2151
Non-Contrast-Enhanced MR Angiography of The Celiac Trunk Using 3D Magnetization-Prepared Dual-Echo Dixon in Free Breathing1Philips GmbH DACH, Hamburg, Germany, 2Diagnostic and Interventional Radiology, University Hospital RWTH Aachen, Aachen, Germany, 3Philips Japan, Tokyo, Japan
Synopsis
Contrast-enhanced MR angiography (CE-MRA) permits accurate assessment of the abdominal aorta and the splanchnic arteries, including the celiac trunk and its branches. However, it is often restricted for patients undergoing dynamic-contrast-enhanced imaging of the liver in the same exam. In this study, we employ the recently introduced Relaxation-Enhanced Angiography without Contrast and Triggering (REACT) method using magnetization-prepared dual-echo Dixon for 3D free-breathing non-contrast-enhanced imaging of the celiac trunk. Initial results in healthy volunteer and patients are reported in comparison to the other techniques such as the conventional and arterial spin labeling (ASL) based balanced steady-state free precession (bSSFP) sequences.
Introduction
3D contrast-enhanced MR angiography (MRA) has been established as a diagnostic tool for morphological assessment of the splanchnic arteries 1. However, it is often restricted for patients undergoing dynamic-contrast-enhanced imaging of the liver in the same exam. We aimed to investigate the clinical feasibility of using a recently introduced non-contrast-enhanced MRA (NCE-MRA) technique – REACT (Relaxation-Enhanced Angiography without Contrast and Triggering) 2 – for imaging of the celiac trunk, with comparison to the conventional approaches based on balanced steady-state free precession (bSSFP) sequences.Methods
REACT was based on magnetization preparation pulses of non-selective T2-prep and inversion recovery (IR), and data acquisition using 3D dual-echo turbo-field echo (TFE) Dixon with semi-flexible echo times 2. While the former suppressed tissues with short T1 and T2, thus enhancing the signal of native blood, the latter improved fat suppression over a large field of view. Previous results have shown uniform and robust blood-to-tissue contrast in multiple anatomies 2. For imaging of the celiac trunk, it was further modified with: (1) isotropic voxel size; (2) a longer T2-prep echo time of 70 ms for higher vessel-to-background contrast; (3) respiratory triggering; (4) compressed sensing reconstruction in combination of wavelet transformation and sensitivity encoding (SENSE) coil information (compressed SENSE or C-SENSE) 3. Figure 1A shows typical images of REACT after optimization. While (1) allowed for arbitrary multiplanar reconstruction (MPR), e.g. in all three orthogonal orientations (Fig 1B, C and D), (2) and (3) helped to further improve the conspicuity of the splanchnic arteries during free breathing, particularly the celiac trunk, as seen in the sagittal partial maximum intensity projection (MIP) (Fig 1E).For in vivo study all human subjects underwent MRI on a 1.5T whole-body clinical system (Philips Ingenia). Two additional bSSFP-based sequences were included for comparison: one conventional bSSFP turbo-field echo (bTFE), and one arterial spin labeling (ASL) based bTFE, also referred to as RAVEL (Repetitive Artery and VEnous Labelling) 4. Detailed imaging parameters were summarized in Table 1.
For image analysis, the general image quality and artifacts was evaluated for REACT in the obtained coronal plane as well as transversal MPR, and for conventional and ASL-based bTFE in the obtained transversal plane. This was done according to a semi-quantitative rating system: 4 = excellent, 3 = good, 2 = fair, 1 = poor. Vessel delineation was assessed in the sagittal MPR and partial MIP for all techniques using the same rating system. In addition, vessel-to-background contrast was evaluated by quantitative measuring the contrast-to-noise ratio (CNR) according to the equation CNR = (Mean blood – Mean background) / (SD blood 2 + SD background 2)1/2, where Mean and SD referred to mean values and standard deviations of the signal intensity measured inside the lumen area (blood) of the descending aorta (dotted circle in Fig 1C) and adjacent background (dashed circle in Fig 1C), respectively 5. Regions of interest (ROIs) were manually drawn in areas with uniform signal and without pathology or artifacts. For statistics paired t-test was used and a p value <0.001 was considered significant.
Results and Discussion
Four young healthy volunteers and 10 patients (45 ± 16 years, 4 female) with clinical indications for abdominal MRI were included. REACT was able to delineate the celiac trunk successfully in all cases, whereas conventional bTFE was susceptible to local field inhomogeneities caused by flows or residual abdominal motion, which led to inconsistent vessel delineation. Two examples are shown in Figure 2A and 2B, respectively. In addition, a 2D acquisition of the conventional bTFE failed to provide diagnostic image quality in the reformatted MPR, which was critical for morphological assessment. 3D ASL-based bTFE provided not only good vessel-background-contrast but also the advantage of artery selection only by combining with a labeling pre-pulse (Figure 3A). However, its generic bSSFP readout may still potentially pose a challenge to signal inconsistency; hence a detailed investigation will be needed. Moreover, five out of 9 patients were referred for 3D dynamic-contrast-enhanced (DCE) liver scans with Gadovist (Bayer AG, Leverkusen, Germany). A first post-contrast dynamic subtraction was performed. Although it did offer high-resolution in-plane vessel morphology with good contrast to the background, an anisotropic acquisition and potential motions between two dynamics led to certain blurring of the vascular structures, particularly in the reformatted MPR (Figure 3B).Furthermore, the (semi-)quantitative analysis confirmed the above image findings (Figure 4A), where conventional bTFE had the lowest rating in image quality and vessel delineation, compared to REACT and ASL-based bTFE (p <0.001). Although it presented a slightly higher CNR than REACT, the result was not significantly different and this was caused by the inconsistent image quality described above, as indicated by a wider SD. REACT revealed highest rating in image quality, but a relatively lower value in both vessel delineation and CNR, compared to ASL-based bTFE, without significant difference. Figure 4B shows one case of celiac trunk stenosis due to Dunbar syndrome, well depicted by REACT.
Conclusion
Initial results of NCE-MRA using REACT in healthy volunteer and patients for imaging of the celiac trunk and detection of associated vascular abnormalities are promising. Further studies are needed with larger cohorts to investigate its clinical performance compared to other MRA techniques.Acknowledgements
The authors thank Lucia Noël, Stephanie Tackenberg, and Chiara Morsch for their help in data acquisition.References
- Schneider G, Grazioli L and Saini S. MRI of the Liver: Imaging Techniques, Contrast Enhancement, Differential Diagnosis (2006) Springer, Italy.
- Yoneyama M, et al. MRI (2019) 63:137.
- Sartoretti E et al. Plos One (2019) 14:e0214887.
- Park SY, et al. Eur Radiol (2015) 25:533–540.
- Aubert B, et al. Magn Reson Imaging (1988) 6:195.
Figures
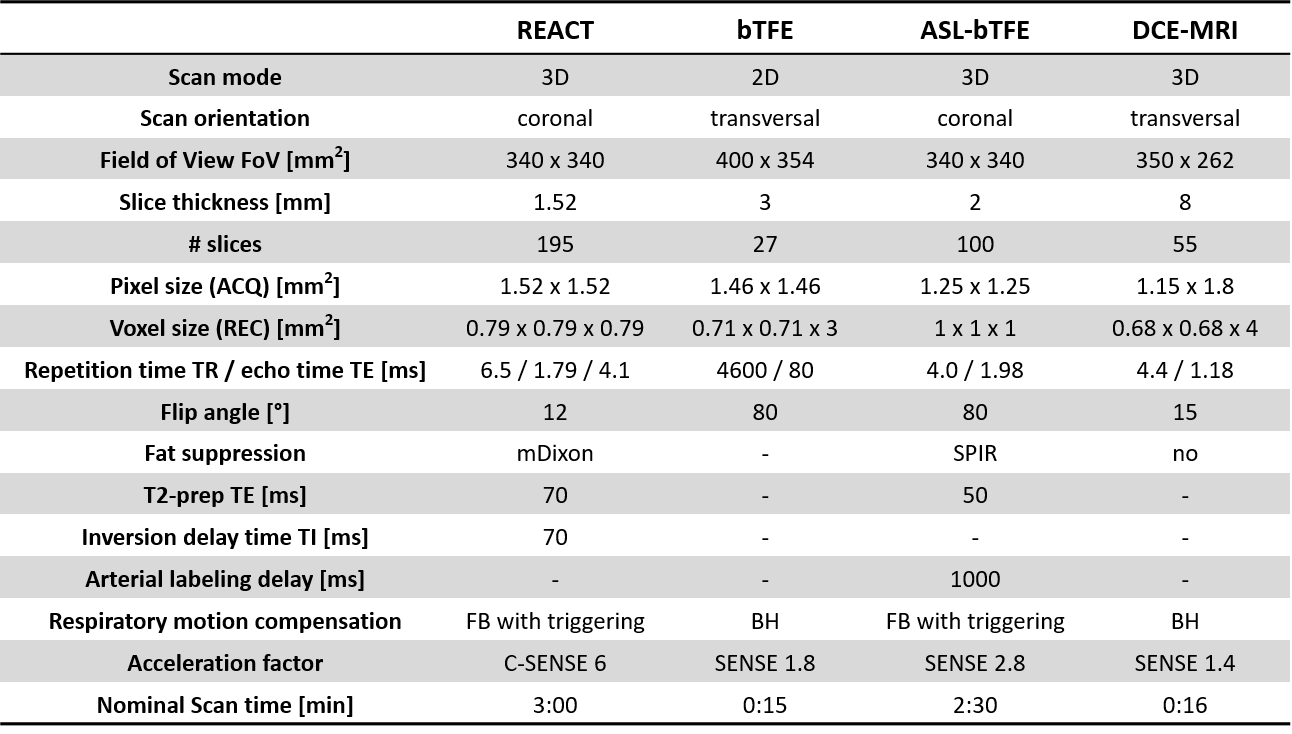
Table 1. Imaging parameters of the pulse sequences used in this study.
REACT = Relaxation-enhanced angiography without contrast and triggering; bTFE = balanced steady-state free precession turbo-field echo; ASL = arterial spin labelling; DCE = dynamic contrast enhanced; FB = free breathing; BH = breath hold; ACQ = acquired; REC = reconstructed; SENSE = sensitivity encoding; C-SENSE = compressed SENSE
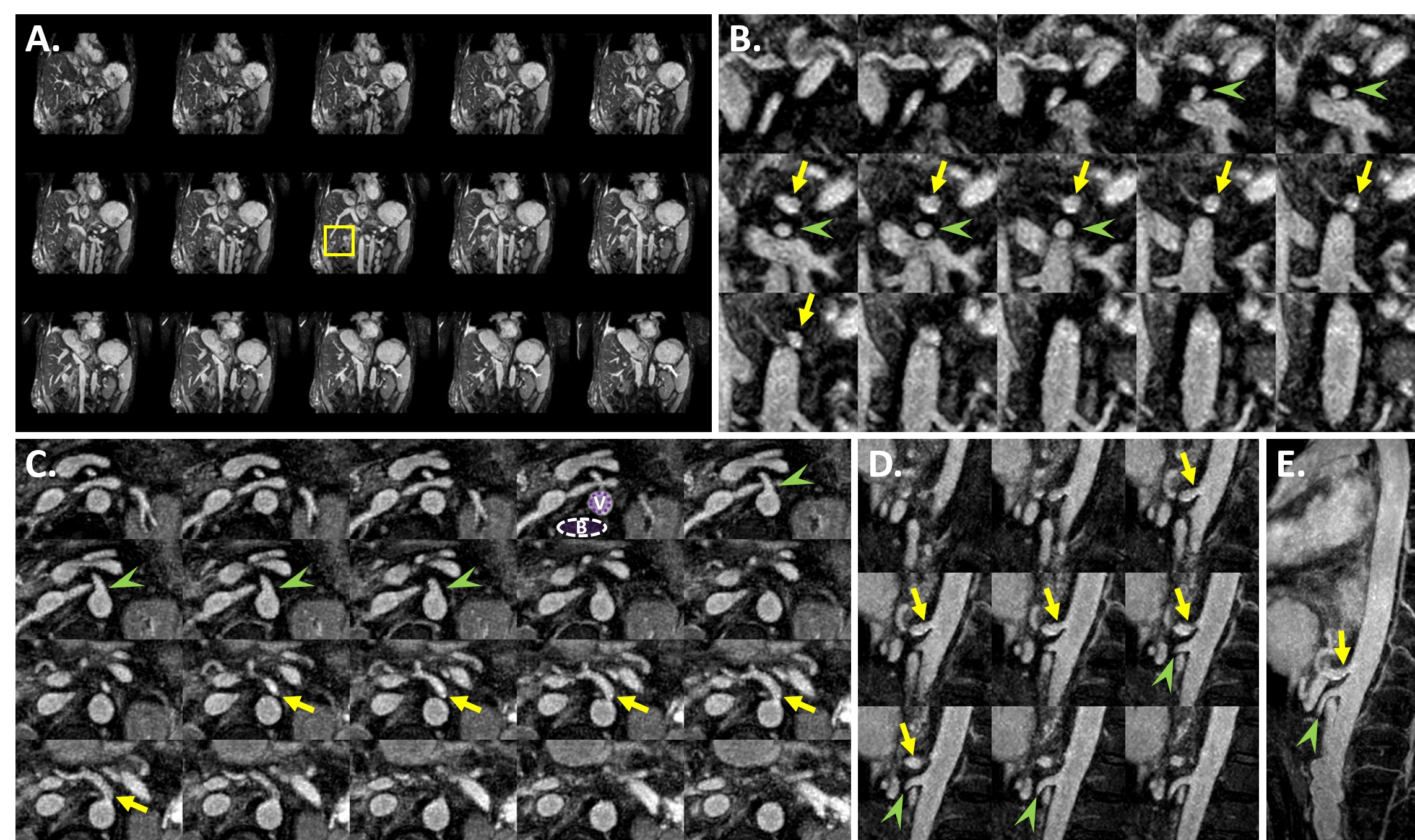
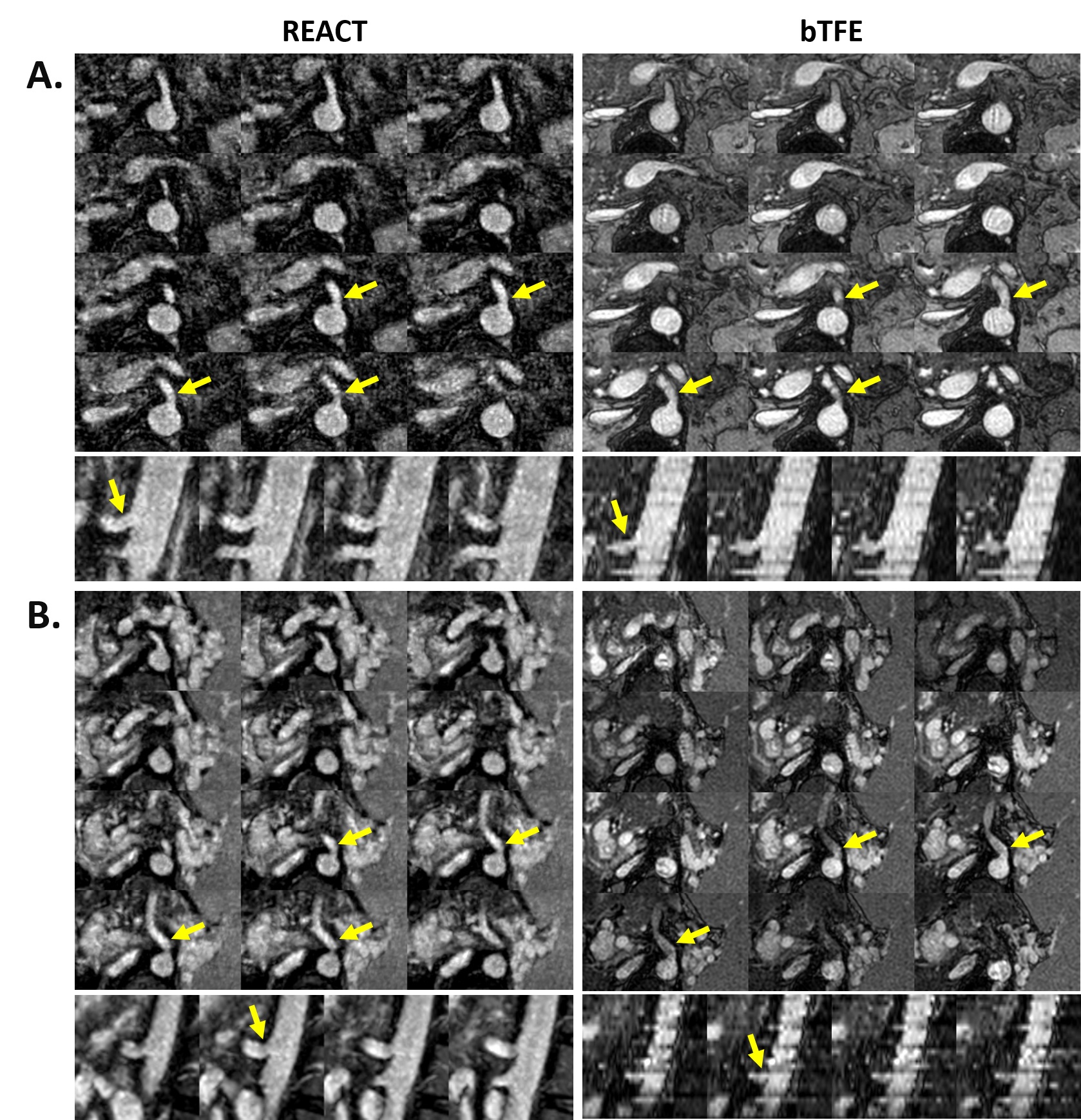
Figure 2. NCE-MRA of the celiac trunk using REACT (left) and conventional bTFE (right). While image quality of REACT was rated as excellent to good in both cases (A and B), bTFE was rated good (A) to fair (B) due to signal void and flow artifacts caused by the susceptibility differences. Selected images were presented in the transversal (1st row) and sagittal (2nd row) MPR. Neither of the patients presented symptoms of celiac trunk stenosis or vascular abnormality. Yellow arrows indicated the celiac trunk.
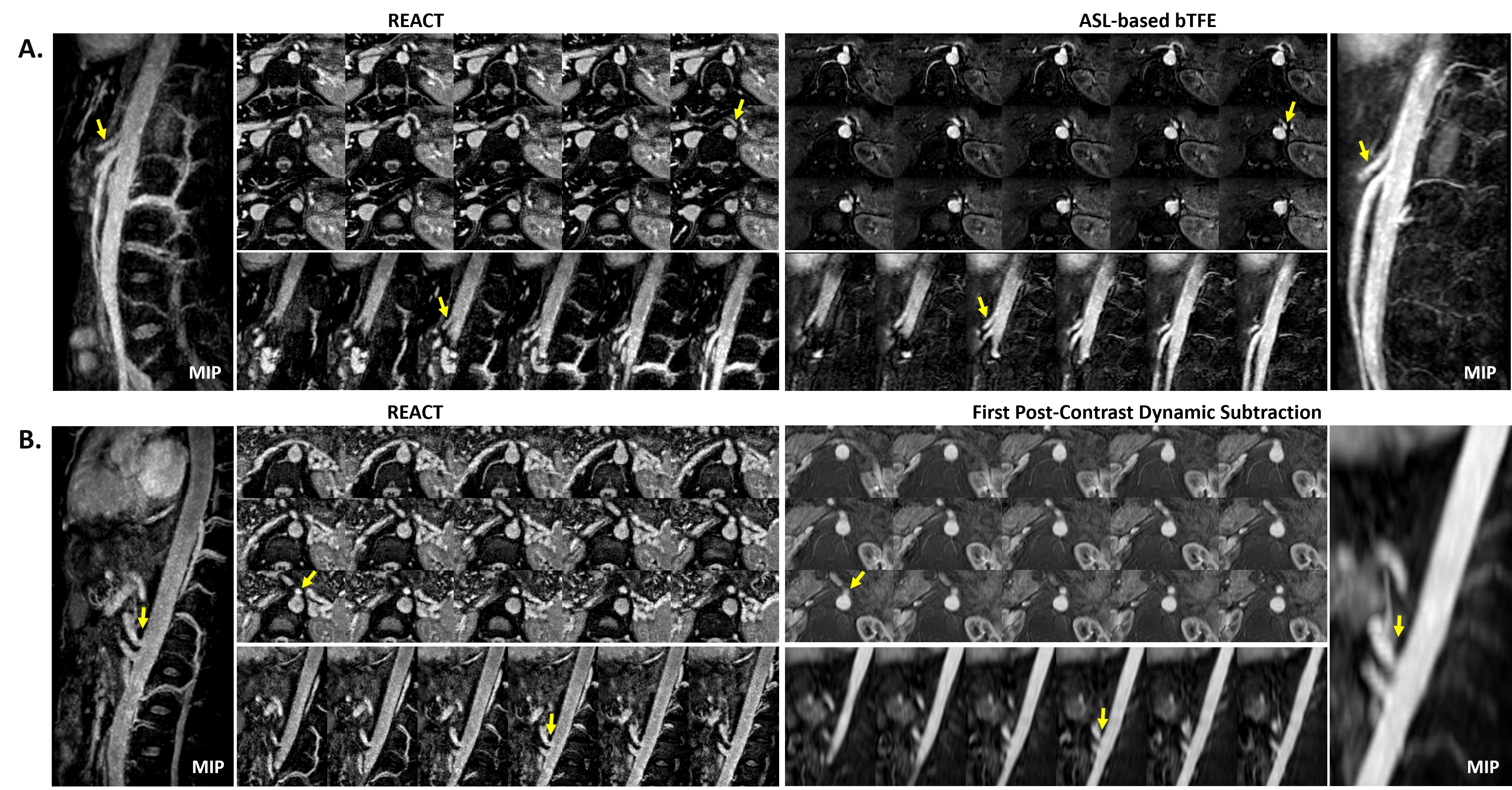
Figure 3. NCE-MRA of the celiac trunk using REACT (left) and ASL-based bTFE (top right), and in comparison to the first post-contrast dynamic subtraction (bottom right). Selected images were presented in the transversal (1st row) and sagittal (2nd row) MPR, respectively. Sagittal partial MIPs were indicated in the images. Neither of the patients in (A) and (B) presented symptoms of celiac trunk stenosis or vascular abnormality. Yellow arrows indicated the celiac trunk.
ASL = arterial spin labeling; bTFE = balanced steady-state free-precession turbo-field echo
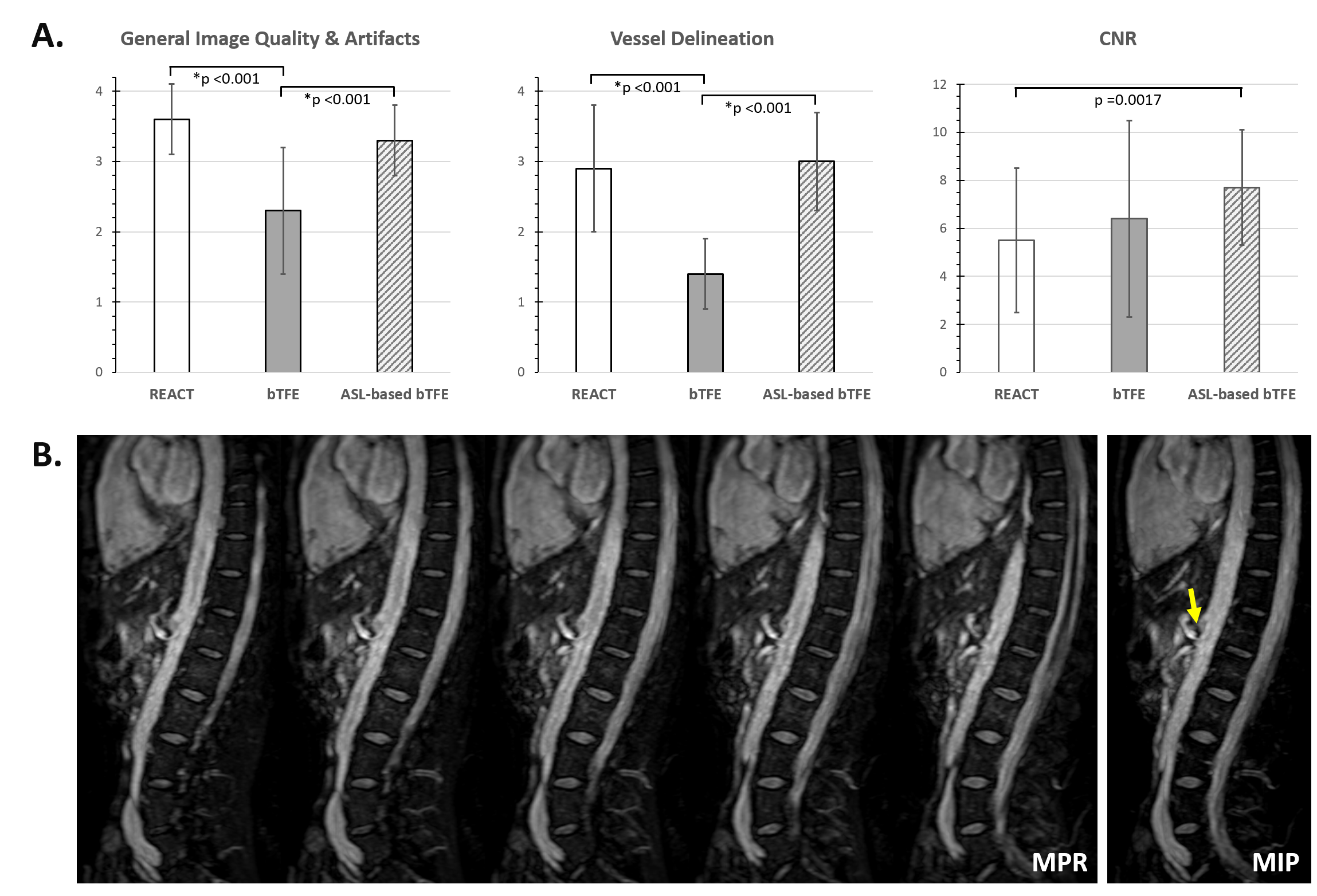
Figure 4. (A) Comparison of REACT, conventional and ASL-based bTFE in general image quality and artifacts, vessel delineation, as well as CNR (n = 9). (B) NCE-MRA of the celiac trunk using REACT in a human subject with stenosis. Selected images were presented in the sagittal MPR. Partial MIP was indicated in the image, and the yellow arrow indicated the celiac trunk stenosis.
MPR = multiplanar reconstruction; MIP = maximum intensity projection; ASL = arterial spin labeling; bTFE = balanced steady-state free-precession turbo-field echo; CNR = contrast-to-noise ratio.