2102
Myocardial Late Gadolinium Enhancement: Accuracy of Auto TI Inversion-Recovery Imaging vs Magnitude and Phase-Sensitivity IR images1Radiology, Beijing Anzhen Hospital, Captial Medical University, Beijing, China, 2Beijing Anzhen Hospital, Capital Medical University, Beijing, China, 3Philips Healthcare, Guangzhou, China, 4Beijing Anzhen Hospital,Capital Medical University, Beijing, China, 5Beijing Anzhen Hospital, Beijing, China, 6Philips Healthcare, Beijing, China
Synopsis
Recently, we proposed a novel LGE approach that could help radiologists/technicians automatically specify TI values .We propose a PSIR-specific TI optimization that could help automatically nulls TI while maintaining the scar-to-myocardium contrast. As a TFE preparation pulse is user defined on scanner, clinical application is readily available on current MR systems without the need for extensive optimizations, software modifications, and/or additional training.
Synopsis
Recently, we proposed a novel LGE approach that could help radiologists/technicians automatically specify TI values .We propose a PSIR-specific TI optimization that could help automatically nulls TI while maintaining the scar-to-myocardium contrast. As a TFE preparation pulse is user defined on scanner, clinical application is readily available on current MR systems without the need for extensive optimizations, software modifications, and/or additional training.abstract
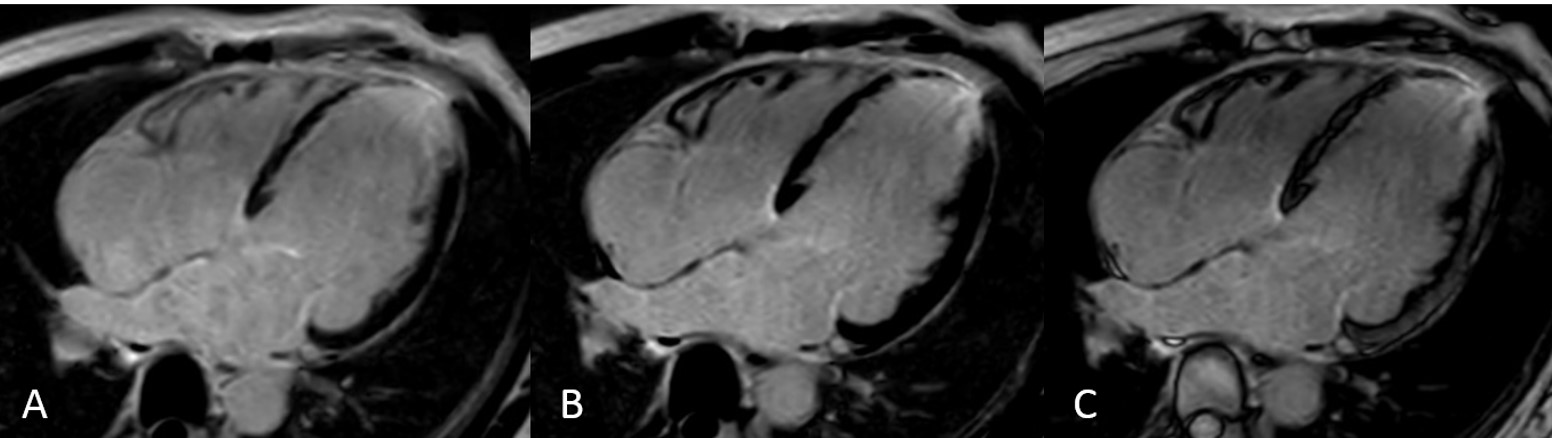
Introduction: For myocardial late gadolinium enhancement (LGE), magnitude inversion-recovery (MagIR) and phase-sensitive IR imaging (PSIR) as two major techniques have been introduced in the clinic [1, 2]. Prior to acquisition of LGE images, it is necessary to acquire a Look-Locker scan to determine the optimum inversion delay for nulling of a chosen tissue (usually viable myocardium, or for PSIR LGE the user may alternatively null blood to achieve black viable myocardium). This Look-Locker scan needs to be similar to the actual LGE scan; there is a single beat version for conventional LGE with higher heart rates, and a dual beat version for PSIR LGE and for conventional LGE with slower heart rates. This is now possible with the new parameters Calc TI to null a T1 and T1 to be nulled (ms) when the TFE prepulse delay is set to user defined. Currently, a novel IR technique, an auto TI-IR that is free from the TI set has been developed. This study is to compare the image quality and precision of the quantification in myocardial LGE using an auto TI-IR approach with that of MagIR and PSIR techniques Methods: From September to October 2019, 15 patients (10 men; mean age, 51 years ± 9) with myocardial infarction underwent cardiac MR were prospectively enrolled in this study. MagIR and PSIR images were acquired after contrast injection 10 minutes. A following auto TI-IR sequence was performed on Philips Ingenia CX3.0T MR scanner (Best, Netherlands). Images were assessed by two experience radiologists. Imaging quality (IQ) and quantitation of LGE areas between the three techniques were analyzed with the ANOVA statistics. IQ was scored in 4-point scales (0= no diagnosis, 1= fair; 2=good; 3=excellent). Quantitation of LGE included area of LGE and LGE fraction. LGE was quantified using a five standard deviation (5SD) (CVI, AB, Canada). Interreader agreement for the detection and quantification of LGE was analyzed with κ and Bland-Altman statistics, respectively. Results: The auto TI-IR sequence was successfully acquired in all patients. The IQ of auto TI-IR was better than that of MagIR imaging (image score 2.5 vs 2.0, p<0.05), no difference compared with PSIR imaging. The area of LGE measured with auto TI-IR technique showed excellent agreement with that of PSIR and MagIR techniques. Interreader agreement was excellent for the detection (κ > 0.88) and quantification (bias range 2.4, P > 0.05) of LGE in auto IR technique. Auto TI-IR MagIR PSIR P value IQ 2.5 2.0* 2.4 >0.05 LGE Area 3.71 cm2 ± 0.58 3.54 cm2± 0.62 3.24 cm2 ± 1.12 >0.05 LGE fraction 18.23% ± 8.25 17.14%± 7.63 14.28% ± 8.22 >0.05 *IQ Auto TI-IR 2.5 vs. Mag IR 2.0, p<0.05. Discussion Our initial results demonstrate that IQ and quantitative LGE with the auto TI-IR technique are comparable to that with MagIR and PSIR techniques. This may allow for more consistent image quality by omitting technologist input in the acquisition of traditional LGE IR sequences and may reduce operator dependence of this application by free TI set. Auto TI-IR technique There is a significant advantage of auto TI-IR technique. Such technique does not require an additional scan because it is already implanted in the IR LGE protocol. In our results, the IQ of the auto TI-IR approach is better than that of MagIR (image score 2.5 vs 2.0, p <0.05). Although there is no statistical difference in quantitation of LGE, the auto TI-IR approach shows more accuracy than that of MagIR (3.71 cm2 ± 0.58 vs 3.24 cm2 ± 1.12 in LGE area, 18.23% ± 8.25 vs 14.28% ± 8.22 in LGE fraction). There is no difference between auto TI-IR and PSIR approach in both IQ and quantification of LGE (image score 2.5 vs 2.4; 3.71 cm2 ± 0.58 vs 3.54 cm2± 0.62 in LGE area, 18.23% ± 8.25 vs 17.14%± 7.63 in LGE fraction). It demonstrates that an auto TI-IR approach would eliminate the need of a TI scout view before LGE imaging and readjusting the TI during the LGE acquisition. Conclusion: The IQ of myocardial LGE using auto TI-IR approach in myocardial infarction patients is better than that of MagIR technique, similar to that of PSIR technique, however, no difference in quantification. The use of auto TI-IR protocol may reduce operator dependence in myocardial LGE.main finding
Our initial results demonstrate that IQ and quantitative LGE with the auto TI-IR technique are comparable to that with MagIR and PSIR techniques.Acknowledgements
No acknowledgement found.References
1. Elgeti T, Abdel-Aty H, Wagner M, Busjahn A, Schulz-Menger J, Kivelitz D, Dietz R, Hamm B: Assessment of late gadolinium enhancement in nonischemic cardiomyopathy: comparison of a fast Phase-Sensitive Inversion Recovery Sequence (PSIR) and a conventional segmented 2D gradient echo recall (GRE) sequence--preliminary findings. Investigative radiology 2007, 42(10):671-675.
2. Kellman P, Arai AE, McVeigh ER, Aletras AH: Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magnetic resonance in medicine 2002, 47(2):372-383.
Figures