2107
The impact of different Middle Cerebral Artery Stenosis Severity on Blood Flow Lateralization1Tsinghua University, Beijing, China, 2Beijing Tsinghua Changgung Hospital, Beijing, China
Synopsis
Middle cerebral artery stenosis induces flow lateralization. However, the impact of stenosis degree on flow lateralization is not fully understood. This study investigated the impact of MCA stenosis severity on MCA blood flow lateralization using 4D flow MRI. Twenty-seven patients with symptomatic MCA stenosis were included. Absolute flow rates of MCA on stenosis and contralateral sides were obtained. Paired samples t-test was used to compare the flows on both sides. We found a significant difference between the flows in the severe stenosis group, while there was no significant difference in non-severe group.
Introduction
Intracranial atherosclerotic disease (ICAD) is one of the most common causes of ischemic stroke worldwide1. Among those high risk factors related with recurrent stroke, hemodynamic changes may be an important one in patients with ICAD. Previous studies have shown that patients with unilateral symptomatic MCA stenosis (≥50%) may have a significant lower flow asymmetry index (AI-F) compared with healthy volunteers2, indicating blood flow lateralization. However, blood flow lateralization in patients with different stenosis severity is not fully understood. Furthermore, 4D flow MRI offers assessment of quantitative value of absolute blood flow rates in MCA3. The goal of this study was to investigate the impact of stenosis severity on MCA flow lateralization.Methods
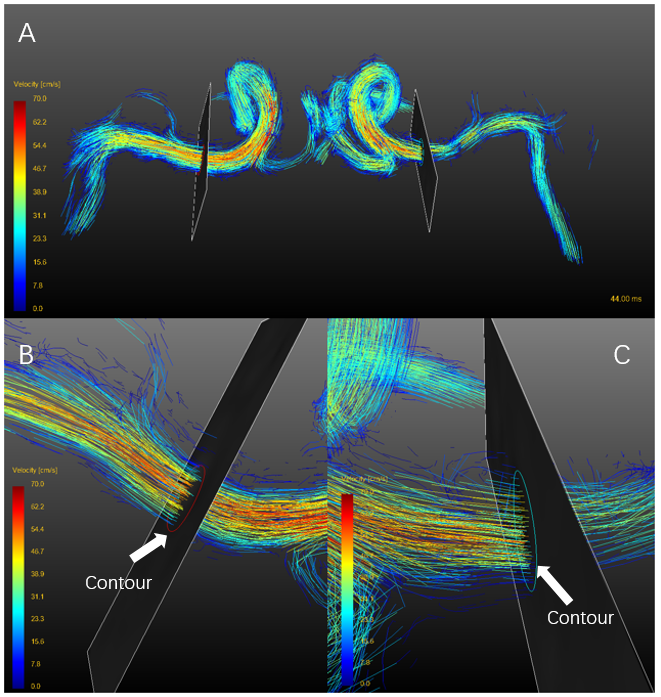
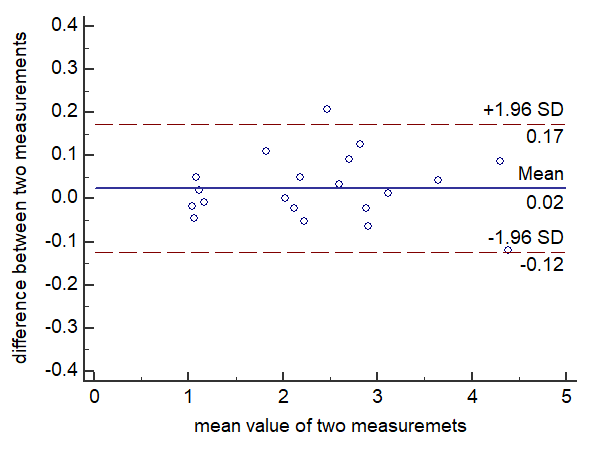
After excluding those with severe internal carotid artery (ICA) and anterior cerebral artery (ACA) stenosis, a total of 27 patients with unilateral symptomatic MCA stenosis were included in the retrospective study. They were divided into severe stenosis group (≥70%, n=15) and non-severe stenosis group (30%-70%, n=12). All participants underwent 4D-flow MRI after 3D TOF MRA in a 3.0T magnetic resonance scanner (GE discovery750, GE Medical Systems). Velocity encoding of 4D-flow MRI was set to 150 cm/s in all directions. Spatial resolution=1 x 1 x 1-2 mm3, temporal resolution=30-57 ms. GTFlow, version 3.2.5 (GyroTools, Zurich, Switzerland) was used to perform all the preprocessing, visualization, and quantification of 4D-flow data.When quantifying blood flow, contours were drawn manually in cut-planes which were perpendicular to MCA-M1 section. And cut-planes on both sides were created bilaterally symmetrical, as shown in figure 1. Velocities of flowing blood that passes through contours were measured. Absolute value of average blood flow rate (Flowavg, ml/s) defined by the mean flow value passing through contours in one cardiac cycle, was measured in GTFlow.4 Intra-observer reproducibility was assessed for Flowavg measurements using Bland–Altman test.
MCA stenosis severity was graded on the basis of clinically available 3D TOF MRA,according to WASID (Warfarin versus Aspirin for Symptomatic Intracranial Disease trial) by experienced radiologist.5 Paired samples t-test was used to compare Flowavg between stenosis side and contralateral side in subgroups. Statistical analysis was conducted by MedCalc, version 15.2.2 (MedCalc Software, Mariakerke, Belgium). The level of statistical significance was set at p< 0.05.
Results
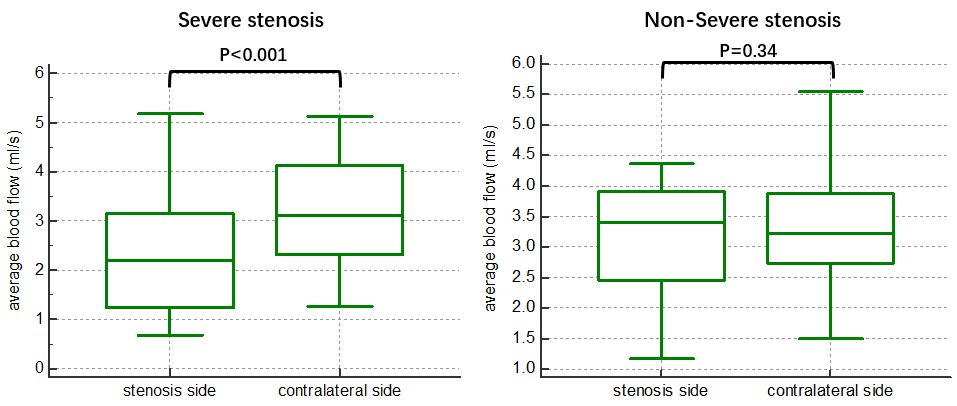
The Bland–Altman plot is depicted in figure 2, indicating good reproducibility. The difference between Flowavg of stenosis side and that of contralateral side is significant in severe stenosis subgroup (2.39±1.29 vs 3.22±1.17 ml/s, p<0.001). But in non-severe stenosis subgroup, the difference is not significant (3.10±1.10 vs 3.33±1.04, p=0.34). The results are shown in figure 3.Discussion
In summary, 4D-flow MRI provides a more comprehensive depiction of flow fields in MCA. We found that MCA Flowavg on the ipsilateral side to MCA stenosis was significantly lower than that of the contralateral side in the severe stenosis subgroup, which is in agreement with the previous findings2,6. And this may be because only severe stenosis is likely to affect blood flow. For few patients in the non-severe stenosis group, Flowavg of the stenosis side is much lower than the contralateral side. And the mismatch between stenosis degree and flow may be interpreted by further research on infarction and perfusion.Conclusion
This 4D flow MRI study shows that blood flow lateralization is related with stenosis severity. As expected, flow lateralization is significant in severe stenosis subgroup. But significant lateralization did not occur in non-stenosis subgroup. Future work can focus on investigating the potential mechanism of blood flow compensation to address the difference. Researches on the relation of different stenosis severity with hemodynamic changes in the entire cerebral arterial tree are important. And impacts of various factors, such as anatomical variations and collateral flow, on flow lateralization need to be investigated in a much larger cohort.Acknowledgements
References
1. Arenillas JF. Intracranial atherosclerosis: current concepts. Stroke 2011;42(1 Suppl):S20-23.
2. Wu C, Schnell S, Vakil P, et al. In Vivo Assessment of the Impact of Regional Intracranial Atherosclerotic Lesions on Brain Arterial 3D Hemodynamics. AJNR Am J Neuroradiol 2017;38(3):515-522.
3. Markl M, Frydrychowicz A, Kozerke S, Hope M, Wieben O. 4D flow MRI. J Magn Reson Imaging 2012;36(5):1015-1036.
4. Li Y, Chen H, He L, et al. Hemodynamic assessments of venous pulsatile tinnitus using 4D-flow MRI. Neurology 2018;91(6):e586-e593.
5. Chimowitz MI KJ, Strong J, et al. The Warfarin-Aspirin Symptomatic Intracranial Disease Study. Neurology 1995;45:1488–1493.
6. Zarrinkoob L, Wahlin A, Ambarki K, Birgander R, Eklund A, Malm J. Blood Flow Lateralization and Collateral Compensatory Mechanisms in Patients With Carotid Artery Stenosis. Stroke 2019;50(5):1081-1088.
Figures