2134
Comparison of high-resolution magnetic resonance imaging and computed tomography for detection of distal vertebral artery calcification1The First Medical Center of PLA General Hospital, Beijing, China, 2Beijing Tiantan Hospital, Beijing, China, 3xinzhou@wipm.ac.cn, National Center for Magnetic Resonance in Wuhan, Wuhan Institute of Physics and Mathematics, Innovation Academy of Precision Measurement Science and Technology, Chinese Academy of Sciences-Wuhan National Laboratory for Optoelectronics, Beijing, China
Synopsis
In this study, we aim to perform a comparative analysis of high-resolution magnetic resonance imaging (HRMRI) and noncontrast computer tomography (NCCT) in detection of arterial calcifications in V3 horizontal and V4 segment of vertebral artery in patients with posterior circulation ischemic events. We observed that, HRMRI is as accurate as NCCT in the detection of V4 segment calcifications, while HRMRI are superior in detection of V3 horizontal segment calcifications than NCCT.
Purpose:
Artery calcification regularly develops during the process of atherosclerosis.1, 2 Intracranial artery calcification recently has been known as an independent risk factor of previous and future ischemic events.3 We aim to perform a comparative analysis between high-resolution magnetic resonance imaging (HRMRI) and noncontrast computed tomography (NCCT) in the detection of artery calcifications in V3 horizontal and V4 segment of the vertebral artery in patients with posterior circulation ischemic events.Methods:
Patients with symptomatic intracranial atherosclerosis who underwent both HRMRI and NCCT scans were included between September 2014 and January 2017. All HRMRI studies were performed by the same experienced radiology technologist 3T GE DISCOVERY MR 750 (GE Healthcare, Waukesha, WI) or 3T Siemens Trio MR scanner (Siemens Healthcare, Erlangen, Germany); 3D T1-weighted imaging, 3D T2-weighted imaging, proton attenuation weighted imaging, post-contrast enhancement 3D T1-weighted imaging for each patient. NCCT was performed on GE DISCOVERY 750 (GE Healthcare, Waukesha, WI), using a standard head scanning protocol with a field of view of 220 × 220 mm, 0.625 beam collimation, and 1.0 mm slice thickness. Calcifications of V3 horizontal and V4 segment were independently interpreted and compared between HRMRI and NCCT. Statistical analysis was performed using SPSS software (version 20.0, SPSS, Chicago, IL, USA). P values were 2-tailed, and results with P values less than 0.05 were considered statistically significant.Results:
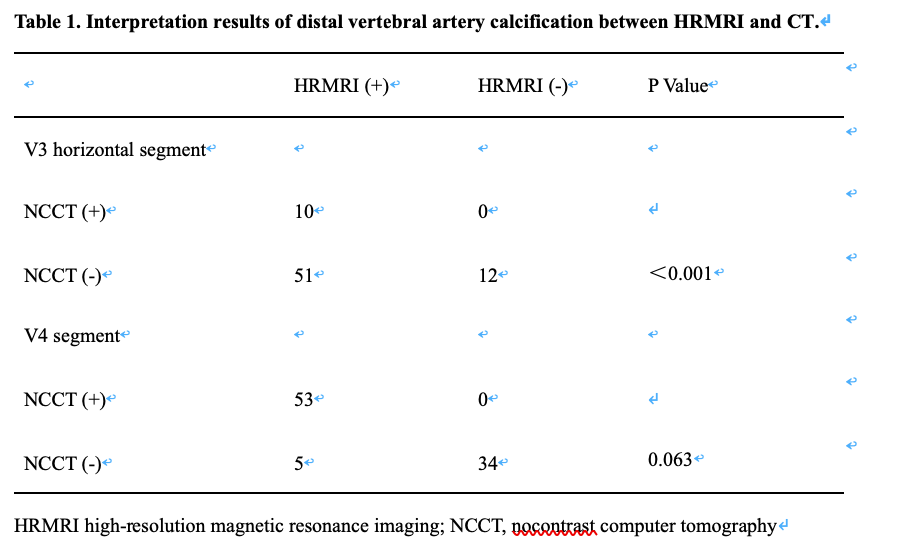
During the study period, 298 patients were enrolled consecutively from September 2014 to January 2017. Finally, 46 patients with eligibility were involved in this study. Of them, 44 were male, and the mean age was 57.1 years. Overall, 92 V4 segments (from all 46 patients) and 73 V3 horizontal segments (from 37 patients) were analyzed in this study. Calcification was detected on 58 (58/92, 63%) V4 segments in 35 patients (35/46, 76%) by HRMRI, in contrast to 53 (53/92, 57.6%) V4 segments in 34 patients (34/46, 73.9%) by NCCT. One typical patient with calcification detected on both NCCT and HRMRI was shown in Figure 1. Of note, four patients with five calcifications detected on HRMRI were not found on NCCT (Figure 2). Calcification was detected on 61 (61/73, 83.5%) V3 horizontal segments in 34 patients (34/37, 92%) by HRMRI, in contrast to 10 (10/73, 13.7%) V3 horizontal segments in 9 patients (9/37, 24.3%) by NCCT. One typical patient with calcification was found on HRMRI but not on CT was shown in Figure 3. The McNemar test revealed a significant difference between NCCT and HRMRI on V3 horizontal segment (P<0.05), but not on the V4 segment (P=0.063). The comparisons between NCCT and HRMRI performance in detection of calcification on V3 horizontal and V4 segment were presented in Table 1.Discussion and Conclusions:
In the comparative analysis between HRMRI and NCCT, we observed that HRMRI is as accurate as NCCT to detect V4 segment calcifications, while HRMRI is superior in detection of V3 horizontal segment calcifications compared to NCCT.As for detection of artery calcification, HRMRI has proved to be a promising approach to V4 and V3 segments in comparison to the NCCT from this study. This work has advanced the comparison between HRMRI and NCCT in patients with posterior circulation ischemic events. The HRMRI approach may be adapted to as an alternative clinical standard with extensive sample-size studies.Acknowledgements
No acknowledgement found.References
1.Bos D, Portegies ML, van der Lugt A, Bos MJ, Koudstaal PJ, Hofman A, Krestin GP, Franco OH, Vernooij MW, Ikram MA (2014) Intracranial carotid artery atherosclerosis and the risk of stroke in whites: The rotterdam study. JAMA neurology 71:405-411.https://doi.org/ 10.1001/jamaneurol.2013.6223.
2. Wu XH, Chen XY, Wang LJ, Wong KS (2016) Intracranial artery calcification and its clinical significance. Journal of clinical neurology (Seoul, Korea) 12:253-261. https://doi.org/ 10.3988/jcn.2016.12.3.253.
3.Chen XY, Lam WW, Ng HK, Fan YH, Wong KS (2007) Intracranial artery calcification: A newly identified risk factor of ischemic stroke. Journal of neuroimaging : official journal of the American Society of Neuroimaging 17:300-303.https://doi.org/ 10.1111/j.1552-6569.2007.00158.x
Figures
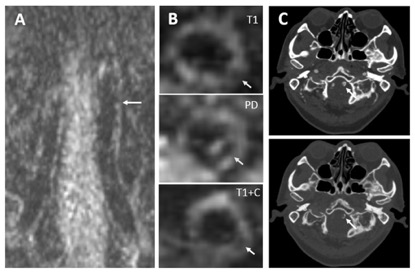

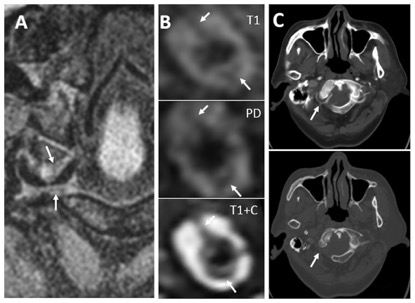
Figure 3. A 66-year-old male. Calcification was visualized on HRMRI but not on NCCT. Coronal HRMRI showed a strip hypointensity on right and superior aspects and left and inferior aspects of right V3 horizontal segment (A). From top to bottom, a strip hypointensity at 9 to 12 o’clock position and on 3 to 6 o’clock right V3 horizontal segment were showed on T1WI, PDWI and enhanced T1WI (arrows) (B). Enhanced CT (upper) showed the same location of V3 horizontal as that on HRMRI, and NCCT (lower) showed no calcification (C). Calcification was not found by NCCT.