2077
Improvement of distortion-free cardiac diffusion weighted imaging (DWI) using motion-compensated single-shot turbo spin-echo (MoCo-TSE) DWI1Department of Radiological Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
We compared the image quality of the motion-compensated (MoCo) and conventional (non-MoCo) cardiac TSE-DWI by visual evaluation and homogeneity evaluation. MC-TSE-DWI achieved superior image quality compared with non-MoCo-TSE-DWI in all b-values and all segments. MoCo-TSE-DWI improves the image quality and may increase the diagnostic potential.
Introduction
Cardiac DWI has a potential to achieve improved clinical diagnosis through novel micro-structural and functional assessment1. In previous study, we reported a utility of cardiac turbo spin-echo based DWI (TSE-DWI) with peripheral gating in comparison with conventional EPI-DWI with cardiac gating2. One of the challenges of cardiac TSE-DWI is to maintain higher signal uniformities both within the slices and inter slices. Furthermore, current TSE-DWI suffers from its low SNR and is sensitive to cardiac motion compared to EPI3. Recently, a utility of motion-compensated (MoCo) DW-EPI using motion-compensated motion probing gradient (MPG) has been reported to quantify the diffusion and perfusion4. Therefore we attempted to combine both TSE-DWI and MoCo-DWI (MoCo-TSE-DWI). The purpose of this study was to compare the image quality of the cardiac TSE-DWI between MoCo-TSE-DWI and conventional TSE-DWI (non-MoCo-TSE-DWI).Methods
[Subjects] Ten healthy volunteers (age range: 28-43 years) were examined using 3.0T MR clinical imager (Ingenia, Philips Healthcare). To validate the feasibility of MoCo-TSE-DWI, we compared with conventional TSE-DWI. [Imaging quality assessment] We previously determined the actual trigger delay (TD) and data acquisition window using CINE imaging. We assessed the signal uniformity of myocardium on the short-axis images of left ventricle. The myocardium was divided into 6, 6, and 4 segments for the basal, mid, and apical, respectively5. Circular region of interests (ROIs) were drawn on 16 myocardial segments. Subsequently, the mean and standard deviation were measured. Furthermore, three radiologists evaluated usefulness in diagnosis visually myocardium using 4-points scale. [Signal uniformity assessment] The coefficient of variation (CV) was used as an estimation of myocardial signal uniformity as follows: CV = Standard deviation/Average value [Statistical analysis] Statistical analysis was performed with Wilcoxon signed-rank test and judged the difference as significant at p<0.05.Results&Discussion
CV of MoCo-TSE-DWI was significantly lower at mid and apical segments than those from TSE-DWI. Visual score from MoCo-TSE-DWI were significantly higher at basal and mid segments than those from TSE-DWI. The number of non-assessable myocardial decreased of about 30% in the MoCo-TSE-DWI compared with the TSE-DWI. TSE-DWI using MoCo improved the signal uniformity entire circumference of myocardium. There was no difference in visual score and availability in the apical segments between two methods. There was no difference in visual score between b-150(s/mm²) and b-300(s/mm²) using MoCo-TSE-DWI. In contrast, visual score was for b-300(s/mm²) significantly lower than for b-150(s/mm²) using non-MoCo. MoCo-TSE-DWI has the possibility to apply further higher b-values. MoCo-TSE-DWI can provide robust diffusion weighted images by compensating myocardial motion. Latterly, a utility of cardiac EPI-DWI using acceleration MoCo (aMoCo) has been reported to eliminate more pulsatile effects than MoCo6. In the future, a combination with aMoCo is also being considered.Conclusion
MoCo-TSE-DWI improves the image quality and might increase the diagnostic potential, compared with conventional (non-MoCo) TSE-DWI. Cardiac MoCo-TSE-DWI could reduce myocardial signal un-uniformity due to myocardial slight movement by applying motion-compensated MPGs, and it might be useful for further assessment of the cardiac pathology.Acknowledgements
No acknowledgement found.References
(1) Nielles-Vallespin S,et.al,Cardiac Diffusion: Technique and Practical Application. J Magn Reson Imaging.2019 Sep 4. (2) Goto Y ,et.al,24th Annual Meeting of ISMRM,Singapore,2016 (Abstract2016). (3) Alsop DC. Phase insensitive preparation of single-shot RARE: application to diffusion imaging in humans. Magn Reson Med. 1997 Oct;38(4) (4) Froeling M, et.al. 22th Annual Meeting of ISMRM,Italy,2014 (Abstract2014). (5) Circulation,105:539-42,2002. (6) Nakamura T, et.al,22th Annual Meeting of ISMRM,Italy,2014 (Abstract2014).Figures
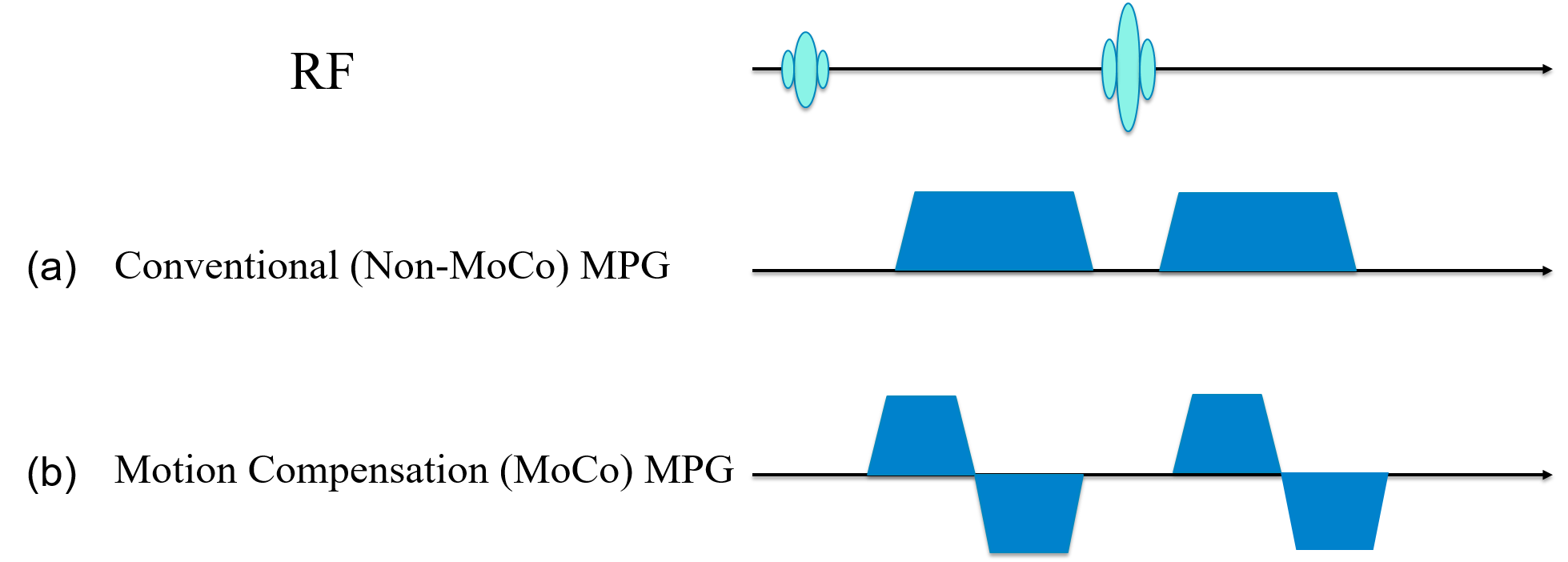
Figure 1 We show a motion compensation diffusion gradient with gradient moment nulling. (a)No phase correction for spin motion signal loss. (b) 1st moment and of gradient = 0 velocity term motion compose.
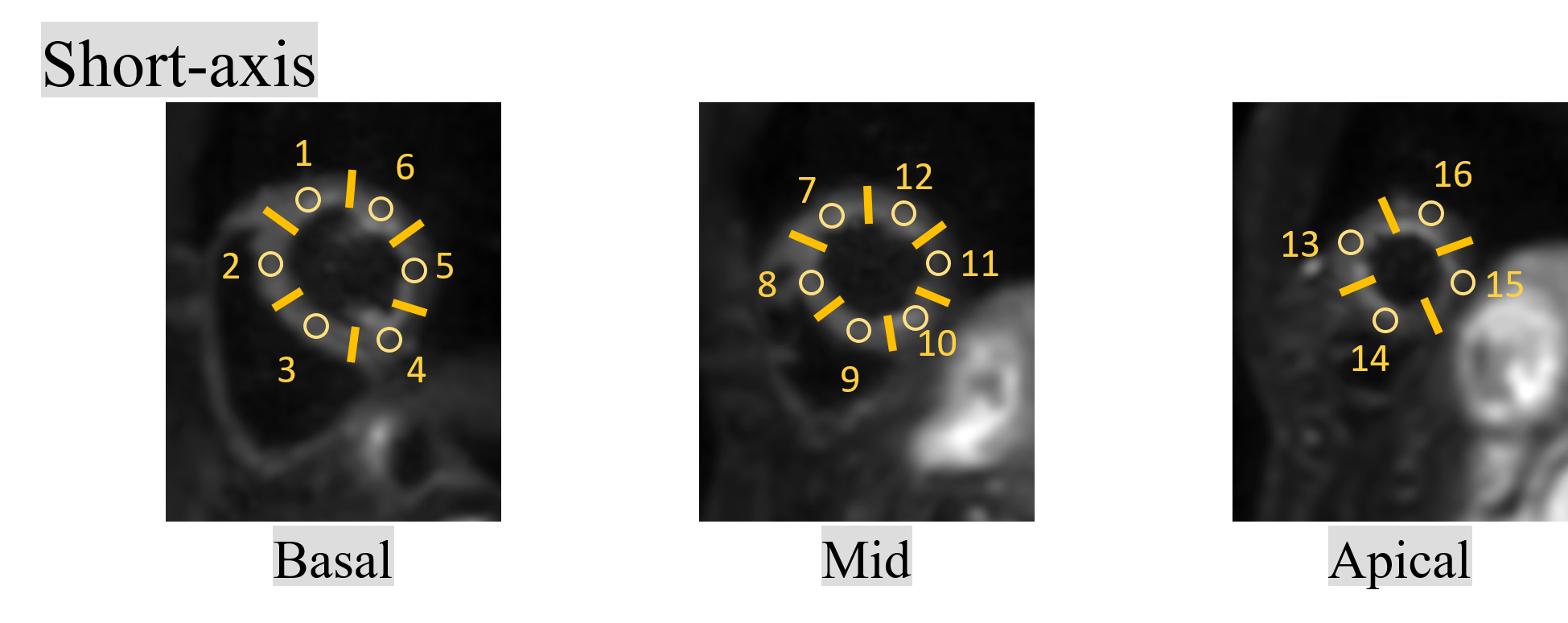
Figure 2. We show segment on left ventricular short axis image determined to evaluate CV and visual analysis.
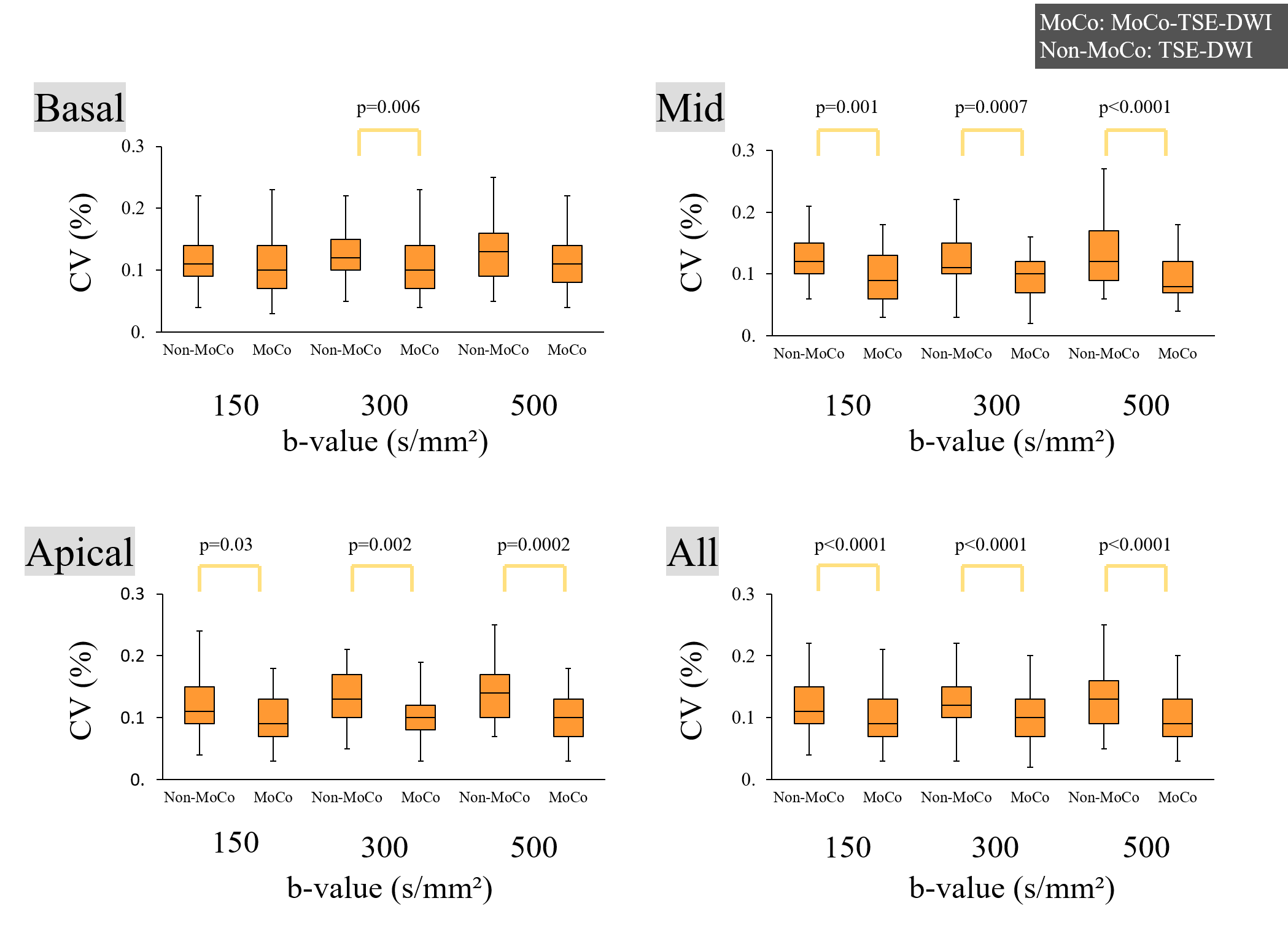
Figure 3. We show results of CV at the heart in each myocardial segments and each b-values.
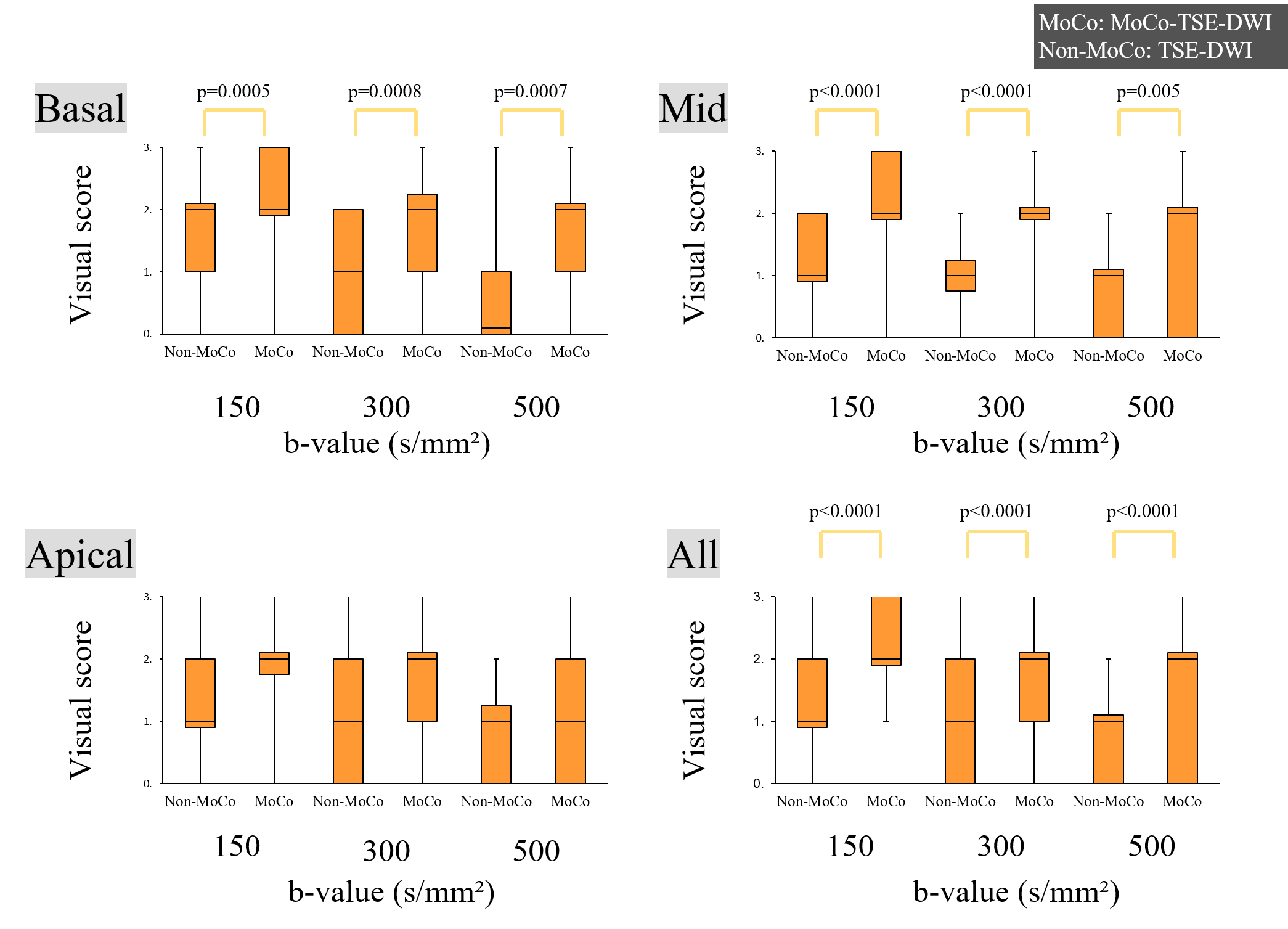
Figure 4. We show results of visual score analysis at the heart in each myocardial segments and each b-values.
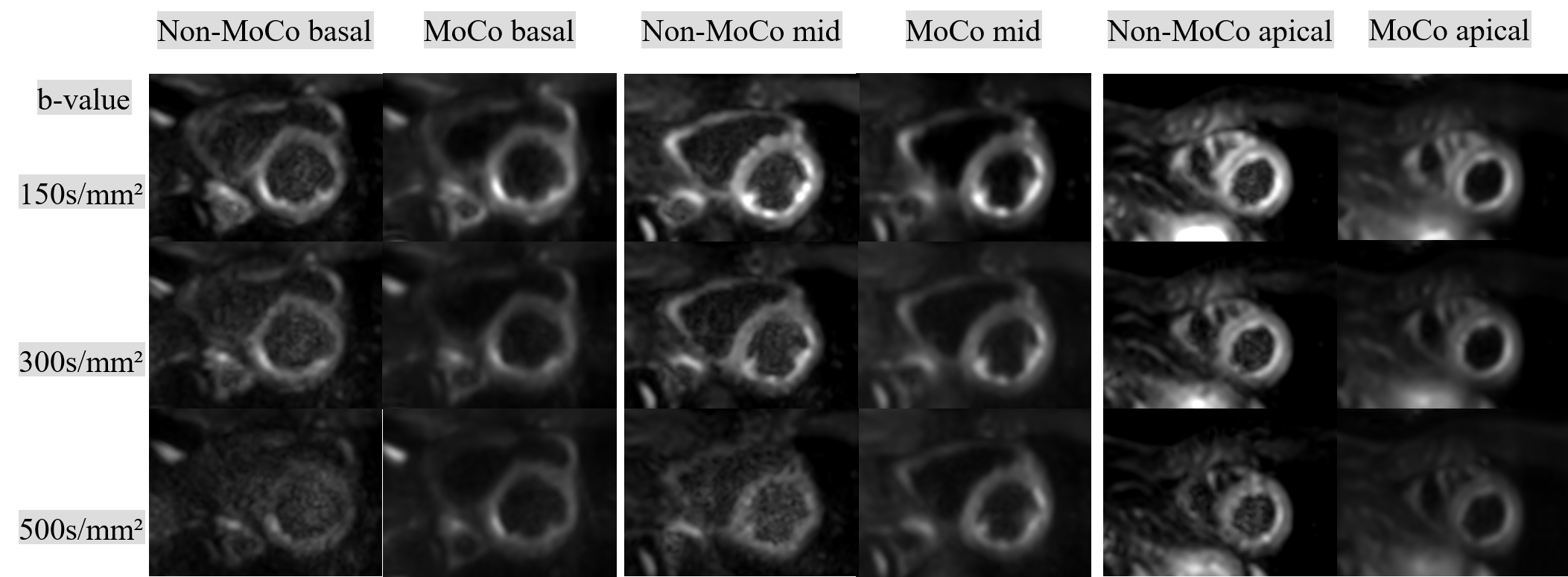
Figure 5. A representative case of MoCo-TSE-DWI(MoCo) and conventional TSE-DWI (Non-MoCo) in each b-values are shown.Visualization of the cardiac wall was improved with MoCo as compared with Non-MoCo at all b-values.