2082
Tissue Characterization by Mapping and Strain Cardiac MR for Detection and Monitoring of Myocardial Injury in Fulminant Myocarditis1Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Synopsis
Fulminant myocarditis is a rare form of acute severe myocarditis and accurate detection and monitoring of the inflammatory myocardial edema is essential for clinical decision-making. We therefore evaluated the ability of multiparametric CMR to detect and monitor the inflammation myocardial alterations and to differentiate acute and convalescent stage of fulminant myocarditis.
Introduction:
Accurate detection and monitoring of the inflammatory myocardial injuries is essential for clinical decision-making. Novel quantitative T1 and T2mapping can detect myocardial edema and further enhance the diagnostic accuracy of cardiac magnetic resonance(CMR).1 Furthermore, cardiac strain has the ability to assess regional and global myocardial dysfunction and could provide additional useful information.2 So far, however, there is no investigations focusing on monitoring the disease activity of fulminant myocarditis by using multiparametric CMR. Therefore, the purpose of this prospective study was to investigate whether multiparametric CMR could detect and monitor inflammation myocardial alterations in fulminant myocarditis.Methods:
Nineteen patients(35 ± 14 years, 37% male) with clinical diagnosis of fulminant myocarditis underwent CMR examinations at 3.0T(MAGNETOM Skyra,Siemens Healthcare,Erlangen,Germany) in the acute phase and at 3-months follow up. The control group consisted of 19 healthy volunteers. The CMR protocol included cine, black blood T2-weighted imaging, T1mapping, T2mapping and late gadolinium enhancement(LGE). Cardiac strain was evaluated by feature tracking.Results:
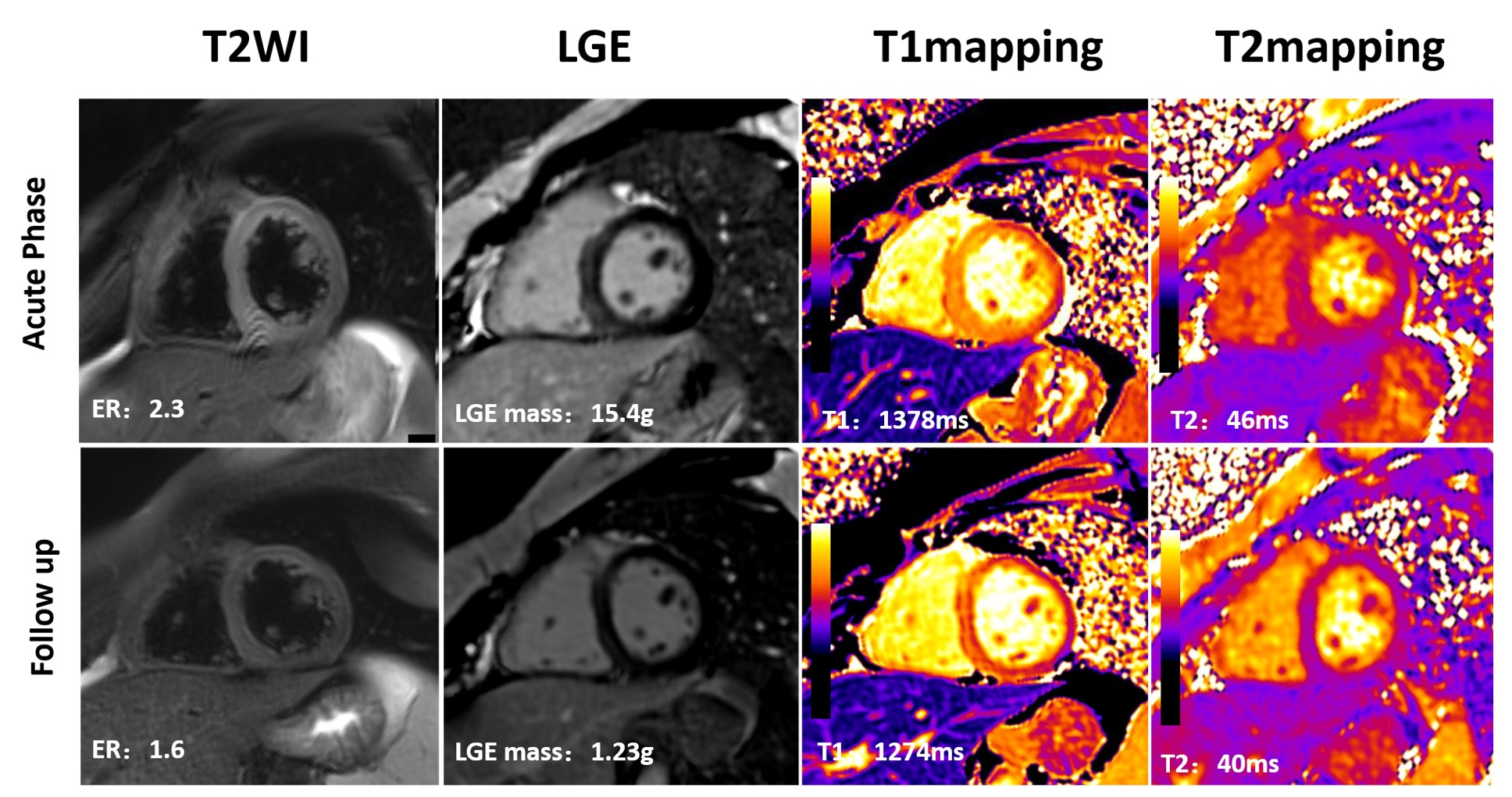
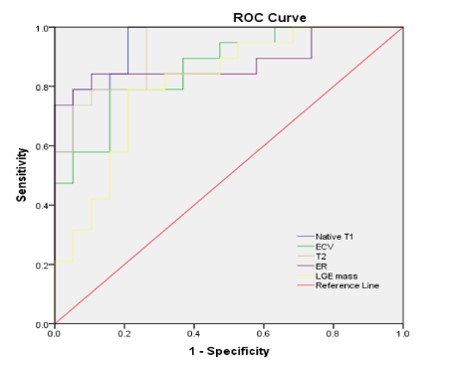
The left ventricular mass index (64 [57, 76] versus 52 [47, 63], P<0.05) and interventricular septum thickness (10.5 [9, 11.3] versus 8.3 [6.6, 9.8], P<0.001) in acute stage was significantly higher compared with controls, and normalized at the chronic stage. All quantitative inflammation metrics, including edema ratio, LGE mass, native T1,T2 and extracellular volume were significantly(all P<0.001) decreased in the follow-up scan (Fig. 1), but still higher compared to controls. Compared with the controls, strain indices were all significantly(all P<0.001) impaired in acute stage. Native T1 and T2 values led to excellent diagnostic accuracy for discriminating fulminant myocarditis from healed myocarditis, with AUC of 0.947 and 0.931 (Fig. 2).Discussion and conclusions:
In this study, the preliminary data from our study demonstrate all quantitative CMR parameters gradually diminished with the resolution of acute inflammation and myocardial edema. Similar to previous stuides,3 we found that the strain parameters slightly improved from the acute to chronic phase, but still significantly impaired compared to the control group. Accordingly, strain analysis may offer additional useful information regarding the functional change during the course of myocarditis. In conclusion, multiparametric CMR could accurately detect and monitor inflammation myocardial injuries in patients with fulminant myocarditis. Native T1 and T2 values achieved excellent diagnostic performance in distinguishing acute from healed myocarditis.Acknowledgements
No acknowledgement found.References
1 Ferreira VM, Piechnik SK, Dall'Armellina E, et al. Native T1-mapping detects the location, extent and patterns of acute myocarditis without the need for gadolinium contrast agents. J Cardiovasc Magn Reson 2014;16:36
2 Luetkens JA, Schlesinger-Irsch U, Kuetting DL et al. Feature-tracking myocardial strain analysis in acute myocarditis: Diagnostic value and association with myocardial oedema. EUR RADIOL 2017;27:4661-4671
3 Luetkens JA, Petry P, Kuetting D, et al. Left and right ventricular strain in the course of acute myocarditis: A cardiovascular magnetic resonance study. Rofo 2018;190:722-732
Figures