2118
EVAR Does Not Affect Mean Blood Flow Volume and Flow Profile of the Visceral Arteries.1Department of Fundamental Development for Advanced Low Invasive Diagnostic Imaging, Nagoya University Graduate School of Medicine, Nagoya, Japan, 2Department of Radiology, Nagoya University, Nagoya, Japan, 3Department of Radiological Technology, Nagoya University Hospital, Nagoya, Japan, 4Department of Radiology, Hamamatsu University School of Medicine, Hamamatsu, Japan, 5Applied Science Laboratory Asia Pacific, GE Healthcare Japan, Hino, Japan, 6Department of Radiology, Stanford University School of Medicine, Palo Alto, CA, United States
Synopsis
We aimed to assess the effect of EVAR treatment to the blood flow profile of visceral arteries using 4D-Flow MRI. 10 patients with AAA underwent 4D-Flow pre- and one month post-EVAR. The flow volume at the sections in suprarenal and infrarenal abdominal aorta, the celiac artery, the superior mesenteric artery and the renal arteries were measured. No significant change in blood flow volume was observed within visceral arteries after EVAR despite the placement of stiff stent in the deformed blood pathway.
Introduction
Endovascular aortic repair (EVAR) is widely performed to prevent abdominal aortic aneurysms (AAA) from rupture. Besides the primal aim, there is a controversy if EVAR affect the flow rate of the abdominal visceral arteries. Repaired blood pathway may relieve blood flow energy loss in the AAA and consequently improve the efficiency of blood delivery to the peripherals (1). On the other hand, stiff metallic stent for EVAR may also restrict overall blood flow to the aorta due to its low compliance of the stent(2). 3D cine-PC MRI (4D-Flow) allows acquisitions of blood flow vector data of whole abdominal aorta in 3 dimensional fashion with time resolution of 20 phases per cardiac cycle. The metal artifact due to the abdominal stent does not hinder the measurement of the blood flow dynamics in 4D-Flow(3). In this study we aimed to assess the effect of EVAR treatment to the blood flow profile of the abdominal aorta as well as abdominal visceral arteries, by comparing the time resolved blood flow volume before and after EVAR.Methods
After informed consent, 10 patients (59 to 82 years old, all male) with infrarenal abdominal aortic fusiform aneurysm were eligible for the study. All patients were treated by EVAR, and underwent 4D-Flow within the period of one month before and after EVAR.All the MR studies were conducted on 3.0T MR imagers with phased array coil (Discovery 750 and Discovery 750W, GE Healthcare, Waukesha, WI). First, the contrast enhanced 3D MR Angiography (Gd-3DMRA) was performed for the segmentation of the aortic boundary. Then, 2D cine PC with velocity encoding (VENC) of 200 cm/s was performed placing a transverse section within suprarenal abdominal aorta to estimate the maximum flow of the aorta. The VENC of 4D-Flow was set to the max flow velocity of 2DcinePC + 20cm/sec. Finally, ECG gated, respiratory compensated gradient-echo-based coronal 4D-Flow covering from suprarenal abdominal aorta to common iliac arteries was performed. The parameters set for 4D-Flow data acquisition are as follows; TR/TE/FA/NEX of 4.5-5.5/2.0-3.0/15/1, FOV of 32 cm, Matrix of 224x224, 2 mm thickness, 60 partitions, 20 /cardiac cycle.
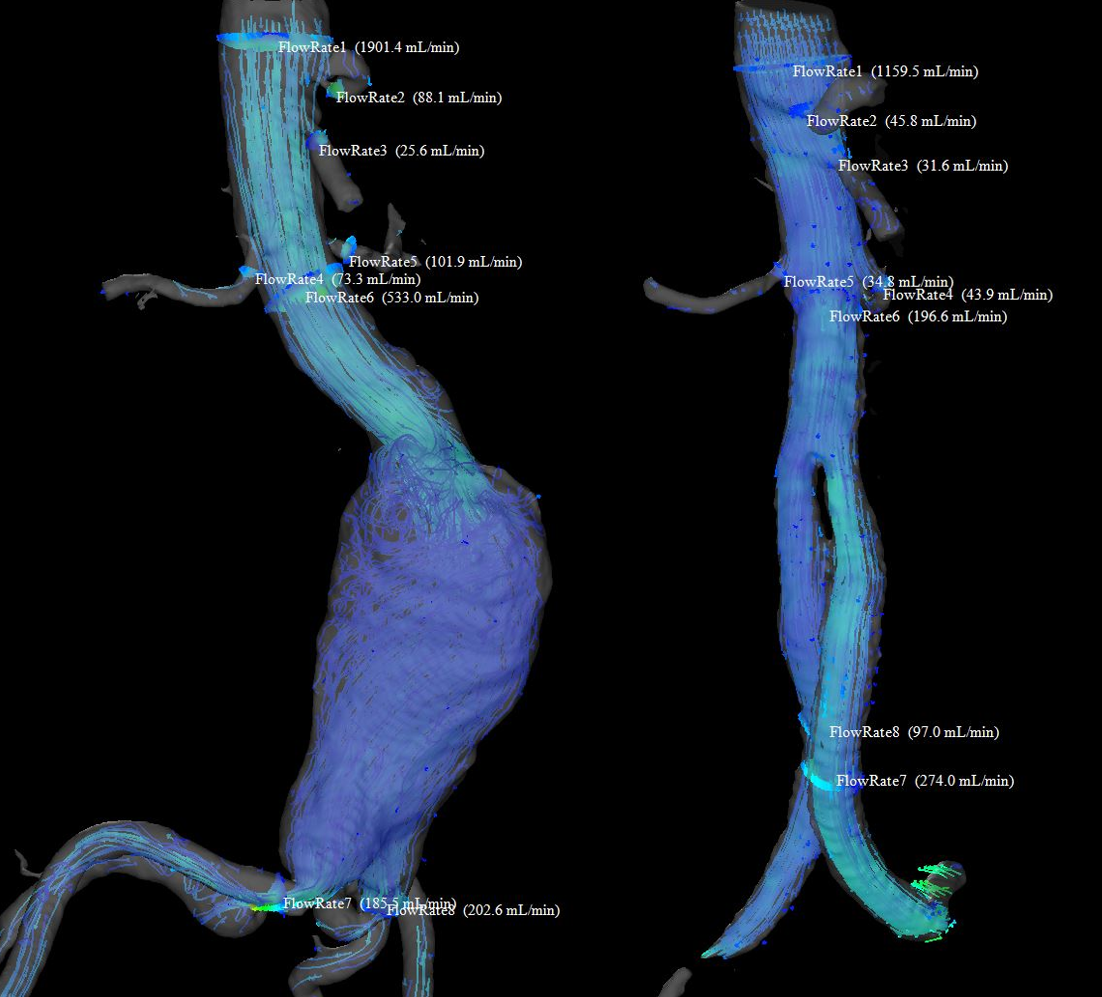
The acquired 4D-Flow data was postprocessed using a flow analysis software (iTFlow, CardioFlowDesign, Japan). The blood flow vector data derived from 4D-Flow and the geometric boundary of the aorta determined by Gd-3DMRA were interpolated using the software. The flow volume at the sections in the suprarenal abdominal aorta (SupraRA), infrarenal abdominal aorta (InfraRA), celiac artery (CA), superior mesenteric artery (SMA) and renal arteries (RA) were measured (figure 1). Each dataset consisted of flow volume data of 20 phases per cardiac cycle. The flow volume of each cardiac phase and time-averaged flow volume were statistically compared at each section using non-parametric test (Wilcoxon’s signed-rank test, p≤0.05 were considered to be significant).
Results
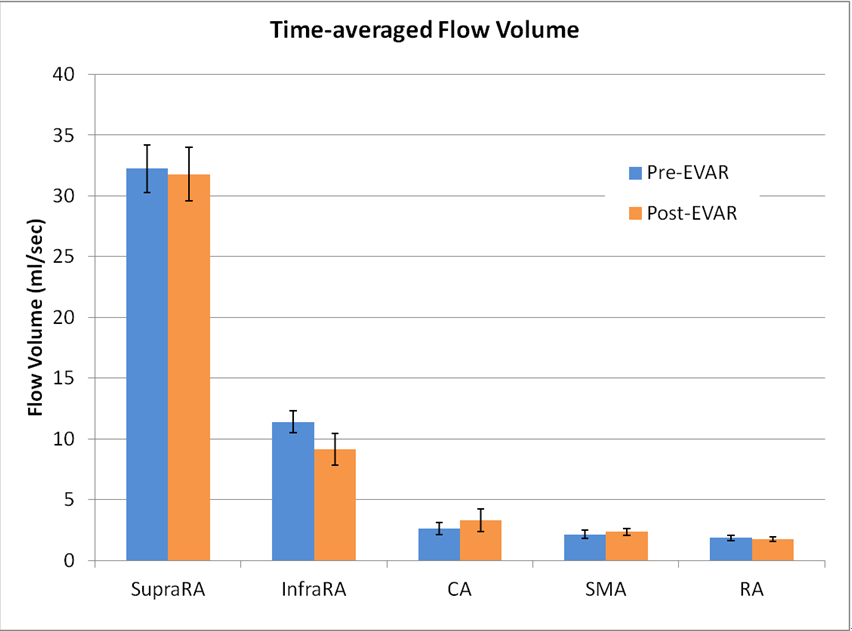
10 suprarenal and infrarenal aortas, CAs and SMAs were measured in ten patients. 21 RA were measured since one patient had two right renal arteries. The time-averaged flow volume of the sections in aorta and visceral arteries showed no significant change between pre- and post-EVAR (figure 2). No significant change of flow volume was observed within suprarenal aorta, CA, SMA and RA throughout all cardiac phases (figure 3). The only significant change of flow volume observed after EVAR was the decrease at maximum systolic phase in infrarenal aorta (phase4; p=0.0371, phase5; p=0.010).Discussion
EVAR may repair deformed blood pathways, which may be contributing to improved blood flow delivery to the peripherals. On the other hand, stiff stent placement may also suppress compliance of the flow path and increase the impedance of blood flow. The modification of the blood flow pathway may alter the blood flow profile of visceral arteries. We hypothesized that the efficiency of blood flow delivery to the visceral arteries would improve as the retrograde reflex flow at early diastole increases (4). However, our result showed no significant change of blood flow volume in the visceral arteries after all. This is physiologically reasonable since the demand for arterial blood in peripherals should not change between pre- and post-EVAR condition. Besides the visceral arteries, significant suppression of systolic blood flow of infrarenal aorta was observed. This was probably due to the stiff stent with high impedance.Conclusion
Despite the modification of the blood pathway in infrarenal aortic aneurysm by stiff metallic stent, 4D-Flow measurement revealed no significant change of the mean blood flow as well as the blood flow volume profile in the visceral arteries after EVAR. 4D-Flow might be useful for evaluation of the blood flow dynamics of aorta and visceral arteries in pre- and post-EVAR condition.Acknowledgements
No acknowledgement found.References
(1) Burris, N. S. and Hope, M. D. “4D flow MRI applications for aortic disease.” Magn Reson Imaging Clin N Am, 2015. 23(1): 15-23.
(2) Takeda, Y. et al. “Endovascular Aortic Repair Increases Vascular Stiffness and Alters Cardiac Structure and Function.” Circ J, 2014. 78(2): 322–328
(3) Sakata, M., et al. “Hemodynamic Analysis of Endoleaks After Endovascular Abdominal Aortic Aneurysm Repair by Using 4-Dimensional Flow-Sensitive Magnetic Resonance Imaging.” Circ J, 2016. 80(8): 1715-25.
(4) Bogren, HG. et al. “Blood flow measurements in the aorta and major arteries with MR velocity mapping.” JMRI, 1994. 4(2): 119-30.
Figures
The flow volume of pre- and post-EVAR at the sections in suprarenal aorta (SupraRA), infrarenal aorta (InfraRA), celiac artery (CA), superior mesenteric artery (SMA) and renal arteries (RA) were measured.