2110
Myocardial Structural and Velocity Analysis in Patients with Arrhythmias Post-Heart Transplantation1Radiology, Northwestern University, Chicago, IL, United States, 2Cardiology, Northwestern University, Chicago, IL, United States, 3Biomedical Engineering, Northwestern University, Evanston, IL, United States
Synopsis
Cardiac magnetic resonance including tissue phase mapping was performed in a cohort of heart transplanted (HTx) patients developing atrial arrhythmias or atrio-ventricular blocks: T1-T2-ECV values and 3-directional myocardial velocities were calculated and compared to the same parameters acquired in HTx patients with normal sinus rhythm during the follow up. Alterations in myocardial structural properties (increased T2) and cardiac dynamics were evidenced in cardiac grafts showing hyperkinetic arrhythmias or atrio-ventricular blocks.
Introduction
Hyperkinetic atrial arrhythmias (AA) are frequently reported after heart transplantation (HTx). Denervation, sinus node ischemia or injury, presence of suture lines, and pericardial inflammation are common underlying mechanisms. Our aim was to study myocardial tissue characteristics and myocardial velocities using cardiac magnetic resonance (CMR) T1 and T2 mapping, and Tissue phase mapping (TPM) respectively, in HTx patients with documented AA and atrioventricular blocks (AVB).Methods
One hundred fifteen patients (49F) were prospectively recruited for CMR follow up after HTx. A total of 211 scans (1-4 scans per patient) were performed. Demographics are reported in Table 1. ECG during follow up was reviewed and patients were included in the AA group if atrial fibrillation, supraventricular tachycardia, atrial flutter, or atrial tachycardia were present in the ECG. Both permanent and paroxysmal AA and AVB were considered for analysis. AA and AVB were classified as permanent if present on ECG at scan time and throughout the entire follow up, or classified as paroxysmal if inconsistently present during follow up. Scan protocol included 2D cine SSFP, T2 mapping and pre- and post-contrast T1 mapping for ECV calculation and TPM for velocity analysis. T2 and pre- and post-contrast T1 maps were segmented from 3 slice short axis views (base, mid, apex) to obtain native T1, post-contrast T1, calculated ECV and T2 values, using a dedicated software (cvi42, Circle, Calgary, Canada). Three directional velocities were acquired using TPM sequence, in 3 slice short axis views as well (base, mid apex). TPM images were analyzed with a dedicated tool (Mathworks, Natick, MA, USA) and 3-directional myocardial velocities (longitudinal, radial, circumferential) calculated. Cardiac twist was subsequently calculated as the difference between circumferential velocity time courses from base and apex. Cross correlation coefficient (CC), an index of interventricular synchrony, was calculated using slice averaged ventricular velocity time courses for each velocity component by combining velocity data for all 3 slices (CC=1: complete synchronism LV-RV; reduced CC=increased dyssynchrony). Acquired parameters in patients with hyperkinetic AA and-or AVB were compared with parameters acquired in HTx patients showing permanent sinus rhythm (SR).Results
Structural (T1,T2, ECV) and velocity values are reported in table 2 (mean±SD), comparisons in Table 3. Compared to HTx patients in permanent SR, T2 values were significantly increased in patients developing AA and biventricular diastolic velocities were reduced in the radial direction. Increased interventricular dyssynchrony in the longitudinal direction was also present in patients with AA. When patients with AVB were grouped with AA for comparison, significant reduction in systolic RV twist and further significant reduction in interventricular synchrony in longitudinal and radial direction were evidenced, compared to patients in SR.Conclusion
HTx patients with AA or AVB show myocardial structural and dynamics alterations of the cardiac graft, when compared to HTx patients in permanent sinus rhythm. CMR-TPM can be a useful tool for post-HTx monitoring in patients developing hyperkinetic or hypokinetic arrhythmias.Acknowledgements
No acknowledgement found.References
No reference found.Figures
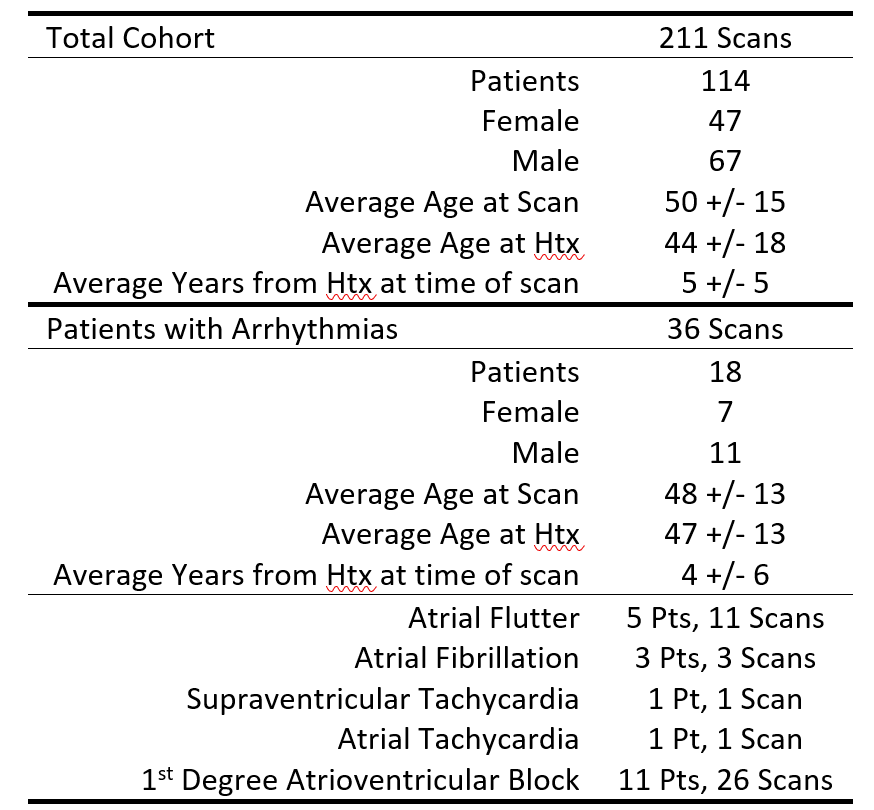
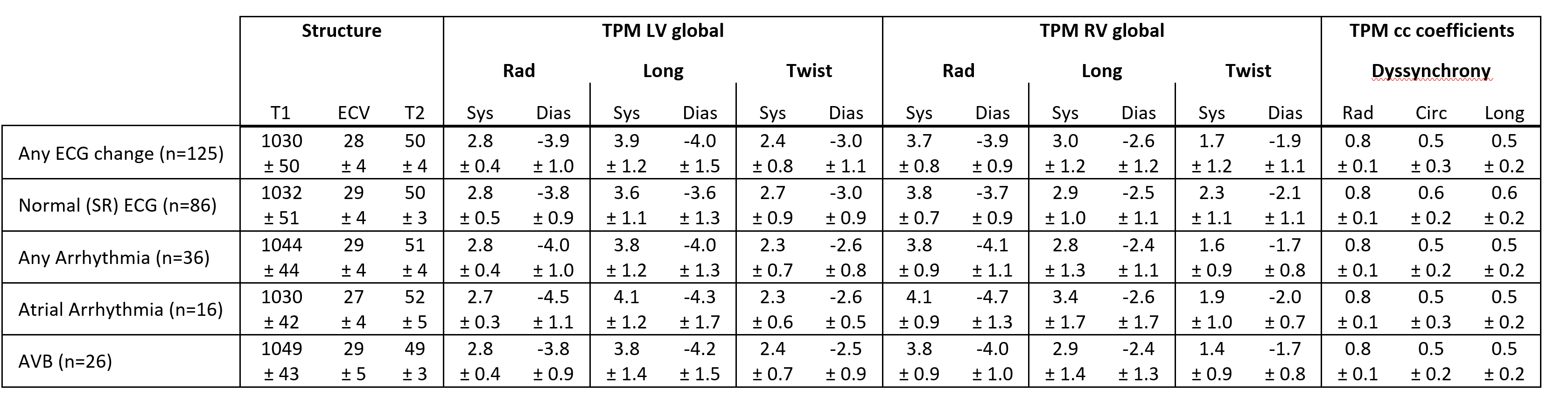
Table 2. Global structural (T1, T2, ECV) and velocity values are reported for patients with and without arrhythmias.
TPM = Tissue Phase Mapping, LV = Left Ventricle, RV = Right ventricle, cc = correlation coefficient, AA = Atrial Arrhythmia, SR=sinus rhythm AVB = Atrioventricular Block, Sys = systole, Dias = diastole, Rad = Radial, Circ = circumferential, Long = longitudinal. n indicates the number of scans

Table 3. Comparing structure and velocity values between patients with and without Arrhythmias.
This table demonstrates p values with P<0.05 indicating statistical significance. TPM = Tissue Phase Mapping, LV = Left Ventricle, RV = Right ventricle, cc = correlation coefficient, AA = Atrial Arrhythmia, AVB = Atrioventricular Block, SR=sinus rhythm, Sys = systole, Dias = diastole, Rad = Radial, Circ = circumferential, Long = longitudinal