2070
Evaluation of factors contributing to the correction of the effect of heartrate variation on MOLLI using BlochSolver1Kyorin University Faculty of Heaith Science, Mitaka, Japan
Synopsis
Fast cardiac T1 mapping including MOLLI with ECG-gating leads to poorer T1 measurement accuracy, since the recovery time of the longitudinal magnetization changes with heart rate variation. Ikekawa et al. proposed correction methods for the changes in the inversion recovery time at each sampling point and in that of longitudinal magnetization on the heartrate variation; however, the specific factor that predominantly improves T1 measurement remains unclear. Here, we investigated the dominant effect of the proposed correction method in the effect of heartrate variation on T1 measurement using BlochSolver.
Introduction
T1 mapping facilitates quantitative evaluation of myocardial characteristics. Fast T1 mapping 1-4, including modified look-locker inversion recovery (MOLLI), can be used to acquire images within a single breath-hold with electrocardiography (ECG) gating. Therefore, T1 measurement accuracy may be influenced by heart-rate variation1,5-7. There are two possible factors associated with this effect:(1) change in the inversion recovery time (TI) at each sampling point, (2) change in the recovery time of longitudinal magnetization. Ikekawa et al. proposed correction methods for these effects on heartrate variation8, but the factor that is responsible for improving T1 measurement accuracy remains unclear. Therefore, we investigated the dominant effect of the proposed correction method in the effect of heartrate variation on T1 measurement. We used BlochSolver9-11, a magnetic resonance imaging (MRI) simulator, that can freely incorporate heartrate variation, as needed.Methods
We set RR at 1000 ms (HR60; N) as a reference, and to simulate heartrate variation we also set the following parameters; (1) shortened RR=750 ms (HR80; S), (2) mild-shortened RR=875 ms (HR69; MS), (3) mild-extended RR=1125 ms (HR53; S) and (4) extended RR=1250 ms (HR48; L). We used heartrate variation in 5 patterns: 1. N-N-N-N (N=1000 ms), 2. MS-MS-MS-MS (MS=875 ms), 3. S-S-S-S (S=750 ms), 4. ML-ML-ML-ML (ML=1125 ms) and 5. L-L-L-L (L=1250 ms). We simulated an electrocardiogram-gated 2D gradient echo single-slice image using the BlochSolver. A 3T MRI T1 standard value phantom was used. The scanning conditions of the MOLLI method were 5.1/2.5 ms, 15°, and 128×256 for TR/TE, FA, and the matrix, respectively. We used the MOLLI protocol of 5(3)3 with initial TI settings (50, 250 ms). Correction effect in T1 measurements on heartrate variations was ensured using the following expression proposed by Ikegawa et al: S=A-Bβexp(-TI/T1*), where TI represents the inversion time, and T1* is the apparent T1, and β=1-γβ, γ=exp(-TI/T1*).βrepresents the factor for correcting the change in the recovery time of longitudinal magnetization. Additionally, TI reflects the actual RR instead of the reference RR to correct for the changes in the TI. The measured values were used to fit the 3-parameter model to estimate A, B, and T1*, and T1 values were calculated from A, B, and T1*: T1=T1*(B/A-1), respectively.Results
Measured T1 values changed with heartrate variation, and were overestimated as the RR became shorter, and underestimated as the RR became longer, when compared with the outcomes of reference RR. Except for the shortest T1 value, the maximum error of T1 measurement due to heartrate variation was 11.5% (Figure 1). Using the proposed correction method, the measured T1 value improved to nearly that of the reference RR except the pattern 5(S-S-S-S), and error was less than 1%. Minor improvements were also noted in pattern 5, with a maximum error of 6.7% compared to 11.5% before correction (Figure 2). The proposed correction method included two factors: with regard to the changes in (1) TI at each sampling point, (2) recovery time of longitudinal magnetization. These factors were separated and corrections were performed for patterns 1 and 2. Both patterns demonstrated a greater degree of correction in the T1 measurement accuracy when only the former correction was performed, and its contribution was greater than 99% to the proposed correction method. Alternatively, the contribution of the latter correction alone was less than 1% (Figure 3,4).Discussion and Conclusion
Here, the heartrate variation resulted in an error of approximately 11.5% in T1 measurements via MOLLI with ECG-gating. The proposed correction method could improve the measured T1 values to the T1 values noted in the reference RR pattern. These results suggest that it is imperative to record the heartrate variation with MOLLI and use it for correction. Specifically, we observed that the correction for the changes in TI at each sampling point greatly contributed to the measurement accuracy. However, this may change with regards to the MOLLI protocol or the more complicated heartrate variation such as extrasystole and requires further investigation. Furthermore, BlochSolver can be a more effective tool since it can freely incorporate heartrate variation as required. The difference between the true T1 value and measured T1 value in reference RR pattern may be associated with the pulse sequence and MOLLI protocol used in this study. These optimizations also need to be studied in the future.Acknowledgements
No acknowledgement found.References
1. Peter Kellman, et al. T1-mapping in the heart: accuracy and precision. J Cardiovasc Magn Reson. 2014;16:2
2. Daniel R Messroghli, et al. Modified look-locker inversion recovery (MOLLI) for high- resolution T1 mapping of the heart. Magn Reson Med. 2004;52:141-146
3. Kelvin Chow, et al. Saturation recovery single-short acquisition (SASHA) for myocardial T1 mapping. Magn Reson Med. 2014;71:2082-2095
4. Shigehide Kuhara, et al. Polarity-corrected TI prep tool for delayed-enhancement MR imaging and T1 mapping. ISMRM. 2014;2447
5. Michelle Fitts, et. al. Arrhythmia insensitive rapid cardiac T1 mapping pulse sequence. Magn Reson Med. 2013;70:1274-1282
6. Thomas Kampf, et al. An analytical model which determines the apparent T1 for Modified Look-Locker Inversion Recovery—Analysis of the longitudinal relaxation under the influence of discontinuous balanced (classical MOLLI) and spoiled gradient echo readouts. Z Med Phys. 2018;28:150-157
7. Lei Zhao, et al. Systolic MOLLI T1 mapping with heart-rate-dependent pulse sequence sampling scheme is feasible in patients with atrial fibrillation. J Cardiovasc Magn Reson. 2016;18:13
8. Rei Ikegawa, et al. Correction of the effects of heart rate changes on MOLLI, ISMRM. 2019;2101
9. Kose R, et al. BlochSolver: A GPU-optimized fast 3D MRI simulator for experimentally compatible pulse sequences. J Magn Reson 2017; 281: 51-65. 2.
10. Kose R, et al. A fast GPU-optimized 3D MRI simulator for arbitrary k-space sampling. Magn Reson Med Sci, 2019; 18: 208-218. 3.
11. Kose K, et al. Bloch image simulations of brain pulse sequences using a GPU-installed gaming PC. Proc. ISMRM, p4829, 2019.
Figures
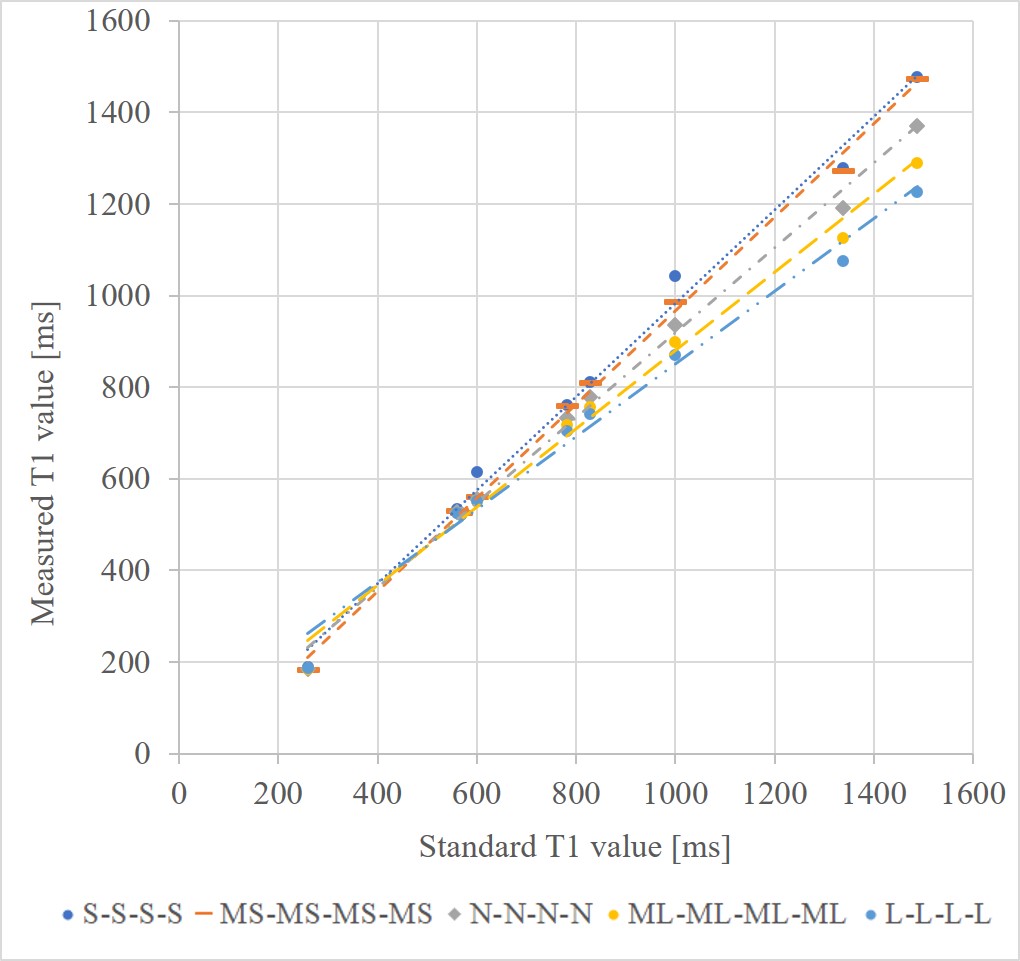
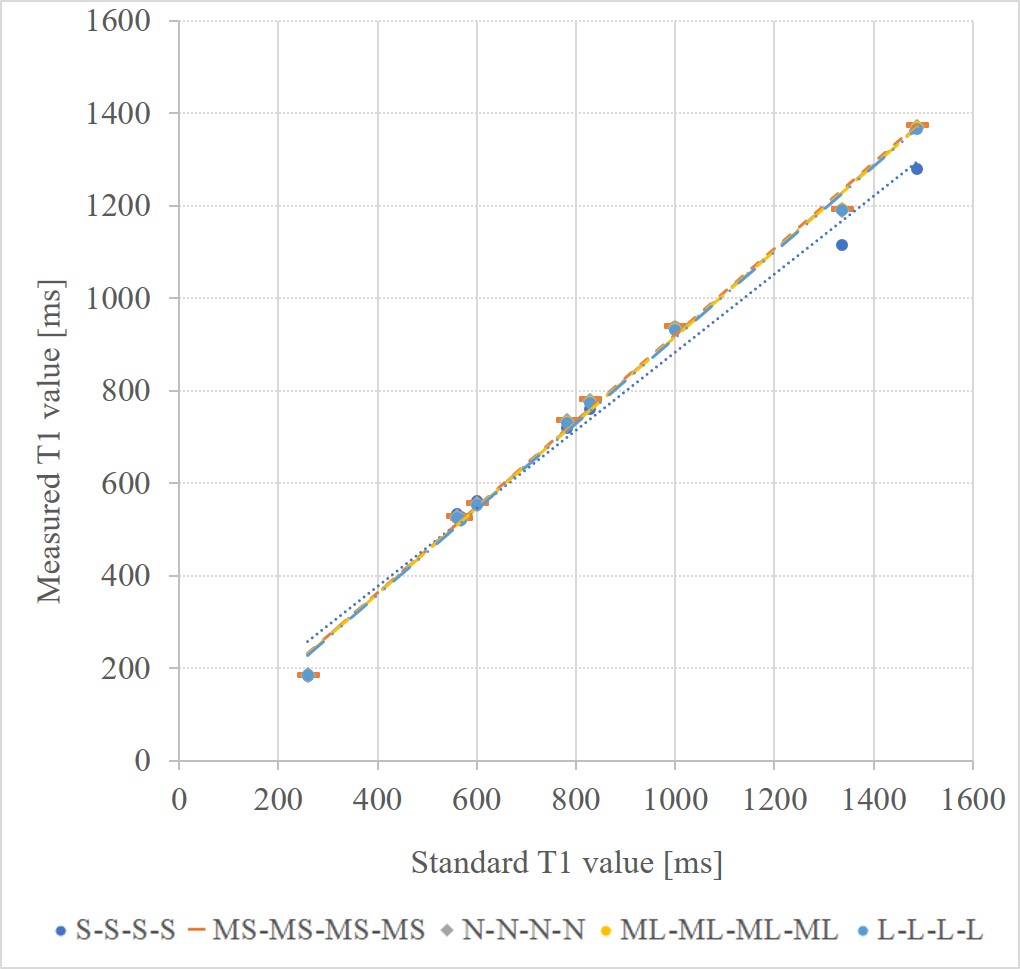
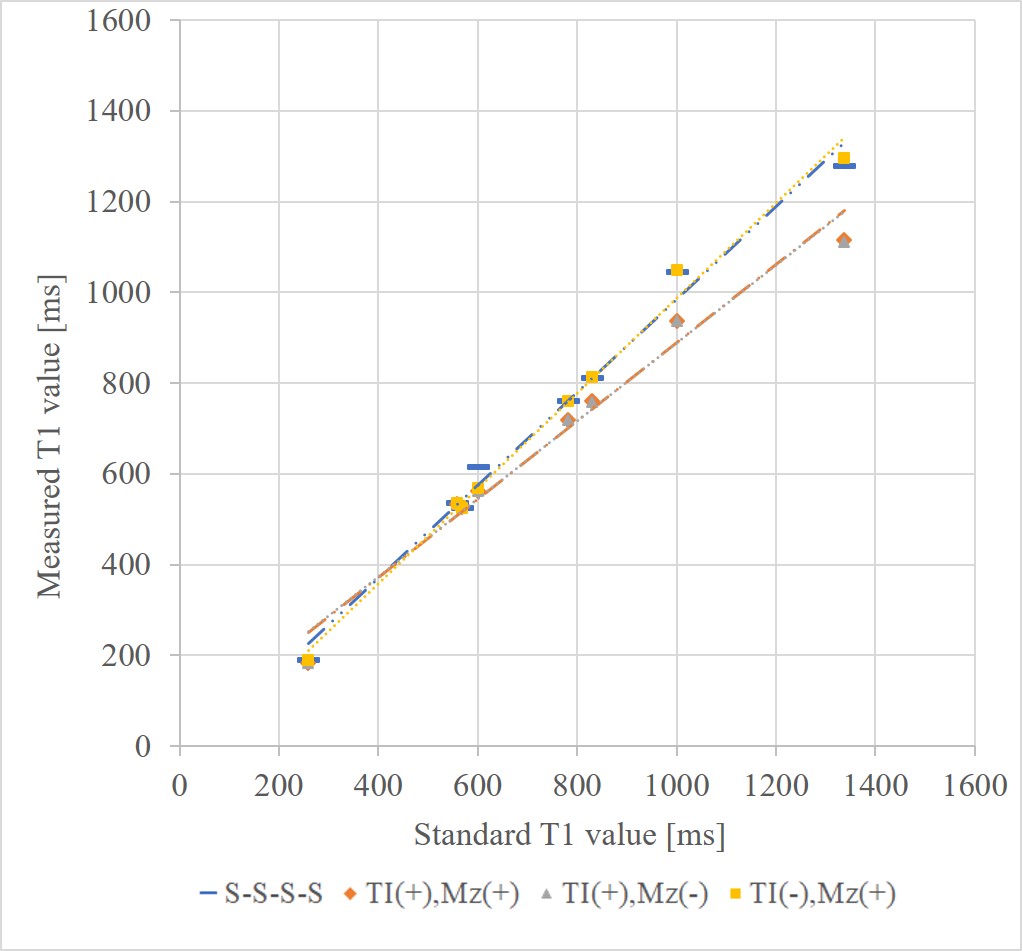
Figure 3. Evaluation for the dominant effect of the correction (S-S-S-S pattern)
TI(+), Mz(+): proposed correction method
TI(+), Mz(-): correction for only the change in TI at each sampling point
TI(-), Mz(+): correction for only the change in the recovery time of longitudinal magnetization
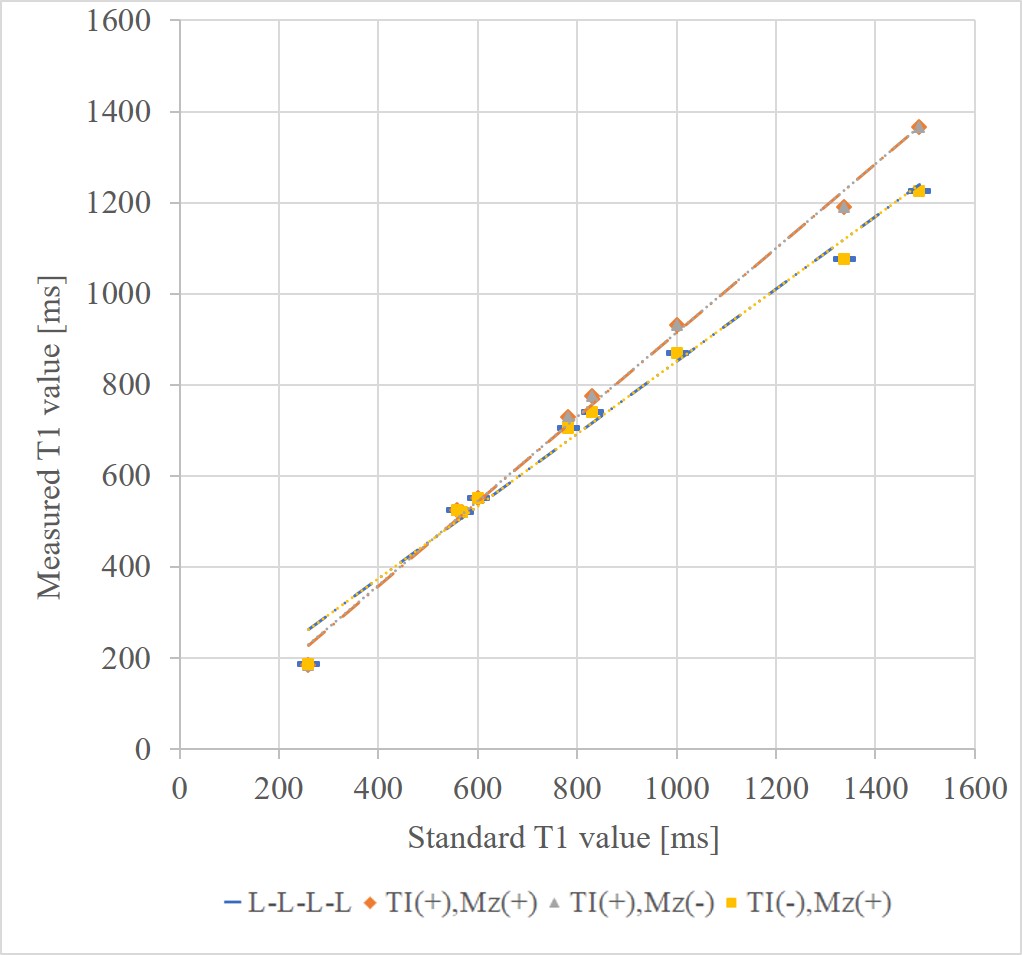
Figure 4. Evaluation for the dominant effect of the correction (L-L-L-L pattern)
TI(+), Mz(+): proposed correction method
TI(+), Mz(-): correction for only the change in TI at each sampling point
TI(-), Mz(+): correction for only the change in the recovery time of longitudinal magnetization