2093
SMS-bSSFP perfusion imaging with high spatial resolution and coverage using pseudorandom undersampling and compressed sensing reconstruction1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom, 3Cardiovascular MR Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4MR Research Collaborations, Siemens Healthcare Pty Ltd, Melbourne, Australia
Synopsis
CMR perfusion imaging requires high temporal resolution, which limits the achievable spatial coverage and spatial resolution using conventional acquisition techniques. Simultaneous multi-slice (SMS) bSSFP perfusion imaging has been previously demonstrated at 1.5 T with matched spatial resolution and doubled spatial coverage compared to conventional protocols. In this work, we have implemented a pseudorandom undersampling scheme for SMS-bSSFP perfusion with compressed sensing reconstruction to increase in-plane acceleration of SMS-bSSFP imaging, enabling high spatial coverage and spatial resolution perfusion imaging at 1.5 T.
Introduction
Cardiac magnetic resonance (CMR) perfusion imaging is a standard technique used to assess inducible myocardial ischemia. This technique has limited spatial coverage (3-4 slices) and inplane spatial resolution (~2.0mm) due to the required temporal resolution (1 RR interval). However, higher spatial coverage and spatial resolution may improve detection of perfusion defects and could help reducing the incidence of dark rim artifacts. Simultaneous multislice imaging (SMS) enables the simultaneous acquisition of multiple slices and can be applied to perfusion imaging. This can be combined with bSSFP1,2, which provides better SNR/CNR properties than other techniques3. SMS-bSSFP perfusion with T-GRAPPA undersampling and iterative reconstruction can provide doubled slice coverage and matched spatial resolution with respect to conventional protocols4. However, linear undersampling schemes such as T-GRAPPA, which result in coherent aliasing, are suboptimal for compressed sensing (CS) reconstruction5, limiting the maximum achievable acceleration. In this study, we have developed a pseudorandom undersampling scheme for SMS-bSSFP with CS reconstruction and evaluated its potential to achieve high acceleration for CMR perfusion with high spatial resolution and coverage.Methods
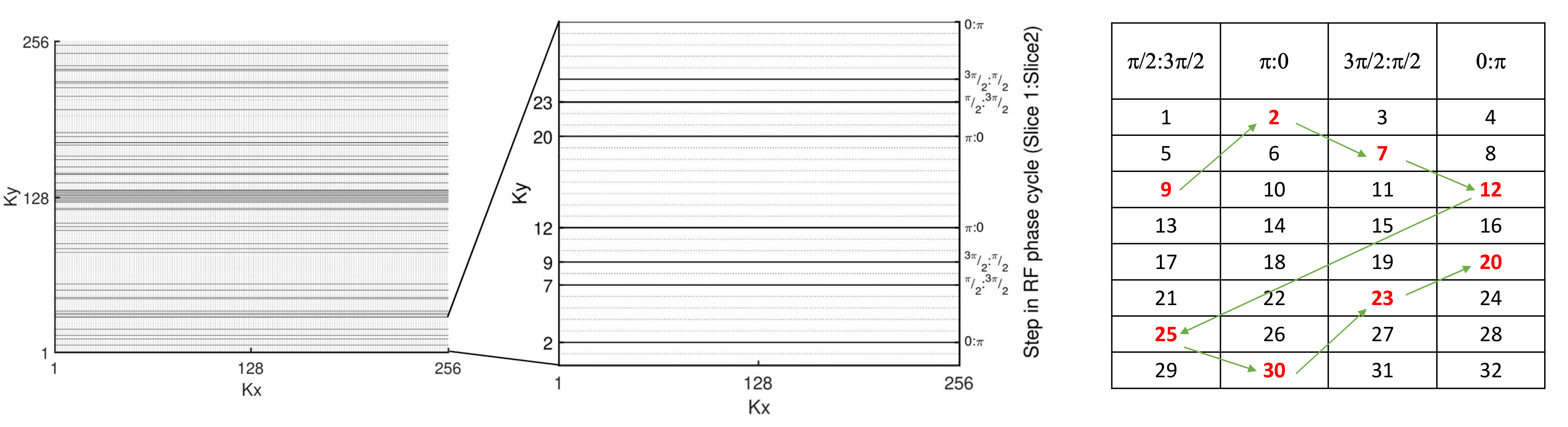
Proposed SequenceA SMS-bSSFP sequence prototype with CAIPIRINHA encoding and GC-LOLA1,2 was modified: a pseudorandom undersampling scheme was developed, as shown in Fig.1. Centre k-space lines are fully sampled while outer k-space lines are pseudo-randomly undersampled to achieve the desired acceleration factor whilst maintaining the required SMS-bSSFP phase cycling scheme (in the case of multiband factor of 2, $$$\phi$$$Slice$$$_1$$$:$$$\phi$$$Slice$$$_2$$$=$$$\pi$$$/2:3$$$\pi$$$/2,$$$\pi$$$:0,3$$$\pi$$$/2:$$$\pi$$$/2,0:$$$\pi$$$) and relative shifts of the bands in image space. To this end, all k-space lines are ordered into 4 bins (each with a particular RF phase cycle step). An equal number of lines is then selected from each bin. The acquisition order is modified to ensure sequential acquisition through the 4 bins. Finally, temporal incoherence is achieved by applying the algorithm to each dynamic phase independently.
Experimental validation
All imaging was performed on a 1.5T MR scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) with an 18-element body coil and 32-channel spine coil.
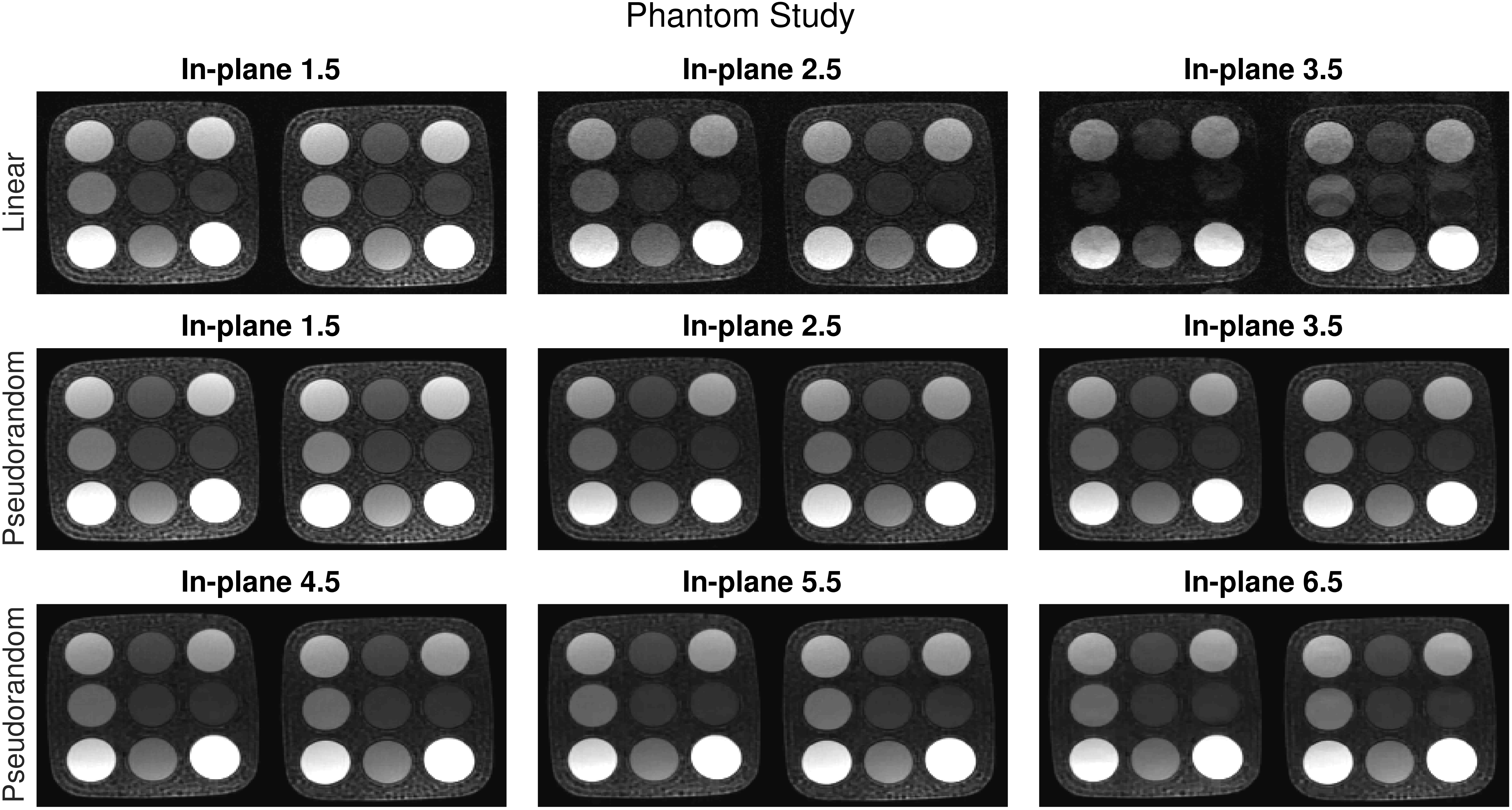
Phantom: SMS-bSSFP perfusion data was acquired in a phantom with pseudorandom (SMS-CS) and T-GRAPPA (SMS-TGRAPPA) undersampling schemes at increasing acceleration factors to confirm whether the proposed acquisition scheme demonstrates improved image quality over linear undersampling. The images were reconstructed using a compressed sensing reconstruction (non-linear iterative reconstruction with L1 regularization in wavelet space6) with fixed spatial and temporal regularisation previously optimised for SMS-bSSFP perfusion4.
In-vivo evaluation: SMS-CS was compared against a conventional 3-slice perfusion protocol in ten patients (8M,mean age 40±16). All underwent two rest perfusion scans under breath-hold, separated by >10min (contrast dose:0.075 mmol/kg each). In random order, the acquisitions consisted of i) Conventional bSSFP protocol and ii) Proposed SMS-CS. Imaging parameters were: TR/TE/α: 2.9ms/1.24ms/50° (SMS-CS), TR/TE/α: 2.5ms/1.04ms/50° (conventional),voxel size: 1.4x1.4x10mm3 (SMS-CS),1.9x1.9x10mm3 (conventional),typical FOV: 360x360mm2,TS 94ms (SMS-CS),74ms (conventional),bandwidth 1302Hz/Px),in-plane acceleration: 5.5 (SMS-CS),3 (conventional),SMS factor: 2 (SMS-CS only). This resulted in a total acceleration of 11 (SMS-CS) and 3 (conventional). The conventional and SMS-CS sequences were reconstructed using a standard GRAPPA reconstruction and an inline SMS-enabled2 prototype compressed sensing reconstruction6, respectively. Qualitative assessment was performed by consensus of two expert readers, blinded to clinical information. Overall image quality was assessed for each slice on a 4-point scale (0:non-diagnostic, 1:major artefact, 2:minor artefact, 3:excellent), and an overall perceived SNR score was determined for each sequence (0:poor SNR, 1:major noise, 2:minor noise, 3:high SNR). Finally, each AHA segment7 was scored as diagnostic/non-diagnostic for each sequence.
Results
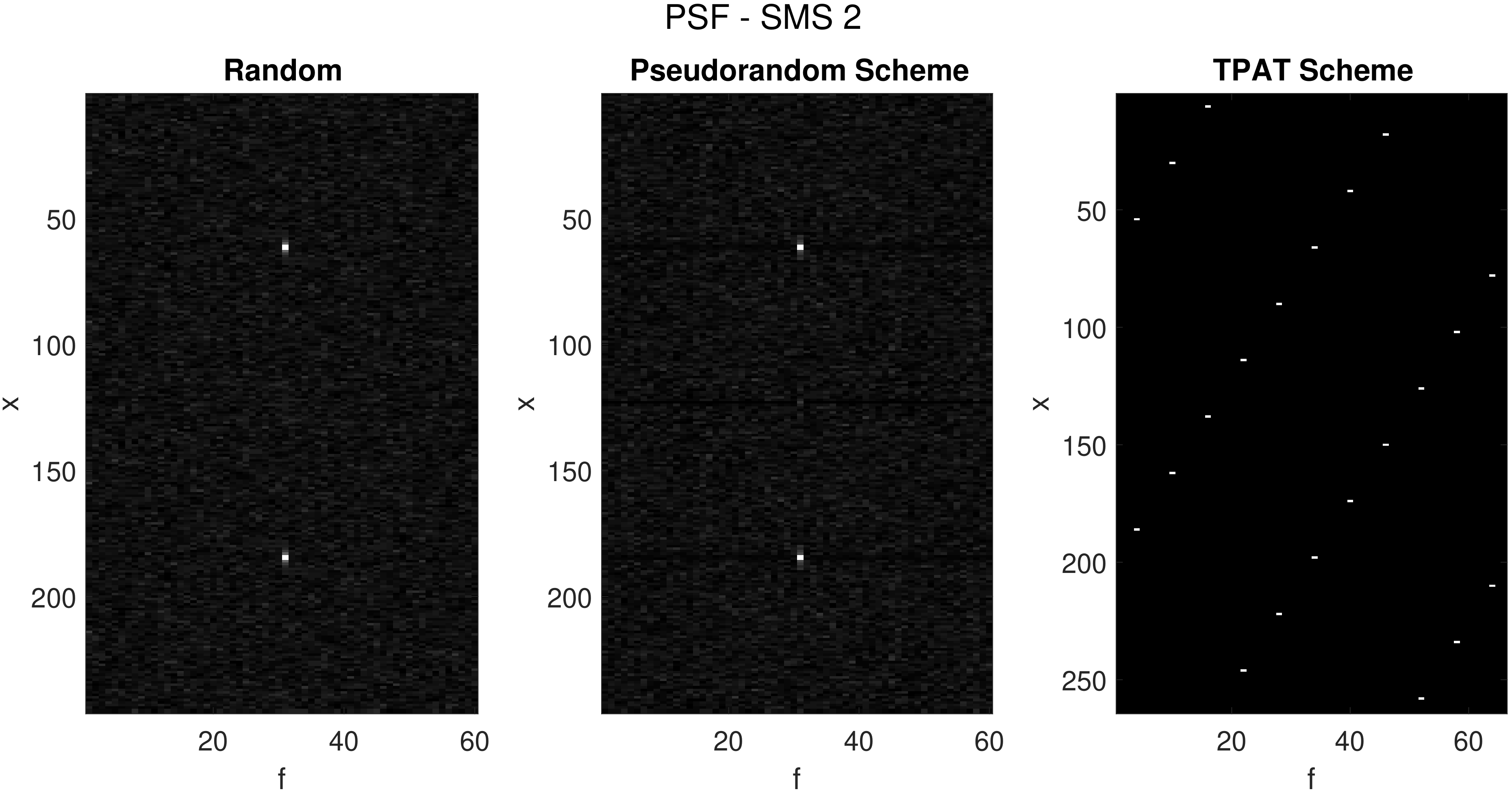
The x-f representation8 (Fig.2) of the proposed SMS-bSSFP pseudorandom undersampling scheme with SMS 2 closely mimics the x-f space of a theoretically random scheme. Conversely, the T-GRAPPA sampling scheme results in multiple coherent peaks, rendering this scheme sub-optimal for compressed sensing reconstruction. SMS-CS improves image quality compared with SMS-TGRAPPA in a phantom (Fig.3). Image quality of the SMS-TGRAPPA scheme is poor at high acceleration factors (>=7). SMS-CS provided excellent image quality up to a total acceleration of 11. Slight artefacts begin to be visible at a total acceleration of 13. Fig.4 shows an example patient study acquired with the conventional and proposed SMS-CS sequence. Over all patients, there was no significant difference between the mean image quality score of the SMS-CS and the conventional sequence (Fig.5a, 2.5±0.4 vs. 2.8±0.2, p=0.08, Wilcoxon signed ranks test) while SMS-CS led to higher perceived SNR (Fig.5b, 2.9±0.3 vs. 2.2±0.6, p=0.04, Wilcoxon signed ranks test) and higher percentage of diagnostic segments (Fig.5c, 100% vs. 94%, p=0.004, McNemar test) than the conventional sequence.Discussion
The proposed SMS-CS sequence enabled an acceleration factor of 11. However, the temporal regularization can introduce artefacts in the presence of poor breath-hold. Therefore, integration of motion estimates in the reconstruction process may prove useful in this context and will be investigated in future work. The proposed sequence was evaluated during rest perfusion protocols. Validation in patients with coronary artery disease and during stress conditions will be the focus of future studies to determine diagnostic performance.Conclusions
The proposed SMS-bSSFP scheme with pseudorandom undersampling and compressed sensing reconstruction enables increased in-plane resolution of 1.4x1.4mm2 with 6-slice coverage for 1.5 T SMS-bSSFP perfusion imaging. This sequence resulted in improved diagnostic confidence, higher perceived SNR, and no significant difference in image quality, when compared to a conventional sequence.Acknowledgements
This work was supported by the EPSRC grant (EP/R010935/1), the Wellcome EPSRC Centre for Medical Engineering at Kings College London (WT 203148/Z/16/Z), the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London, and Siemens Healthineers. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Stab D, Ritter CO, Breuer FA, Weng AM, Hahn D, Köstler H. CAIPIRINHA accelerated SSFP imaging: CAIPIRINHA Accelerated SSFP Imaging. Magnetic Resonance in Medicine. 2011;65(1):157-164. doi:10.1002/mrm.22600
2. Stab D, Speier P. Gradient-controlled local Larmor adjustment (GC-LOLA) for simultaneous multislice bSSFP imaging with improved banding behavior. Magnetic Resonance in Medicine. 2019;81(1):129-139. doi:10.1002/mrm.27356
3. Wang Y, Moin K, Akinboboye O, Reichek N. Myocardial first pass perfusion: Steady-state free precession versus spoiled gradient echo and segmented echo planar imaging. Magnetic Resonance in Medicine. 2005;54(5):1123-1129. doi:10.1002/mrm.20700
4. Nazir MS, Neji R, Speier P, et al. Simultaneous multi slice (SMS) balanced steady state free precession first-pass myocardial perfusion cardiovascular magnetic resonance with iterative reconstruction at 1.5 T. Journal of Cardiovascular Magnetic Resonance. 2018;20(1). doi:10.1186/s12968-018-0502-7
5. Lustig M, Donoho DL, Santos JM, Pauly JM. Compressed Sensing MRI. IEEE Signal Processing Magazine. 2008;25(2):72-82. doi:10.1109/MSP.2007.914728
6. Liu J, Lefebvre A, Zenge MO, Schmidt M, Mueller E, Nadar MS. 2D bSSFP real-time cardiac CINE-MRI: compressed sensing featuring weighted redundant Haar Wavelet regularization in space and time. J Cardiovasc Magn Reson. 2013;15(Suppl 1):P49. doi:10.1186/1532-429X-15-S1-P49
7. Cerqueira MD, Weissman NJ, Dilsizian V et al. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association, Circulation. 2002;105:539-542
8. Tsao J, Boesiger P, Pruessmann KP. k-t BLAST andk-t SENSE: Dynamic MRI with high frame rate exploiting spatiotemporal correlations. Magn Reson Med. 2003;50(5):1031-1042. doi:10.1002/mrm.10611
Figures