2145
Whole heart coronary MRA with 3D non-selective bSSFP-DIXON: comparison with conventional methods
Kazuo Kodaira1, Michinobu Nagao2, Masami Yoneyama3, Yasuhiro Goto1, Isao Shiina1, Yutaka Hamatani1, Mamoru Takeyama1, Isao Tanaka1, and Shuji Sakai2
1Department of Radioligical Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
1Department of Radioligical Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
Improvement of fat suppression is important for whole heart coronary magnetic resonance angiography (WHC-MRA), because Unwanted signal arising from fat can compromise vessel delineation and decrease the diagnostic value of WHC-MRA. Balanced DIXON (bDIXON) can reduce fat suppression unevenness than SPIR method while maintaining high signal value. However, it is yet not applied for WHC-MRA. Furthermore, 3D non-selective bDIXON (3D NSbDIXON) with shortening TR can suppress an increase in imaging time. We propose a new sequence of 3D NSbDIXON for WHC-MRA, and examine the image quality in comparison to the conventional methods.
Introduction
Whole heart coronary magnetic resonance angiography (WHC-MRA) is a promising noninvasive method for detection of coronary artery disease1. WHC-MRA requires effective fat suppression because some coronary arteries are embedded in the epicardial fat2, 3. WHC-MRA typically applies SPIR pre-pulse, but it often obscured left circumflex artery (LCX) due to partial fat suppression failure. DIXON with spoiled gradient-echo (T1TFE-DIXON) improved the image quality of WHC-MRA compared to SPIR2. However, a limitation of T1TFE-DIXON at 1.5T is its lower signal-to-noise ratio (SNR). 3D balanced DIXON (3D bDIXON) has the possibility to solve these problems. By applying the balanced-TFE readout instead of T1TFE, it could increase the SNR, but it may suffer from banding artifacts. To prevent the increasing of banding artifacts, we applied 3D non-selective excitation pulses, which has already been demonstrated to improve the quality of 3.0T bSSFP WHC-MRA4, for balanced-TFE DIXON. 3D non-selective bDIXON (NSbDIXON) enables shortening TR (Fig. 1), resulting in decreasing the banding artifacts in addition to increasing the TFE factor during one heartbeat. Furthermore, 3D NSbDIXON has the potential to improve the effect of fat suppression compared to SPIR while ensuring high SNR thanks to bSSFP readout compared with conventional DIXON. Therefore, we hypothesized that 3D NSbDIXON can improve the image quality of WHC-MRA. In this study, we investigated the feasibility of 3D NSbDIXON for WHC-MRA by comparing with NSbTFE and non-selective T1TFE-DIXON (NST1TFE-DIXON).Methods
A total of six volunteers (6 males; age range: 26~44) were examined on a 1.5T MRI (Ingenia CX, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects. First, we compared the WHC-MRA images among 3D NST1TFE-DIXON, 3D NSbTFE-SPIR, and 3D NSbDIXON. Three sequences were acquired with navigator and cardiac triggering with the following parameters: FOV=350×350mm, voxel-size=1.5×1.5×1.5mm, C-SENSE_factor=7, TR/TE1/TE2/FA for NST1TFE-DIXON=5.3/1.73/3.6/20, for NSbTFE=2.3/1.14/NA/70, and for NSbDIXON=3.3/1.14/2.2/70. Curved Planer Reconstructions (CPRs) were performed using Ziostation2 (Ziosoft Co, Tokyo) and image quality was evaluated by visual score at the 10 points (RCA: #1, 2, 3, 4 LAD: #5, 6, 7, 8 CX: #11, 13) based on American Heart Association (AHA) classification. we evaluated them as 4-point grades (grade “4” was excellent, “1” was severe) by three blinded readers. For quantitative comparison, SNR and contrast-to-noise ratio (CNR) were measured. The SNR was assessed in the aorta and epicardial fat. To allow quantitative SNR measurements, we used a noise measurement method proposed by Zwanenburg et al5. Each sequence was repeated with exactly the same receiver gain, but without any RF and gradient pulses. The reconstructed images showed only noise, including the noise added due to the Compressed-SENSE (C-SENSE) reconstruction. The standard deviation of a region of interest of the corresponding area in the noise image was used as metric for the noise. SNRaorta and SNRepicardial fat were then calculated as follows: SNRaorta = SI (aorta) / SDnoise (aorta) SNRepicardial fat = SI (epicardial fat) / SDnoise (epicardial fat) where SI (aorta) and SI (epicardial fat) are the mean average signal intensity of the aorta and epicardial fat respectively, and the corresponding SDnoise is the standard deviation at the same location on the noise images. Subsequently, we measured the CNR for comparing image contrast quantitatively. The CNR was estimated for aorta and epicardial fat (CNRaorta-epicardial fat) and aorta and myocardium (CNRaorta-myocardium). The CNRaorta-epicardial fat and CNRaorta-myocardium were calculated by the following equations: CNRaorta-epicardial fat = [SI (aorta) - SI (epicardial fat)] / 0.5 [SDnoise (aorta) + SDnoise (epicardial fat)] CNRaorta-myocardium = [SI (aorta) - SI (myocardium)] / 0.5 [SDnoise (aorta) + SDnoise (myocardium)]. The SNR and CNR were assessed by wilcoxon signed-rank test.Results
Figure 2 and 3 shows the representative images using NST1TFE-DIXON, NSsbTFE and NSbDIXON. The results of visual score are shown in Figure 4. 3D NSbDIXON was significantly higher than NST1TFE DIXON and NSsbTFE regarding RCA, LAD, CX. Figure 5 shows the SNR and the CNR comparison among three sequences. For the SNRaorta, NSbTFE and NSbDIXON showed significantly higher value compared to NST1TFE-DIXON. In the SNRepicardial fat, NSbDIXON and NST1TFE-DIXON showed significantly lower value compared to NSbTFE. Furthermore, NSbDIXON showed significantly lower value compared to NST1TFE-DIXON. In the CNRaorta-epicardial fat, NSbDIXON showed significantly higher value compared to NSbTFE and NST1TFE-DIXON. In the CNRaorta-myocardium, NSbDIXON and NSbTFE showed significantly higher value compared to NST1TFE-DIXON.Discussion
From the results of SNR, it is considered that bDIXON provides higher SNR similar to conventional bSSFP compared with conventional DIXON. In addition, DIXON had a higher fat suppression effect than SPIR, and even a slight fat signal could be suppressed. Therefore, bDIXON has a lower epicardial fat signal value than bTFE, and bDIXON is considered to have an improved CNRaorta-epicardial fat over bTFE.Conclusion
WHC-MRA derived from 3D NSbDIXON has a higher blood signal than that of T1TFE-DIXON and a better contrast between arteries and background fat tissues than that of conventional bTFE-SPIR. This might improve the visualization of entire coronary arteries.Acknowledgements
No acknowledgements found.References
(1) Teresa Correia et al. Technical note: Accelerated nonrigid motion-compensated isotropic 3D coronary MR angiography. Med Phys. 2018 Jan; 45(1): 214-222. (2) Maryam Nezafat et al. Coronary MR angiography at 3T: fat suppression versus water-fat separation. Magn Reson Mater Phy. 2016; 29: 733-738. (3) Peter Bornert et al. Water/Fat-Resolved Whole-Heart Dixon Coronary MRA: An Initial Comparison. Magn Reson Med. 2014; 71: 156-163. (4) Isao Shiina, Kazuo Kodaira, et al. Whole-heart coronary MRA using Non-Selective balanced SSFP sequence at 3T: comparison of image quality. Proceedings of the 27th Annual Meeting of ISMRM (2019). (5) Zwanenburg et al. MR Angiography of the cerebral perforating arteries with magnetization prepared anatomical reference at 7T: comparison with time-of-flight. J Magn Reson Imaging. 2008; 28: 1519–1526.Figures
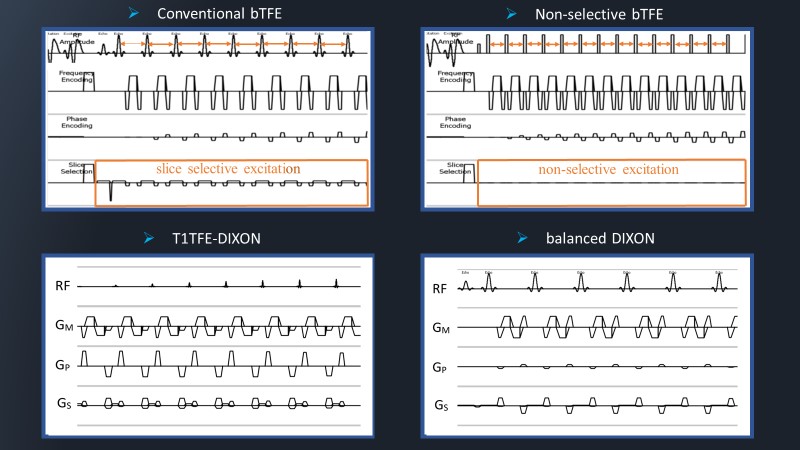
Figure 1: The sequence chart of conventional
bTFE, non-selective bTFE, T1TFE-DIXON and balanced DIXON (bDIXON). Non-selective bTFE enables shorter TR by not using
the slice selective excitation.
The bDIXON collects
echoes at two points while rephasing so that the sum of the gradient magnetic
fields of the three axes becomes zero. In this study, non-selective was
combined with three sequences of bDIXON, bTFE, and T1TFE-DIXON.
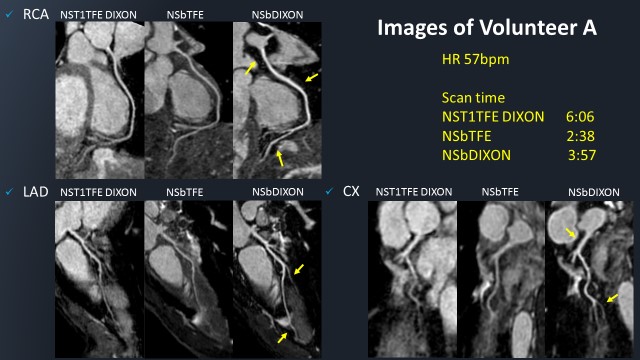
Figure 2: CPR
images of coronary artery of volunteer A
in NST1TFE DIXON, NSbTFE and NSbDIXON. Compared to NSbTFE using SPIR method,
the sequences using DIXON method had higher fat suppression effect and better
image contrast. Moreover, NSbDIXON has a higher blood signal value than NST1TFE
DIXON, so the distal blood vessels are more visible.
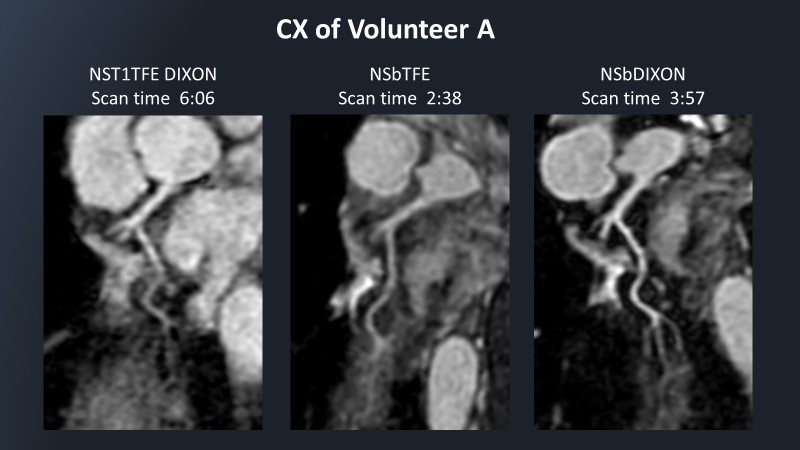
Figure 3: CPR
images of CX of volunteer A in NST1TFE
DIXON, NSbTFE and NSbDIXON. NSbDIXON showed CX much better than the other two
sequences.
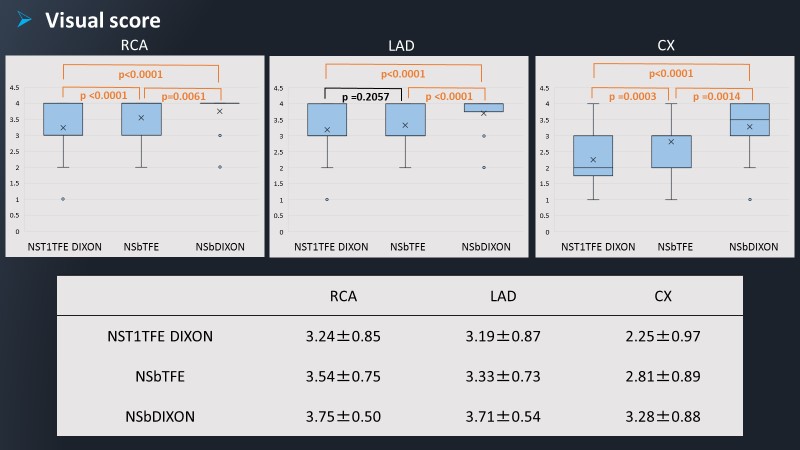
Figure 4: The
results of visual evaluation.
NSbDIXON was significantly
higher than NST1TFE DIXON and NSsbTFE
at RCA, LAD, CX (P <0.01). NSbTFE scored higher than T1TFE DIXON, and
significant differences were observed in RCA and CX (p <0.001).
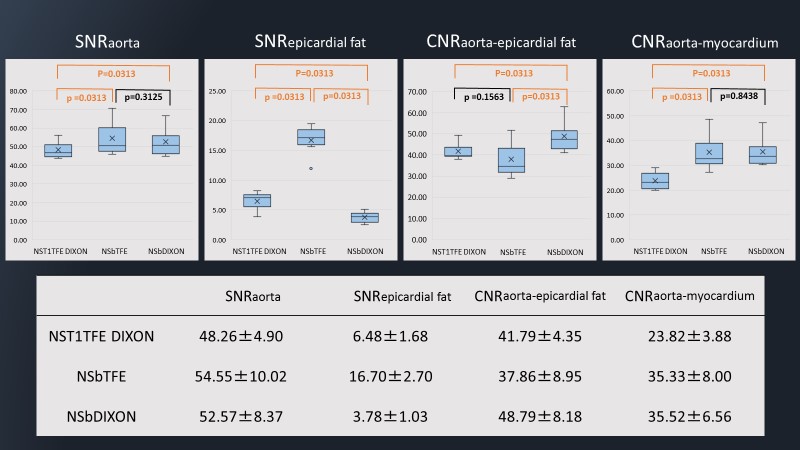
Figure 5: The results of SNR and
CNR. For the SNRaorta, NSbTFE and NSbDIXON showed
significantly higher value compared to NST1TFE-DIXON. In the SNRepicardial fat, NSbDIXON and NST1TFE DIXON
showed significantly lower value compared to NSbTFE.
Furthermore, NSbDIXON showed significantly lower value compared to NST1TFE-DIXON.
In the CNRaorta-epicardial fat, NSbDIXON showed significantly higher value compared to NSbTFE and
NST1TFE-DIXON. In the CNRaorta-myocardium, NSbDIXON and NSbTFE showed significantly higher value compared to
NST1TFE-DIXON.