2142
3D whole heart CMRA using an image-navigator framework – a clinical comparison study with CCTA and diaphragmatic navigators1Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Conventional diaphragmatic navigator coronary magnetic resonance angiography (d1D-NAV-CMRA) is limited by long and unpredictable acquisition-times and motion related image quality degradation. To overcome these challenges, we have previously proposed an image-navigated non-rigid motion-compensated, undersampled reconstruction CMRA framework (iNAV-CMRA) with <10min acquisition times. Here we investigated the clinical feasibility of 1.2mm3 iNAV-CMRA, comparing its performance, in patients with suspected coronary artery disease, against 1.2mm3 d1D-NAV-CMRA and coronary computed tomography angiography (CCTA). Compared to the d1D-NAV-CMRA, the iNAV-CMRA had a shorter acquisition-time(7:24±0:33min vs. 21:02±7:27min, p<0.0001), with improved coronary vessel-length, vessel-sharpness and image-quality-score, and visually comparable to CCTA.
Main Abstract
INTRODUCTION: Coronary computed tomography angiography (CCTA) is the established clinical gold standard non-invasive imaging modality for the anatomical assessment of coronary artery stenosis. However, it is limited by the long-term cumulative risk of ionising radiation and short-term risk of iodine-contrast mediated nephropathy. Furthermore, in the presence of significant coronary calcification, its evaluation accuracy is reduced as a result of hard beam and calcium blooming artifacts. Coronary magnetic resonance angiography (CMRA) has the potential to offer a non-invasive, ionising radiation and contrast free alternative to CCTA for the assessment of coronary stenosis. However, despite the recent progress in free breathing 3D whole heart CMRA sequences, widespread application remains limited to niche clinical situations. This is largely due to lower spatial resolution compared to CCTA ( ≈ 1mm vs. 0.5mm), prolonged and unpredictable acquisition times, low scan efficiency and residual respiratory motion artefacts associated with 1D diaphragmatic navigator (d1D-NAV) gating. To overcome some of these limitations, we have recently integrated highly undersampled acquisitions with image based navigators (iNAV) and non-rigid motion correction (iNAV-CMRA) to enable free breathing, non-contrast 3D whole heart CMRA with 100% respiratory scan efficiency in a clinically feasible acquisition time of under 10 minutes (1-3). Here, we investigated whether the iNAV-CMRA framework could improve the visualisation of coronary arteries compared with the conventional d1D-NAV CMRA in patients with suspected coronary artery disease (CAD) who were referred for a clinical CCTA.METHODS: Eleven patients with suspected CAD were recruited for CMRA on a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Two separate non-contrast CMRA datasets were acquired in each patient with the use of nitrates and beta-blockers in line with standard clinical CCTA recommended practice. A 2.5-fold accelerated 1.2mm3 isotropic resolution iNAV CMRA was acquired first. With this sequence, a 2D iNAV (1) was performed (exploiting the start-up echoes of the 3D bSSFP CMRA scan) to enable beat-to-beat 2D translational and bin-to-bin 3D non-rigid respiratory motion compensated (2) undersampled reconstruction3of the heart with 100% respiratory scan efficiency (4). With the second sequence, a conventional (2-fold GRAPPA accelerated) 1.2mm3 isotropic resolution d1D-NAV CMRA was acquired with foot-head (FH) translational motion correction and a ±3.5mm respiratory gating window (gated and tracked). Vessel length and sharpness (for the first 4cm and full length) of the right coronary artery (RCA), left anterior descending artery (LAD) and left circumflex artery (LCx) were measured and compared after reformatting with dedicated software for CMRA analysis (5). A vessel sharpness of 100% marks an abrupt change in signal intensity whereas a sharpness of 0% indicates the absence of an edge. A 4-point image quality score (where 1: indicates uninterpretable CMRA images, 2: poor image quality (blurred edges, noise and residual artifacts), 3: acceptable image quality (vessels adequately visualised, only mildly blurred edges), 4: excellent image quality with sharply defined coronary borders) was performed by an independent expert with CMR level III accreditation and more than 15 years of experience in clinical CMR who was blinded to the patient information and acquisitions. All statistical analyses were performed using GraphPad Prism version 8 software.
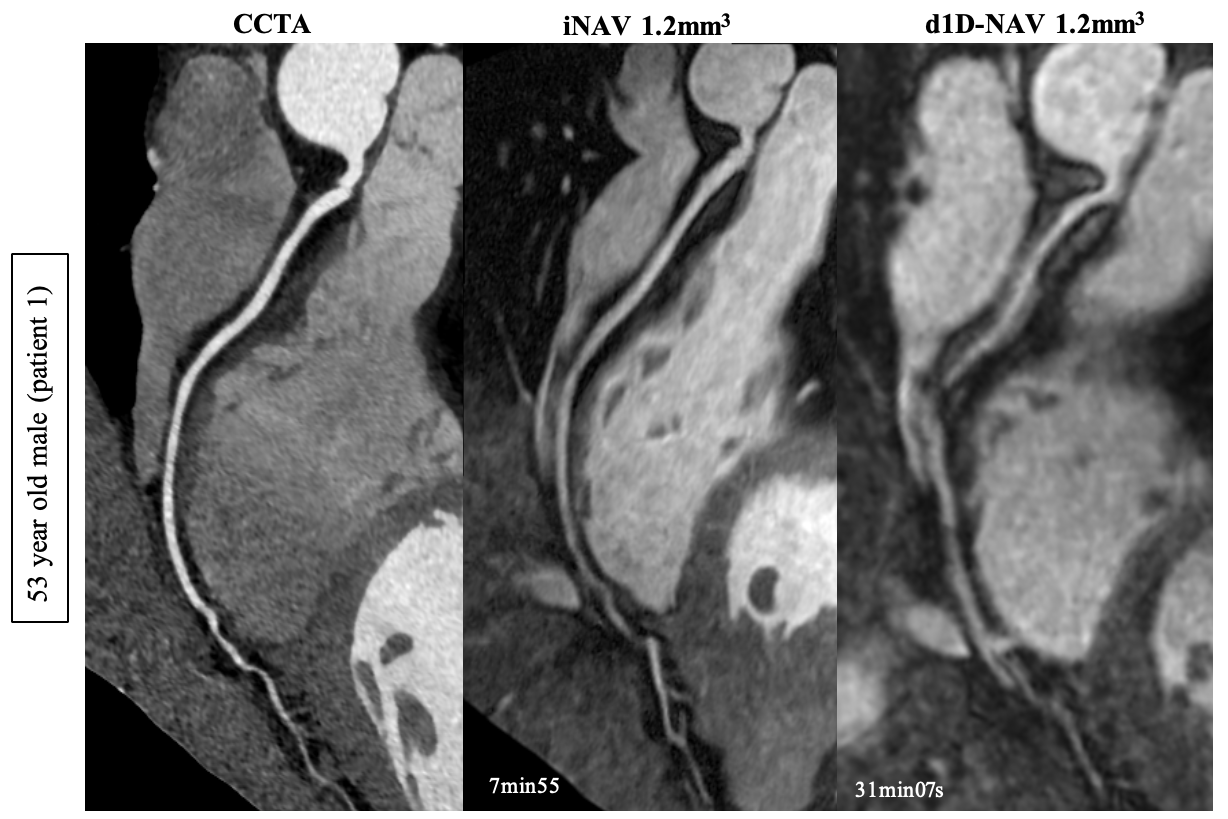
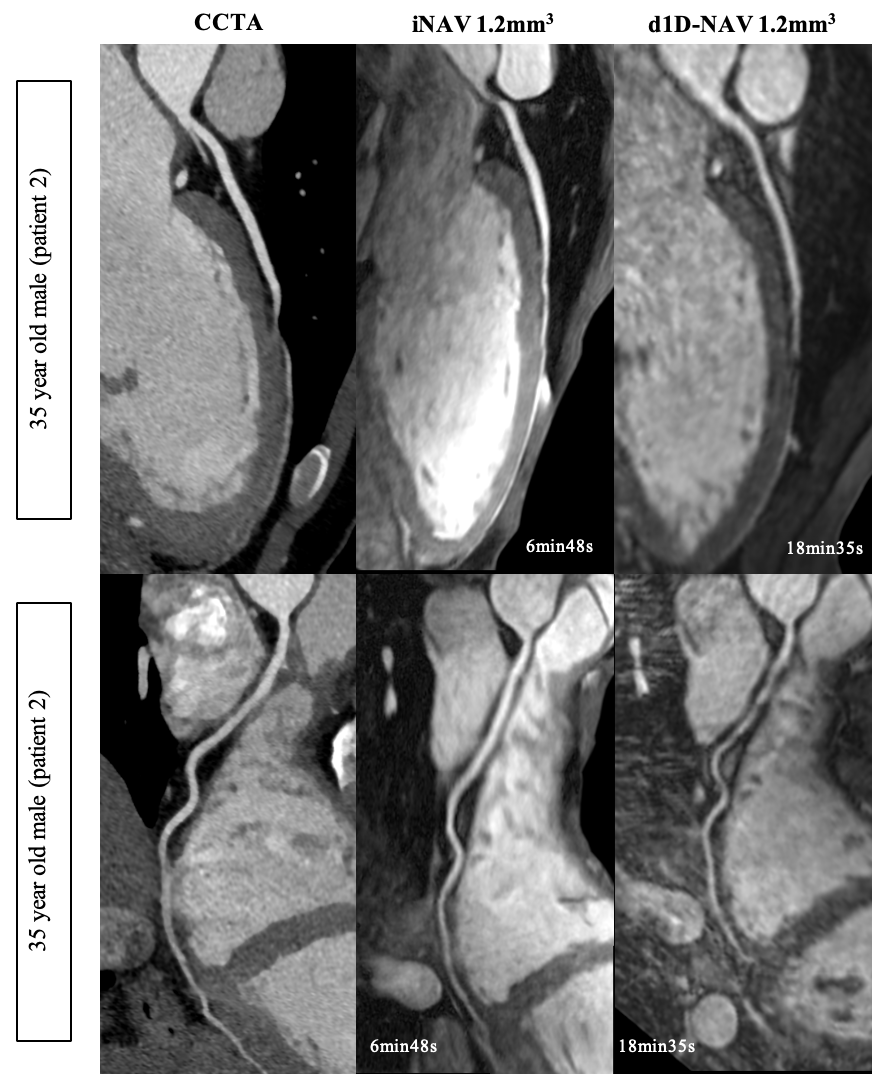
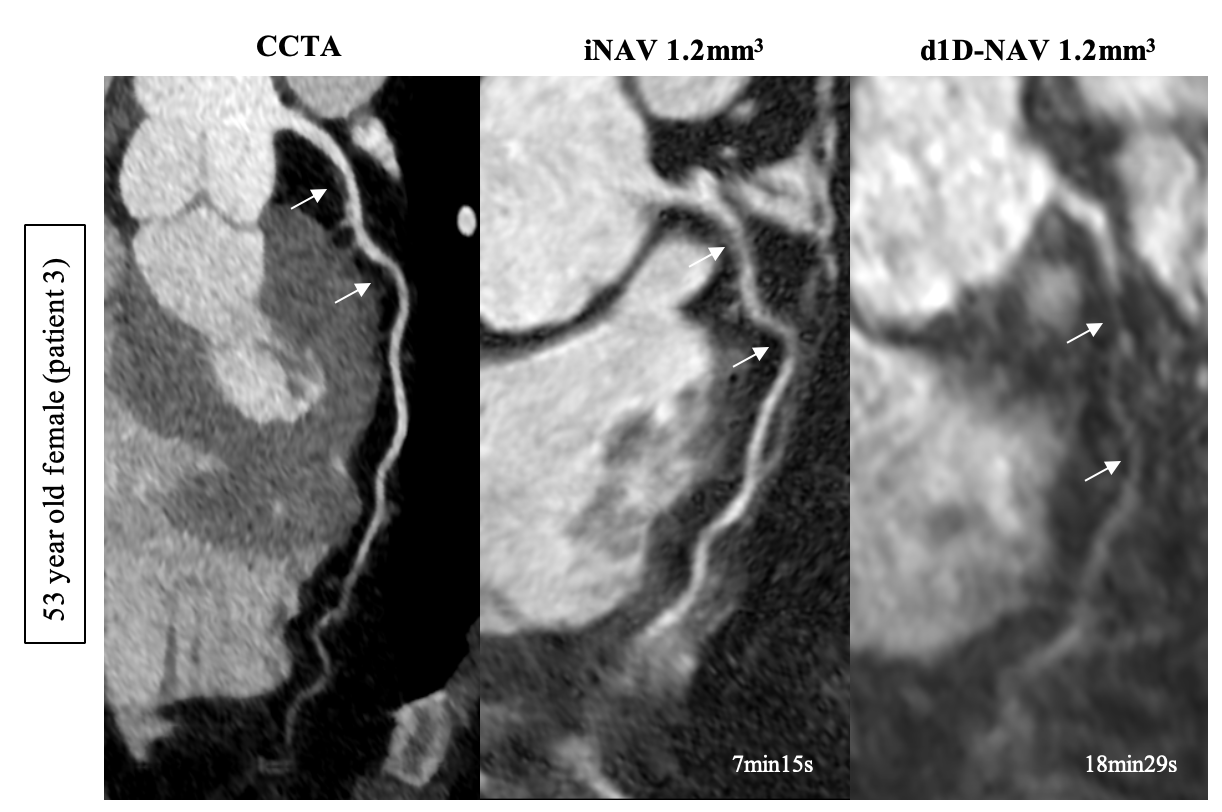
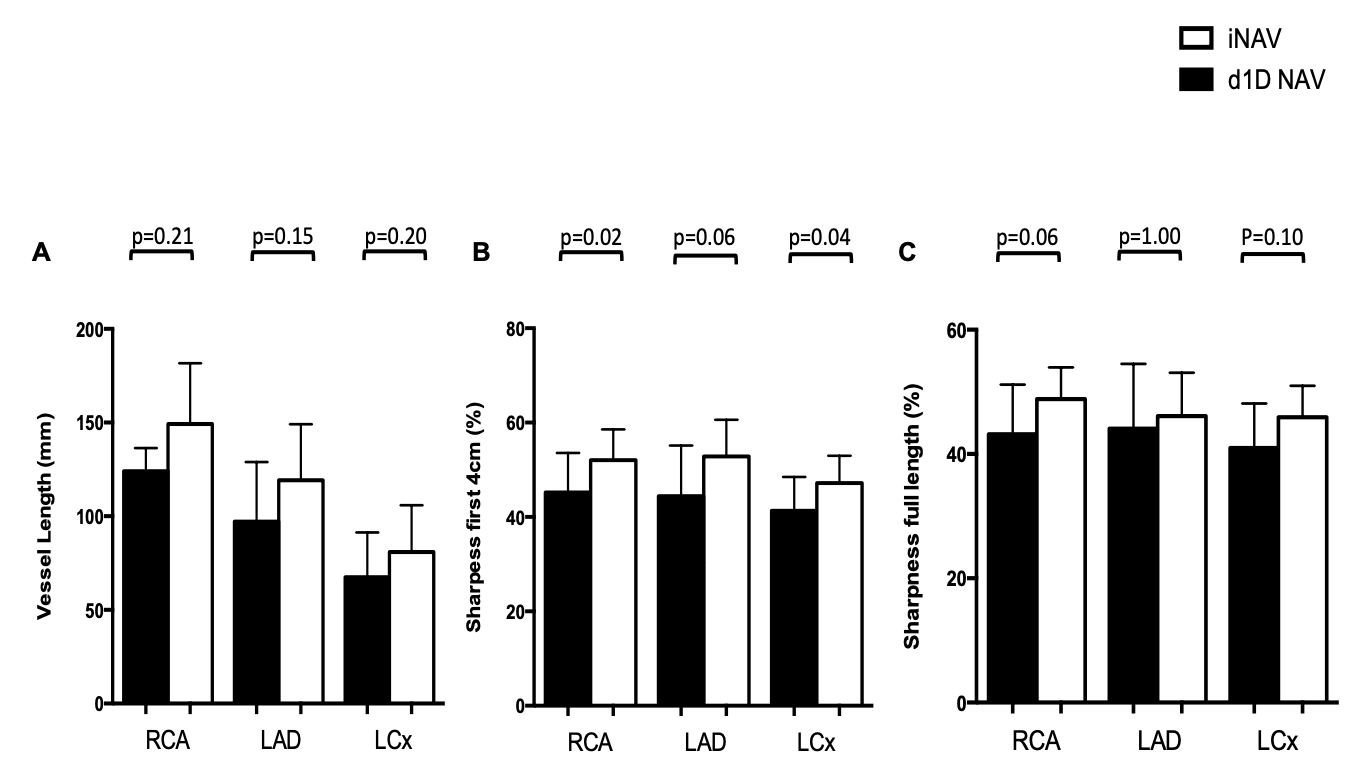
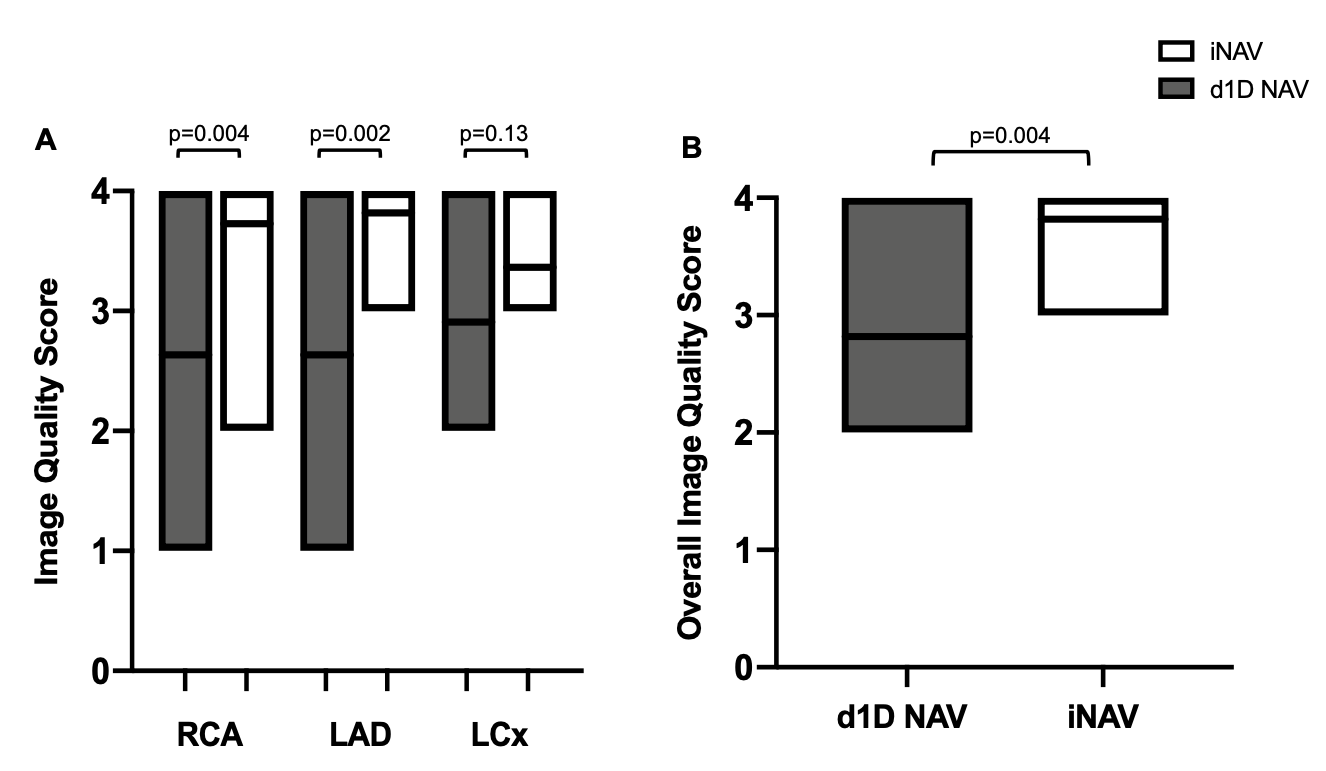
RESULTS: The average scan time for the iNAV-CMRA was significantly shorter compared to the d1D-NAV-CMRA (7:24 ± 0:33 min vs. 21:02 ± 7:27 min, p<0.0001). The respiratory scan efficiency of the iNAV-CMRA was 100% compared to 44% with the d1D-NAV CMRA (p<0.0001). The iNAV CMRA images show an excellent delineation of the coronary vasculature, visually comparable to that of CCTA (Figures 1, 2 and 3). In comparison to the d1D-NAV-CMRA, visible vessel length was improved with the iNAV-CMRA in all three coronary arteries (Figure 4). Compared to the d1D-NAV-CMRA, vessel sharpness was improved with the iNAV-CMRA in all three coronary arteries, which was statistically significant for the RCA and LCx in the proximal 4cm (p=0.02 and p=0.04 respectively) (Figure 4). The image quality score was significantly improved with the iNAV-CMRA for the RCA, LAD and overall 3D dataset (p=0.004, p=0.002, and p=0.004 respectively) (Figure 5).
CONCLUSION: In this preliminary clinical comparison study of patients with suspected CAD who were referred for a CCTA, the iNAV-CMRA framework was superior to the conventional d1D-NAV-CMRA in terms of coronary vessel length, vessel sharpness and image quality score despite a significantly shorter acquisition time. The reformatted visual image quality was comparable to that of CCTA. Larger clinical validation studies in patients with suspected CAD with the use of nitrates and beta-blocker is now warranted.
Acknowledgements
No acknowledgement found.References
1. Henningsson M., Koken P., Stehning C., Razavi R., Prieto C. and Botnar R. M. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn. Reson. Med.67,437–445 (2012).
2. Cruz, G., Atkinson, D., Henningsson, M., Botnar, R. M. and Prieto, C. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn. Reson. Med.77,1894–1908 (2017).
3. Bustin, A., Ginami, G., Cruz, G., Correia, T., Ismail, T. F., Rashid, I., Neji, R., Botnar, R. M. and Prieto, C. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn. Reson. Med.81,102–115 (2019).
4. Prieto, C., Doneva, M., Usman, M., Henningsson, M., Greil, G., Schaeffter, T. and Botnar, R. M. Highly efficient respiratory motion compensated free-breathing coronary mra using golden-step Cartesian acquisition. J. Magn. Reson. Imaging41,738–746 (2015).
5. Etienne, A., Botnar, R. M., Van Muiswinkel, A. M. C., Boesiger, P., Manning, W. J. and Stuber, M. ‘Soap-Bubble’ visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn. Reson. Med.(2002).
Figures