2144
Improvement in 3.0 T whole-heart coronary MRA using the bSSFP method with a non-selective RF pulse1radiology, Tokyo metropolitan police hospital, Tokyo, Japan, 2Philips Japan, Tokyo, Japan
Synopsis
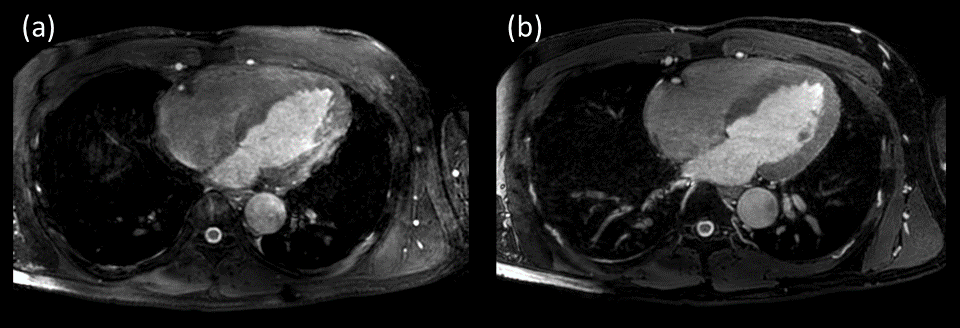
One of the problems of whole heart coronary MRA using bSSFP sequence at 3.0T is banding artifacts, caused by a long TR due to SAR limitations, resulting in degradation of image quality. A non-selective radio frequency (RF) pulse (e.g. block or hard pulse) enables to shorten the TR that leads to to reduce the banding artifacts. Hence whole heart coronary MRA using the bSSFP with non-selective RF pulse was improved image quality at 3.0T.
Introduction
Whole heart coronary MRA (WHC-MRA), using balanced steady-state free-precession (bSSFP) sequence with respiratory gating, is an established method for assessment of ischemic heart disease without contrast agents. One of the challenges of WHC-MRA at 3.0T is the banding artifact caused by the repetition time (TR) prolongation on the SAR limitation, and this leads to the deterioration of image quality. Alternatively, T1 turbo field echo (T1TFE) is also clinically used for WHC-MRA at 3.0T to prevent the banding artifacts, but its SNR is intrinsically low. Hence, bSSFP sequence is still needed even if it achieves good image quality at 3.0T. Recently, non-selective (non-sel) RF pulse with block pulse has been developed to enables shorter TR/TE which leads to reduce banding artifact for bSSFP WHC-MRA at 3.0T. In this study, we demonstrate the utility of bSSFP with non-sel RF pulses for WHC-MRA at 3.0T.Methods
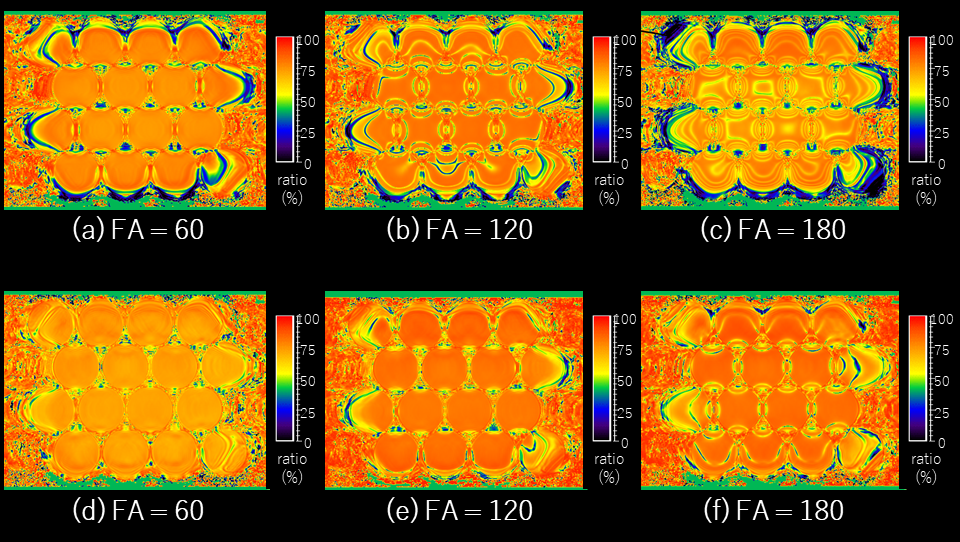
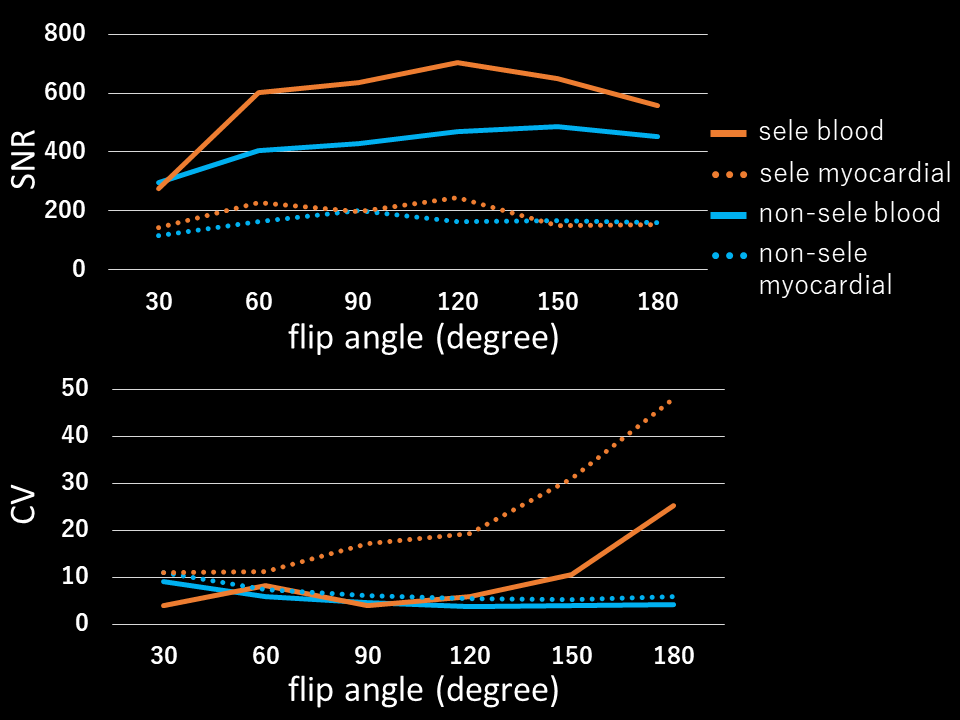
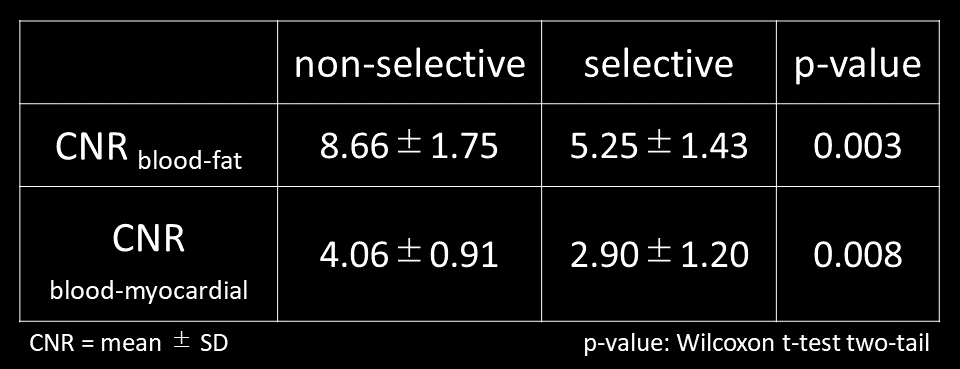
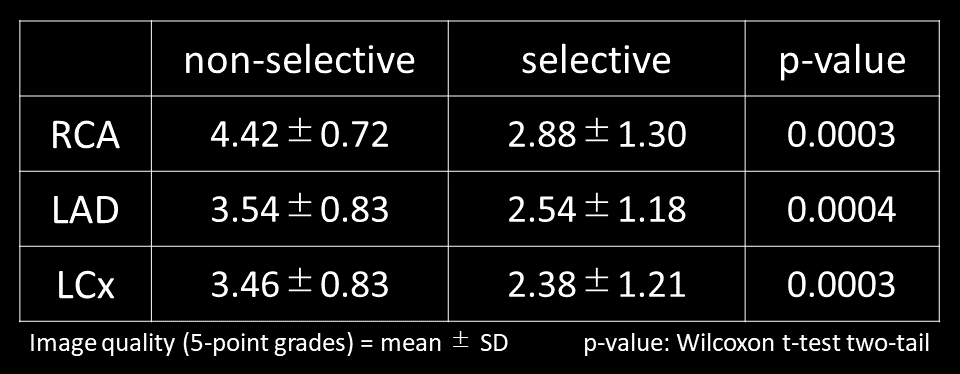
3.0T Philips MR system and 32-channel torso-cardiac coil were used in this study. The scan parameters was set based on volunteer experiments. The uniform coil performance test and blood / myocardial hand-made phantoms was used on phantom study, and 3D bSSFP sequences using selective / non-sel RF pulse were set to cover phantom by coronal slab orientation with the following parameters: FOV (mm) = 300×300, in-plane resolution (mm) = 1.53×1.57, slice thickness (mm) = 3.0mm/1.5mm overlap, TR/TE(ms) = 2.8~30/1.4~8.2 (selective); 2.1~5.4/1.05~2.2 (non-sel), SENSE factor = 2.0×1.5, shot interval(msec)= 1000, scan time=3:54 (selective); 2:52 (no-sel) and the flip angle (FA) was variable to increase 30 degrees from 30 to 180 degree. Images on were assessed by using signal to noise ratio (SNR); coefficient variation (CV); contrast ratio (CR) map for homogeneity, measured by signal intensity (SI) and standard deviation (SD). Using our institutional review board-approved procedures on clinical study, 10 volunteers underwent WHC-MRA with 3D bSSFP sequences using selective/non-sel RF pulses were set to cover whole heart by transverse and coronal slab orientation using navigator and vector cardiac gating with the following parameters: FOV (mm) = 300×350 , in-plane resolution (mm) = 1.34×1.35, slice thickness (mm) = 1.7mm/0.85mm overlap, TR/TE (ms) = 2.2~2.5/1.12~1.23, FA=60, SENSE factor =2.0×1.5, low-high-radial, TFE factor=25, startup echo=6, water fat shift (pixel/Hz)=0.23, T2prep (msec)=50, refocusing=2, SPIR, NSA = 1, scan time= 3:49~6:56 (depend on heart beat). For the evaluation of CNR (CNR blood-fat, blood-myocardial) was measured by blood, fat and myocardial SI and SD. The image quality for three vessels on banding and blurring artifacts, we evaluated using 5-point grades (grade “5” was absent, “1” was severe) by three blinded readers.Results
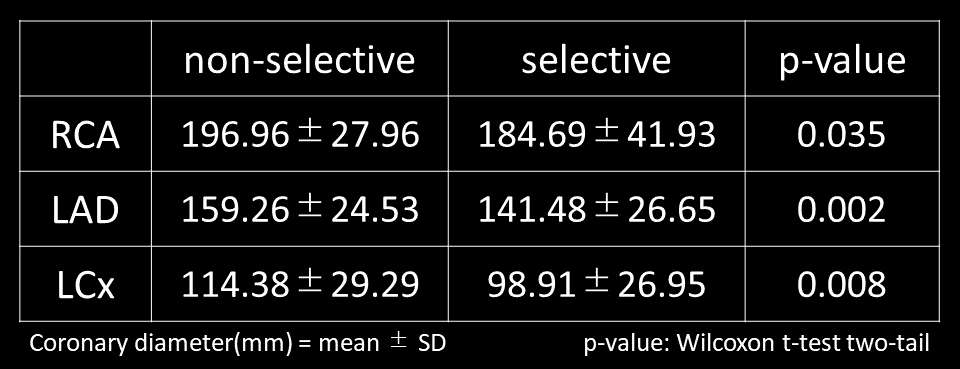
The SNR on phantom study of non-sel RF pulse was lower than that of selective RF pulse bSSFP sequence, and increasing FA improved CV. The CR maps of non-sel RF pulse was at least similar on small FA, and to improve than that of selective RF pulse in high FA. The CNRs on clinical study using non-sele RF pulse were significantly higher than that of sels RF pulse (CNR blood-fat: P= 0.003, CNR blood-myocardial: P=0.008). The image quality of non-sel RF pulse were better than sel RF pulse (RCA: P=0.035, LAD: P=0.002, LCx=0.007). Although non-sel RF pulse was shorter scan time by shorten TR, it could effectively suppress aliasing artifacts with wide-coverage coronal orientation.Discussion
The non-sel RF pulses on 3.0T significantly improved the SNR, CV and CR compared to conventional selective RF pulses by adopting a very short block pulse shape without slice selective gradients and it enables shortening TR/TE with the same in-plane resolution.Conclusion
In conclusion, a non-selective RF pulse using the 3D-bSSFP sequence can improve the image quality of 3.0 T WHC-MRA without scan time extension while preventing banding and blurring artifacts.Acknowledgements
No acknowledgement found.References
1. Weber O. M., Alastair J. M., Charles B. H. Whole-heart steady-state free precession coronary artery magnetic resonance angiography. Magn Reson Med. 2003; 50(6): 1223-1228.
2.Carr H.Y. Steady-state free precession in nuclear magnetic resonance. Physical Review 1958; 112(5): 1693-1701.
3. Foxall D. L. Frequency-modulated steady-state free precession imaging. Magn Reson Med. 2002; 48(3): 502-508.
4.Zur Y., Stokar S., Bendel P. An analysis of fast imaging sequences with steady-state transverse magnetization refocusing. Magn reson med. 1988; 6(2): 175-193.
5. Vasanawala S. S., Pauly J. M., Nishimura D. G. Linear combination steady-state free precession MRI. Magn Reson Med. 2000; 43(1): 82-90.
6. Nayak K. S., Lee H. L., Hargreaves, B. A, et al. Wideband SSFP: alternating repetition time balanced steady state free precession with increased band spacing. Magn Reson Med. 2007; 58(5): 931-938.
7. Moore J., Jankiewicz M., Anderson A. W, et al. Evaluation of non-selective refocusing pulses for 7 T MRI. J Magn Reson. 2012; 214: 212-220.Figures