2138
Pulmonary artery dimensions from catheter angiography, multi-slice computed tomography, 3D-rotational angiography and PC MR Angiography1Biomedical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 2University of Wisconsin - Madison, Madison, WI, United States
Synopsis
In a swine congenital heart disease model we show strong agreement between PA dimensions from 3DRA, CA and MSCT. Non contrast-enhanced PC-MRA from PCVIPR showed good agreement with CA and MSCT for the imaging of non-stented proximal PAs.
Background
Accurate pulmonary artery (PA) imaging is necessary for management of patients with complex congenital heart disease (CHD). The ability of newer imaging modalities such as 3D rotational angiography (3DRA) or phase contrast magnetic resonance angiography (PC-MRA) to assess PA morphology has not been compared against established angiography techniques.Methods
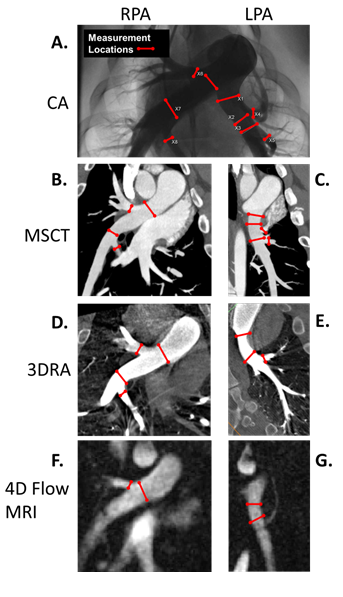
18 anesthetized 20-week old male swine (55 ± 9 Kg - 4 sham controls, 4 untreated proximal LPA stenosis and 10 stented proximal LPA) had CA, MSCT, 3DRA and PC-MRA on the same date. Measurements of PA morphology (including PA stenosis and PA stents) from 3DRA and PC-MRA are compared to 2D catheter angiography (CA) and multi-slice computed tomography (MSCT) in a swine CHD model. Contrast free 4D Flow MRI was performed with a three-dimensional radial undersampled isotropic projection reconstruction sequence (PC-VIPR) (1,2) on a 3.0T MRI scanner (Discovery MR750, GE Healthcare, Waukesha, WI). PA diameter measurements were performed independently by two investigators (RP – 1 year experience mentored by LL - 15 years CHD imaging experience) in the following locations: proximal LPA, LPA and RPA adjacent to two first order branch origins and two proximal RPA and LPA first order branches (Figure 1). Bland-Altman analysis is used for imaging modality comparisons.Results
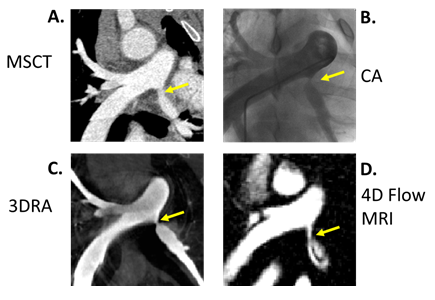
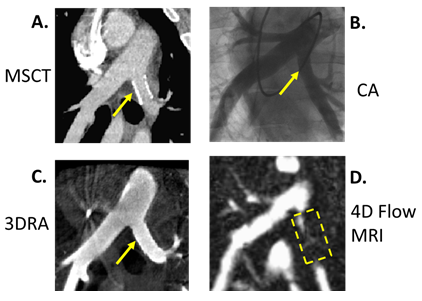
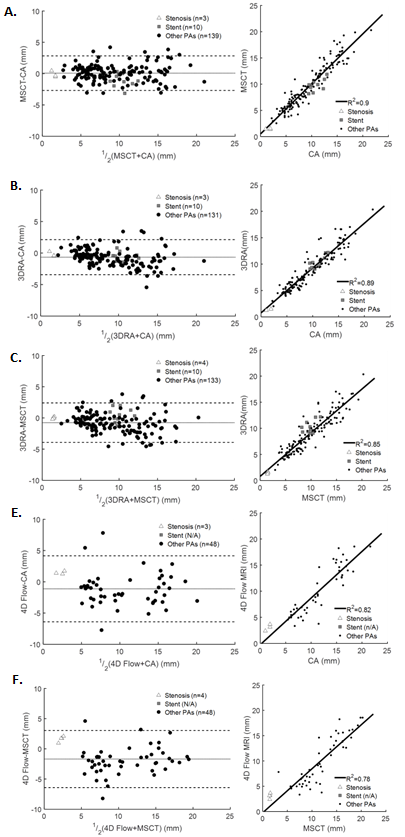
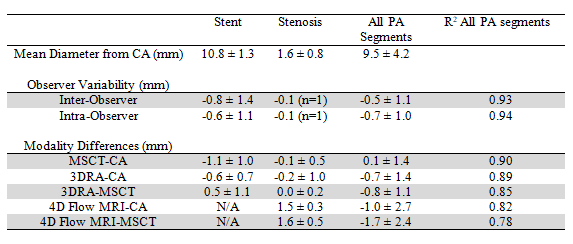
Representative healthy, stenotic and stented PA angiograms are shown in Figures 1-3. For all PA segments 3DRA had strong agreement with CA and MSCT (Table, Figure 4) although systematic underestimation by 3DRA was observed. Stents and the distal PA vessels could not be reliably visualized by PC-MRA so only 34% of measurement sites were identified. Stenosis diameters from PC-MRA were within one voxel (1.25mm) of CA and MSCT measurements and for other PA segments PC-MRA had good agreement with CA and MSCT. PA diameter agreement between CA and MSCT confirmed previously published data in CHD patients.Discussion
Strong agreement was seen between 3DRA, CA and MSCT, particularly in stenotic and stented regions. Non-contrast-enhanced PC-MRA was only able to image the proximal PA measurement sites and showed good agreement compared to CA and MSCT for these PA segments. Based on this information, 3DRA is a reliable method for measuring the size of the proximal and distal PAs and as a guide for PA interventions. Non-contrast-enhanced PC-MRA was only able to accurately measure the size of the proximal PAs.A summary of qualitative findings include the following: CA provided only a two dimensional view of the pulmonary vasculature while all other imaging modalities generated detailed multi-planar data sets that can be visualized from multiple angles. The ability of MSCT, 3DRA and PC-MRA to create multi-planar datasets is key for comprehensive assessment of the branching pulmonary arteries (3,4). 3DRA with IVC occlusion only opacified the PAs as contrast is intentionally localized to the PAs with IVC occlusion to better define PA anatomy while the entire vasculature (PAs, pulmonary veins, aorta) is visualized with CA in the levophase and with MSCT and 4D Flow MRI. PA stents caused localized artifact and as such the proximal LPA was not visible with 4D Flow MRI although the LPA distal to the stent was visible.
In addition to PC-MRA, other MRA techniques are in clinical use. Multiple sequences are typically used in a single cardiac MR exam for comprehensive assessment. The advantages and limitations of other MR techniques are discussed elsewhere (3). We do note that PC-MRAs from PCVIPR can be obtained without a contrast agent and also measures key functional information such as cardiac output, lung perfusion, pulmonary-systemic blood flow ratio (Qp:Qs) and can also estimate stenosis pressure drop. Contrast-enhanced MRA was not included in this study but is typically used in human clinical protocols. Given the uncertainty regarding gadolinium deposition we chose to investigate the PA imaging capabilities of a non-contrast-enhanced MRA technique.
Conclusion
Our findings show strong agreements between PA dimensions from 3DRA, CA and MSCT demonstrating feasibility of using 3DRA for diagnostic PA imaging in complex CHD. Non contrast-enhanced PC-MRA from PCVIPR showed good agreement with CA and MSCT for the imaging of non-stented proximal PAs.Acknowledgements
This investigation was supported by the Clinical and Translational Science Award (CTSA) program, through the NIH National Center for Advancing Translational Sciences (NCATS), grant UL1TR002373 (AR, LL and CF) and under the NIH Ruth L. Kirschstein National Research Service Award T32 HL 007936 from the National Heart Lung and Blood Institute to the University of Wisconsin-Madison Cardiovascular Research Center (RP). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.References
1. François CJ., Srinivasan S., Schiebler ML., et al. 4D cardiovascular magnetic resonance velocity mapping of alterations of right heart flow patterns and main pulmonary artery hemodynamics in tetralogy of Fallot. J Cardiovasc Magn Reson 2012;14:16. Doi: 10.1186/1532-429X-14-16.
2. Wieben O., Francois C., Reeder SB. Cardiac MRI of ischemic heart disease at 3 T: Potential and challenges. Eur J Radiol 2008;65(1):15–28. Doi: 10.1016/j.ejrad.2007.10.022.
3. Crean A. Congenital heart disease CARDIOVASCULAR MR AND CT IN CONGENITAL HEART DISEASE. Heart 2007;93:1637–47. Doi: 10.1136/hrt.2006.104729.
4. Choe YH., Ko JK., Lee HJ., Kang I-S., Park PW., Lee YT. MR Imaging on Non-visualized Pulmonary Arteries at Angiography in Patients with Congenital Heart Disease. J Korean Med Sci 1998;13:597–602. 5. Leschka S., Oechslin E., Husman L., et al. Pre-and Postoperative Evaluation of Con-genital Heart Disease in Children and Adults with 64-Section CT 1. Radiographics 2007;27(3):829–46. Doi: 10.1148/rg.273065713.
Figures