2129
Evolution of Diffuse Wall Thickening of Petrous Internal Carotid Artery Peri-Revascularization: A MR Vessel Wall Imaging Follow-up Study
Xiaoyi Chen1, Huimin Xu2, Tao Wang3, Jin Zhang4, Huiyu Qiao5, Hualu Han5, and Xihai Zhao5
1Department of Radiology, Beijing Geriatric Hospital, Beijing, China, 2Department of Radiology, Peking University Third Hospital, Beijing, China, 3Department of Neurosurgery, Peking University Third Hospital, Beijing, China, 4Department of Radiology, Renji Hospital, Shanghai Jiaotong University, Shanghai, China, 5Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University School of Medicine, Beijing, China
1Department of Radiology, Beijing Geriatric Hospital, Beijing, China, 2Department of Radiology, Peking University Third Hospital, Beijing, China, 3Department of Neurosurgery, Peking University Third Hospital, Beijing, China, 4Department of Radiology, Renji Hospital, Shanghai Jiaotong University, Shanghai, China, 5Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University School of Medicine, Beijing, China
Synopsis
Carotid artery severe stenosis or occlusion will lead to ischemia within the vessel wall and diffuse wall thickening (DWT) in the downstream arterial segment. The revascularization surgery is an effective treatment for carotid artery stenosis. This study investigated the peri-revascularization change of DWT in petrous internal carotid artery (ICA) among carotid atherosclerotic patients using MR vessel wall imaging. We found that the DWT in ipsilateral petrous ICA recovered after revascularization treatment (1.68±0.68 mm vs. 1.39±0.47 mm, P =0.002) and it began to recover one month later after the revascularization.
Introduction
Previous studies reported that the phenomenon of diffuse wall thickening (DWT) in petrous internal carotid artery (ICA) was prevalent in carotid arteries with severe stenosis in proximal segment.1 Carotid artery severe stenosis or occlusion will lead to decreases in blood flow of downstream arterial segments and subsequently ischemia,2,3 showing DWT on magnetic resonance (MR) vessel wall images.1 The revascularization surgery is a safe and effective procedure to prevent stroke in patients with carotid steno-occlusive diseases. It can relieve the stenosis in proximal ICA, improve the blood flow perfusion and ischemia condition in the vessel wall.4 However, it is unknown that if the DWT in petrous ICA will recover after revascularization surgery for ICA with severe stenosis or occlusion in proximal segment. This study sought to investigate the peri-revascularization change of DWT in petrous ICA among carotid atherosclerotic patients using MR vessel wall imaging.Methods
Study sample: Patients with symptomatic severe atherosclerotic stenosis in ICA and referred to carotid endarterectomy or carotid artery stenting were recruited. The study protocol was approved by institutional review board and written consent form was obtained from each patient. MR imaging: The MR vessel wall imaging for carotid arteries was conducted before (<1 month) and after (<6 months) surgery on a 3.0T MR scanner (Achieva TX, Philips Medical Systems, The Netherlands) with an 8-channel carotid coil. The carotid MR imaging protocol and parameters are as follows: 3D time-of-flight (TOF): TR/TE 20/4.9 ms, flip angle 20°, field of view (FOV) 4×16×16 cm3, spatial resolution 1.0 mm3; 3D T1-VISTA: TR/TE 800/19 ms, flip angle 90°, FOV 20×18×4 cm3, spatial resolution 0.5 mm3; 3D MERGE: TR/TE 9.4/4.3 ms, flip angle 6°, FOV 4×16×16 cm3, spatial resolution 0.8 mm3. Data analysis: All images obtained before and after revascularization surgery were reviewed by two experienced radiologists blinded to imaging time point with consensus. The degree of stenosis of proximal ICA was measured on 3D TOF MRA images.5 The 3D T1-VISTA and MERGE images were used to measure the wall thickness of the petrous ICA on a MR workstation (Philips Extended MR WorkSpace 2.6.3.4, Best, The Netherlands) at the proximal, middle, and distal segments and the average value of these three segments was taken for statistical analysis. The time interval between surgery and follow-up MR scans was classified into the following categories: 0-30 days, 31-90 days, >90 days. DWT was identified as mean wall thickness >1.5mm.1 The DWT recovery was identified as mean wall thickness decreased by 0.5 mm after surgery. Statistical analysis: The prevalence of DWT at baseline and DWT recovery after revascularization surgery were calculated. The stenosis of proximal ICA and mean wall thickness of petrous ICA before and after surgery was compared by non-parametric Wilcoxon paired test.Results
In total, 26 arteries from 25 patients (mean age 64.8±8.6 years, 22 males) before and after revascularization surgery with acceptable image quality were included for final analysis. The mean time interval between baseline and follow-up MR scans was 94.3±67.5 days. Of the 26 carotid arteries at baseline, 14 (53.8%) had DWT in the petrous segment. Of the 14 arteries with DWT, 6 (42.9%) showed recovery. The distribution of DWT recovery in different categories of follow-up period is detailed in Figure 1. The non-parametric Wilcoxon paired test revealed that the stenosis degree of proximal ICA (83.8±10.4% vs. 8.5±17.5%, P <0.001) and the mean wall thickness of petrous ICA (1.68±0.68 mm vs. 1.39±0.47 mm, P =0.002) were significantly reduced after carotid revascularization surgery. Fig. 2 represents MR images of a carotid artery with significant stenosis in proximal segment and DWT in petrous segment before surgery and MR images after carotid endarterectomy at the same patient.Discussion and Conclusion
The diffuse wall thickening in ipsilateral petrous ICA will recover after revascularization treatment among patients with severe atherosclerotic stenosis in proximal ICA and it began to recover one month later after the revascularization surgery. The DWT was explained by vessel wall edema according the MR imaging performance.1,6 Hemodynamic studies have confirmed that severe stenosis can cause critical flow and wall mechanical conditions, which may activate a series of pathophysiological processes, including endothelial dysfunction and inflammation, and subsequently result in wall edema.7,8 The severe carotid stenosis can be restored by revascularization surgery, making the downstream arterial segment reperfusion and the DWT in petrous ICA recovery finally. However, the dynamic evolution of DWT in petrous ICA after revascularization in different time points is not clear and needs to be prospectively studied.Acknowledgements
NoneReferences
- Chen X, Zhao H, Chen Z, et al. Association between proximal internal carotid artery steno-occlusive disease and diffuse wall thickening in its petrous segment: a magnetic resonance vessel wall imaging study. Neuroradiology. 2017;59(5):485-490.
- Gibbs JM, Wise RJS, Leenders KL, et al. Evaluation of cerebral perfusion reserve in patients with carotid-artery occlusion. Lancet. 1984;1(8370):182-186.
- Powers WJ, Press GA, Grubb RL Jr, et al. The effect of hemodynamically significant carotid artery disease on the hemodynamic status of the cerebral circulation. Ann Intern Med. 1987;106(1):27-34.
- Abou-Zamzam AM Jr, Moneta GL, Landry GJ, et al. Carotid surgery following previous carotid endarterectomy is safe and effective. Vasc Endovascular Surg. 2002;36(4):263-270.
- North American Symptomatic Carotid Endarterectomy Trial Collaborators, Barnett HJM, Taylor DW, et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325(7):445-453.
- Pedersen SF, Kim WY, Paaske WP, et al. Determination of acute vascular injury and edema in porcine carotid arteries by T2 weighted cardiovascular magnetic resonance. Int J Cardiovasc Imaging. 2012;28(7):1717-1724.
- Tang D, Yang C, Kobayashi S, et al. Steady flow and wall compression in stenotic arteries: a three-dimensional thick-wall model with fluid-wall interactions. J Biomech Eng. 2001; 123(6):548-557.
- Simard JM, Kent TA, Chen M, et al. Brain oedema in focal ischaemia: molecular pathophysiology and theoretical implications. Lancet Neurol. 2007;6(3):258-268.
Figures
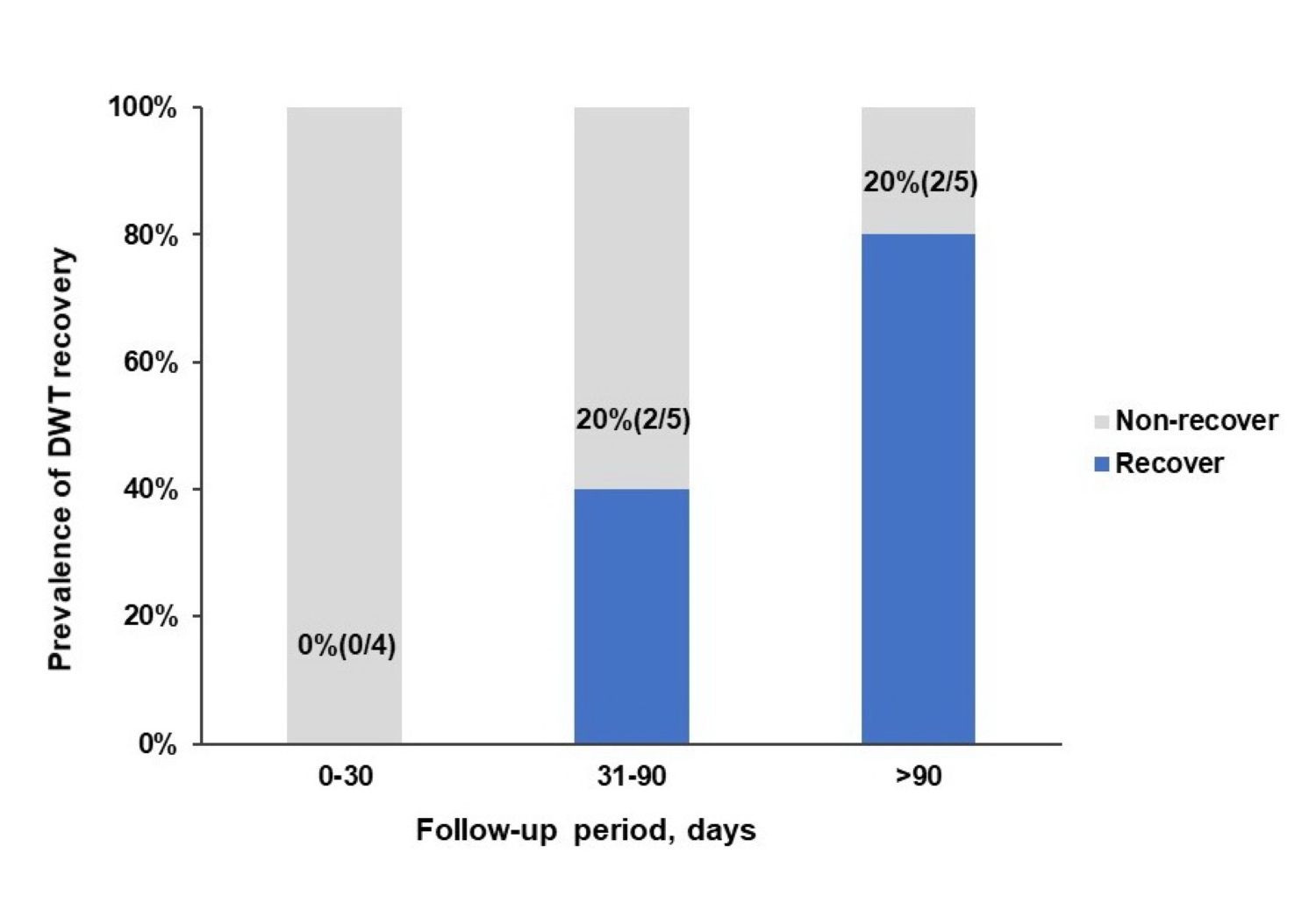
Figure 1. The prevalence of DWT in
petrous ICA recovery among different follow-up periods.
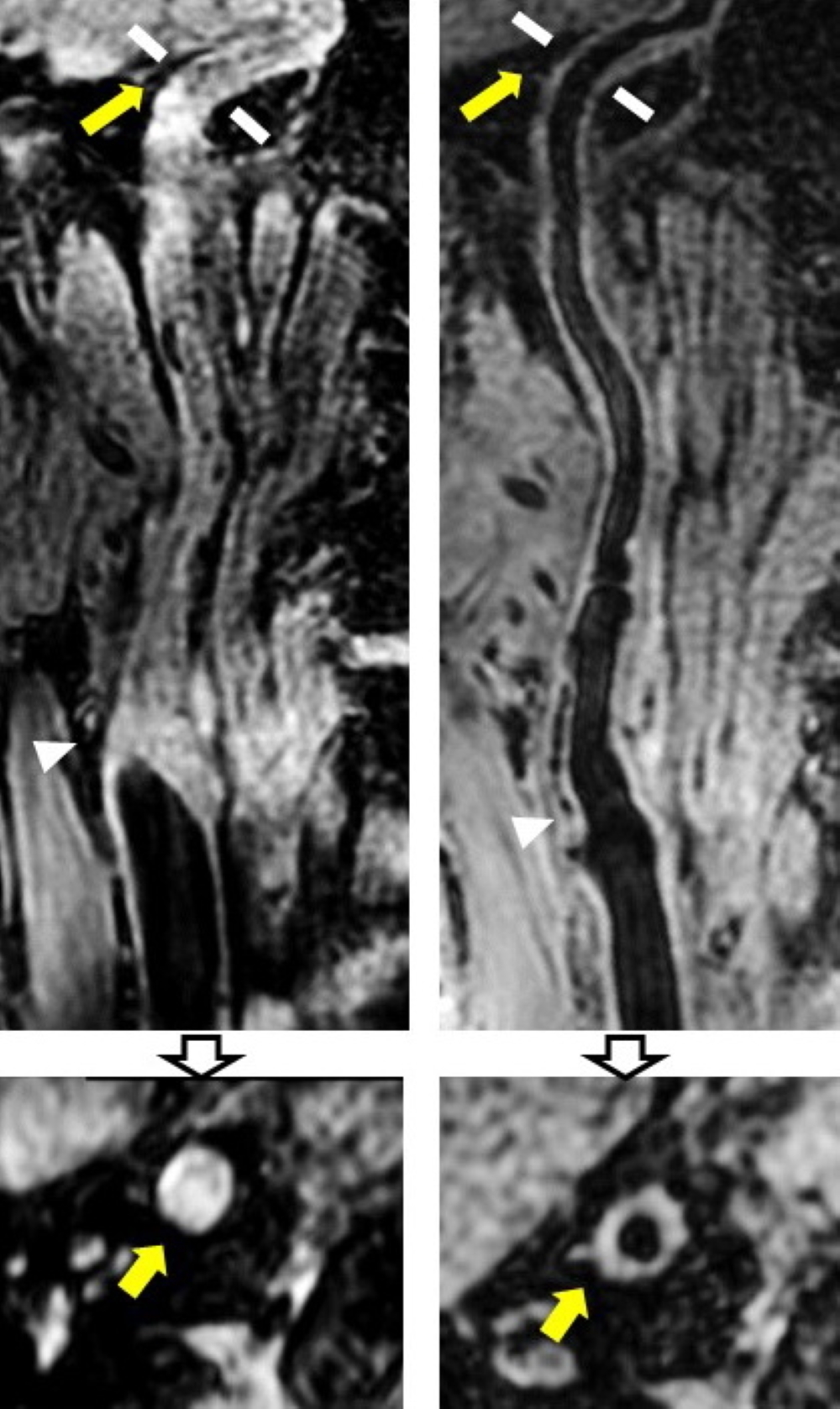
Figure 2. The curved and axial reconstructed MR images from a 60
years old male patient with carotid atherosclerotic occlusion peri-CEA. The
left column represents the carotid artery with occlusion in proximal ICA (white
arrow head) and severe DWT in petrous ICA (yellow arrow) before CEA; the right
column represents the MR images 68 days later after CEA, we found that the
stenosis was restored (white arrow head) and the DWT in petrous ICA recovered
(yellow arrow) completely (mean wall thickness =1.48mm).