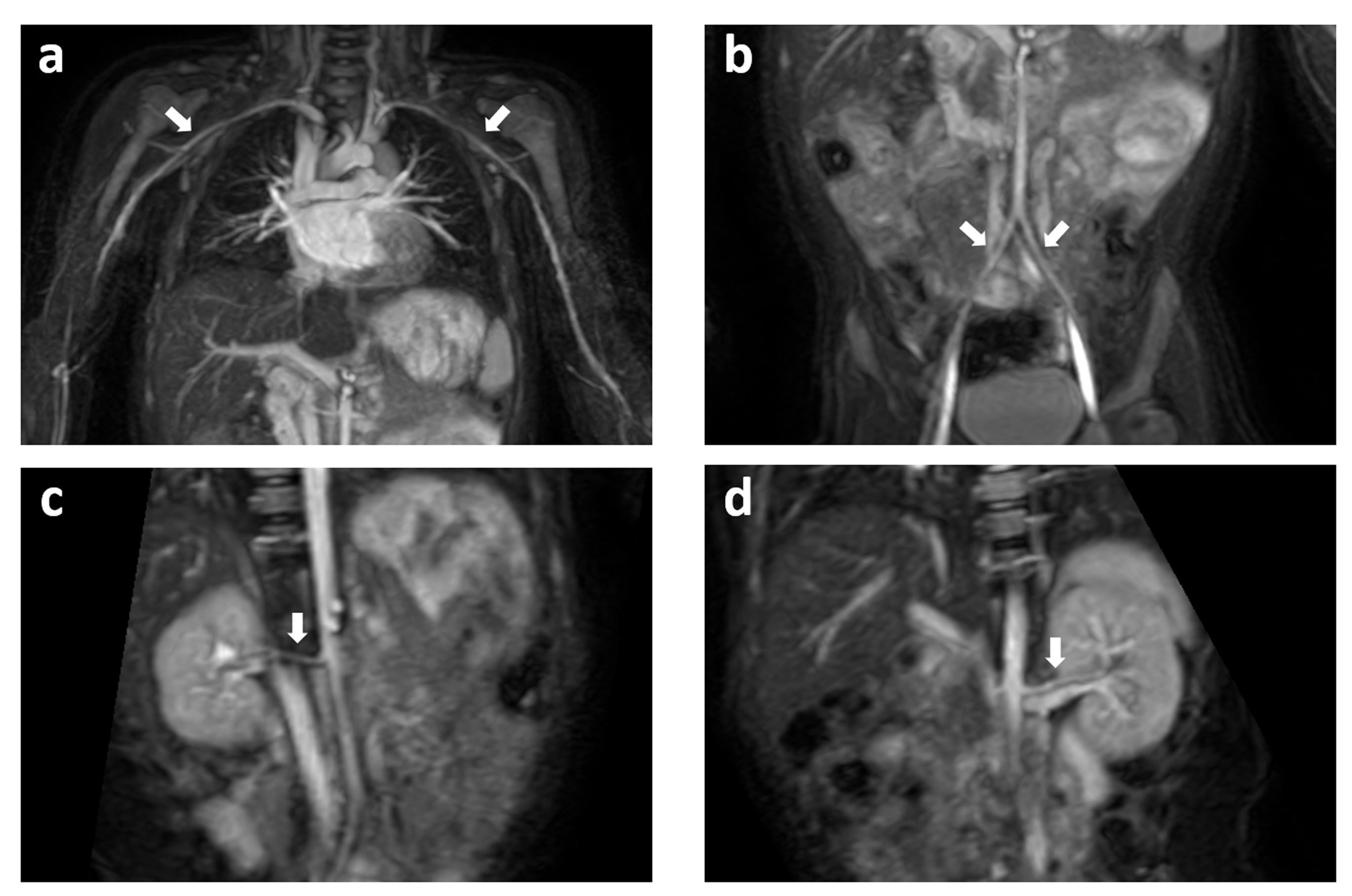
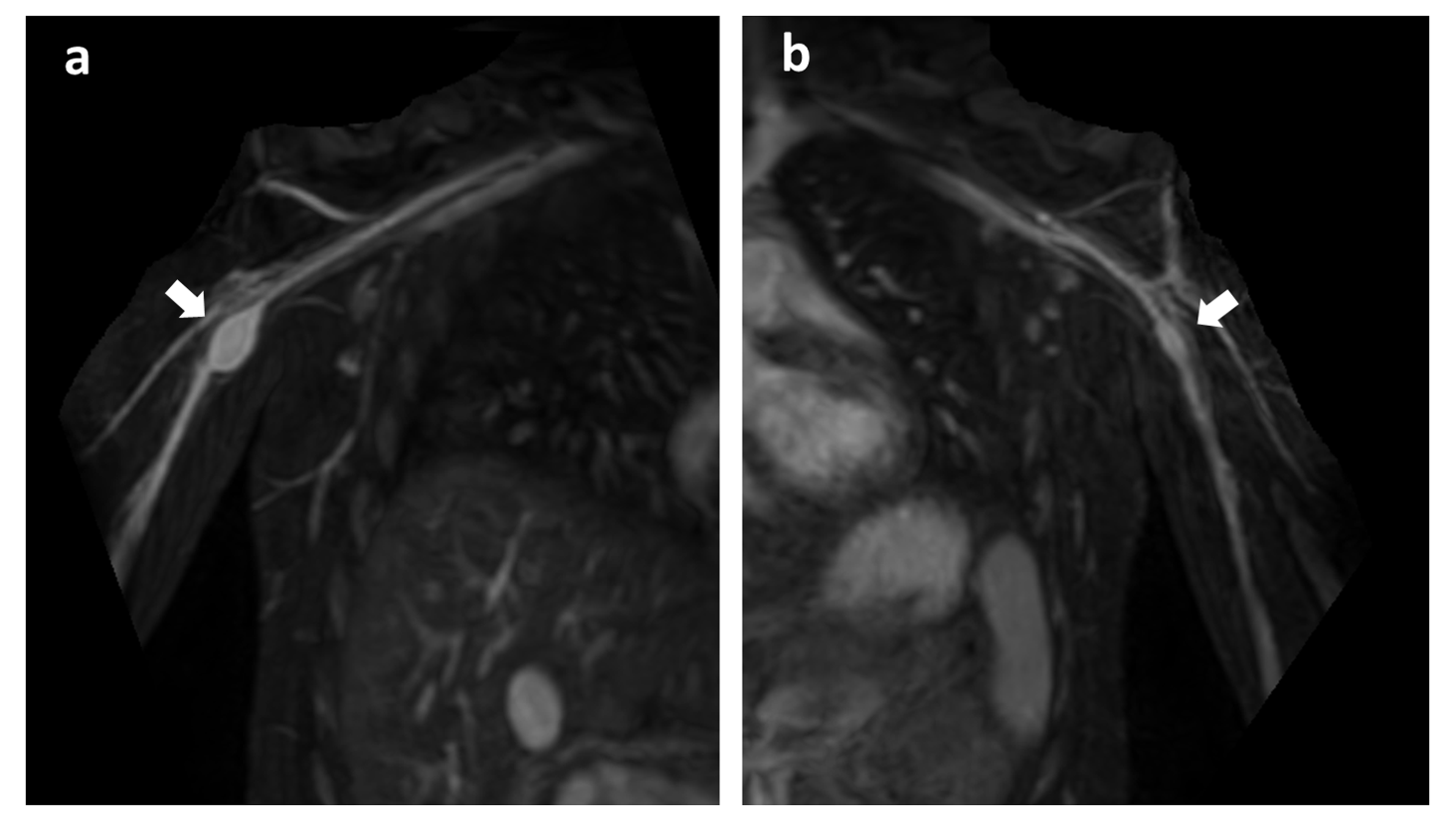
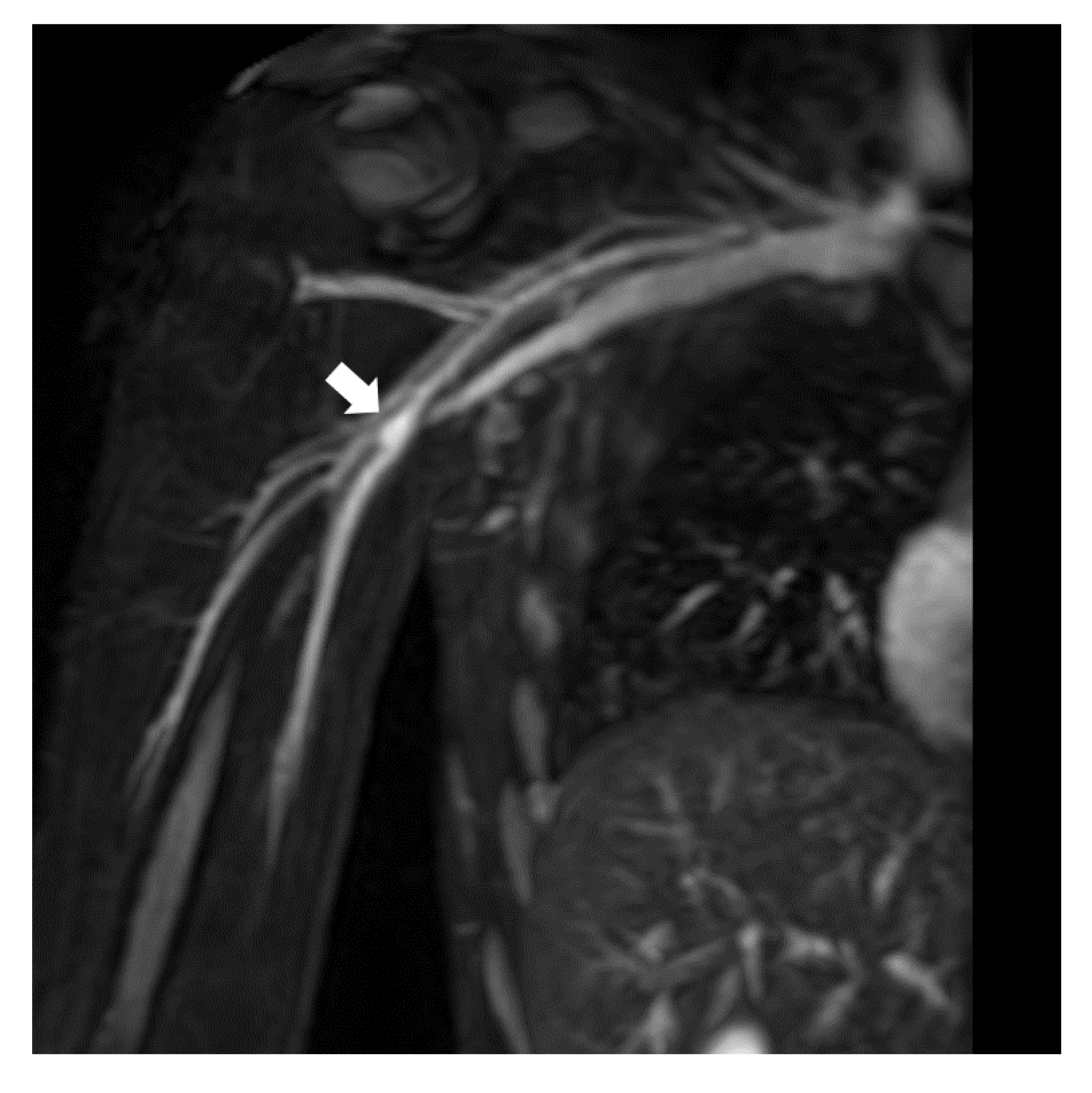
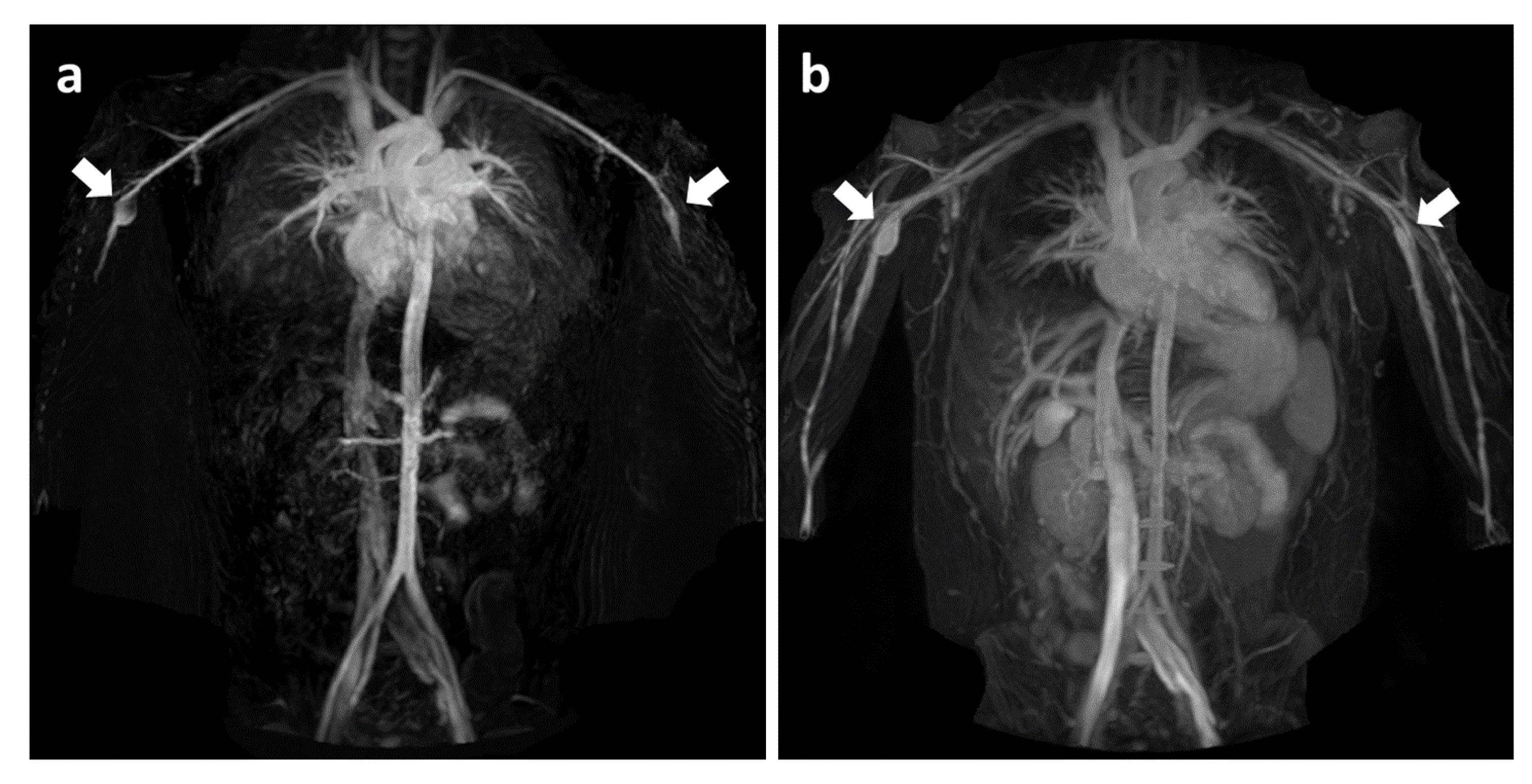
In 30 of 31 cases (96.8%) in aorta, in 30 of 31 cases (96.8%) in subclavian artery, in 26 of 30 cases (87.1%) in renal artery, in 29 of 31 cases (93.5%) in iliac artery, both readers evaluated the image quality of diastolic-phase only TRANCE was excellent or acceptable. Representative diastolic-phase only TRANCE images are shown in Figure 1. Although diastolic-phase only TRANCE depicted both arteries and veins, arteries could be well visualized by using multi-planar reconstruction. Representative clinical images of two patients with SAAs are shown in Figure 2 and 3. One patient had bilateral brachial artery aneurysms [Fig.2] and another patient had right brachial artery aneurysms [Fig.3]. Finally, Figure 4 shows the representative conventional (subtracted) TRANCE and diastolic-phase only TRANCE images. TRANCE basically requires both systolic and diastolic phase images to discriminate the arteries and veins by subtraction. In conventional TRANCE [Fig.4a], subtraction indeed improves the selective visualization of the arteries, but aneurysm was obscured by subtraction probably due to the presence of turbulent flow in the aneurysm. Although diastolic-phase only TRANCE depicted both arteries and veins, it well visualized the aneurysm [Fig.4b]. This would be one of the most clinical benefit for applying diastolic-phase only TRANCE for screening of SAA.Conclusion
This study has demonstrated the clinical usefulness of diastolic-phase only TRANCE, in addition to routine coronary MRA examination, in SAA screening without significant prolongation of examination time.Acknowledgements
No acknowledgement found.References
1. Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation 2004; 110:2747-71.
2. Kato H, Sugimura T, Akagi T, et al. Long term consequences of Kawasaki disease: a 10- to 21-year follow-up study of 594 patients. Circulation 1996;94:1379-85.
3. Kantarci M, Guven E, Ceviz N et al. Vascular imaging findings with high-pitch low-dose dual-source CT in atypical Kawasaki disease. Diagn Interv Radiol 2019;25:50-54.
4. Gutzeit A, Sutter R, Froehlich JM, et al. ECG-triggered non-contrast-enhanced MR angiography (TRANCE) versus digital subtraction angiography (DSA) in patients with peripheral arterial occlusive disease of the lower extremities. Eur Radiol 2011;21:1979–87.
Figures