2053
Motion-Sensitive (MoSe) CINE imaging: utility for improving robustness of myocardial quantitative mapping1Department of Radiological Services, Women's Medical University Hospital, tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Women's Medical University Hospital, tokyo, Japan, 3Philips Japan, tokyo, Japan
Synopsis
Motion-Sensitive (MoSe) CINE imaging, based on T2FFE (also known as PSIF) sequence, could clearly visualize the motion-insensitive cardiac timing due to its motion sensitivity and it point out when is the best timing to trigger for both systole and diastole to prevent signal loss and/or motion artifacts effectively. Confirming the MoSe CINE imaging in addition to conventional bSSFP CINE imaging could be useful to determine accurate trigger delay (TD) setting which leads to increase the robustness of image quality in quantitative myocardial mapping and other imaging such as T2-weighted imaging and diffusion-weighted imaging.
Introduction
Myocardial quantitative mapping such as T1, T2, and T2* map is promising method for evaluating myocardial tissue characteristics [1]. Commonly, the exact cardiac trigger delay (TD) for the acquisition is determined by either using system automatic pre-set timing (operator can choose as “diastole” or “systole”) or directly observing cardiac morphology changes using balanced-SSFP (bSSFP) CINE imaging. Although an operator can confirm morphology changes of the heart during one cardiac cycle by using bSSFP CINE imaging and can apply quasi-optimal TD visually, there are still sub-optimal choice of TD in some cases using only bSSFP CINE, resulting in increase of motion artifacts and deterioration of image quality [2,3], particularly in case of high heart rates. To determine the exact TD for enabling high image quality with high reproducibility, direct visualization of “motion-sensitive timing (TD)” is desirable in addition to observe morphology changes.T2-fast field echo (T2FFE) is a variant of SSFP, which can provide T2-weighted contrast despite the gradient echo (GRE) sequence [4]. The T2FFE sequence is also called ‘reversed fast imaging with SSFP, PSIF’. T2FFE theoretically has a greater sensitivity to motion [5]. The signals from moving spins are strongly attenuated, and motion artifacts are observed because a steady-state cannot be attained for the spins that move along a magnetic field gradient. Nevertheless, one study demonstrated that T2FFE achieves rapid 3D T2-weighted black- blood imaging while minimizing the impact of motion using a low flip angle under the shortest repetition time (TR) and the shortest echo time (TE) conditions similar to the bSSFP sequences [6].
We hypothesized that T2FFE would be promising for direct visualization of motion-insensitive cardiac-phase timing. In this study, we attempted to extend this technique to cardiac CINE imaging, Motion-Sensitive (MoSe) CINE imaging, for determining exact TD timing and evaluated its feasibility for improving the robustness of cardiac quantitative mapping.
Methods
A total of five volunteers were examined on a 3.0T system (Ingenia, Philips Healthcare). The study was approved by the local IRB, and written informed consent was obtained from all subjects.To demonstrate the feasibility of using MoSE-CINE imaging for optimal TD selection, we compared two procedures: one is conventional approach (operator set the preset TD timing for diastole and TD was automatically determined by MR system software) and visual approach using MoSE-CINE (operator visually defined the diastole and check whether heart structure is not obscured by cardiac movements at the determined TD). To evaluate quantitatively, regions-of-interest (ROIs) were placed on 16 segments of the myocardium in the short axis image of the left ventricle [7], standard deviation (SD) of relaxation times in respective ROIs were compared between both approaches, and assessed by Wilcoxon signal-rank test.
Imaging parameters for MoSe-CINE imaging: T2FFE with free-breathing and retrospective cardiac gating, FOV=380mm, pixel size=2.64*1.7mm, slice thickness=12mm, flip angle=25, number of heart phase=32, TR=6.6ms, TE=3.7ms, ProSet water excitation 121, NSA=16, and acquisition time=2m55s.
Results & Discussion
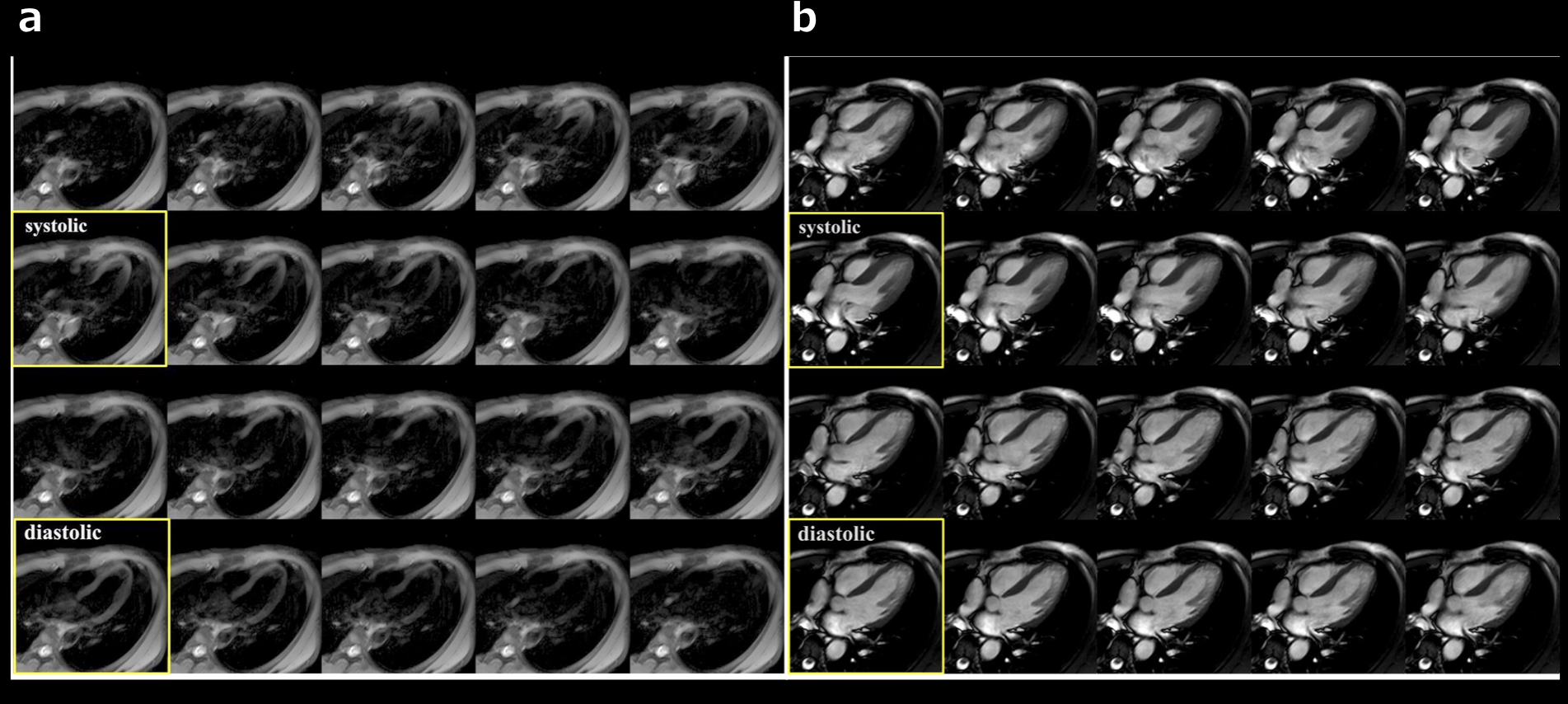
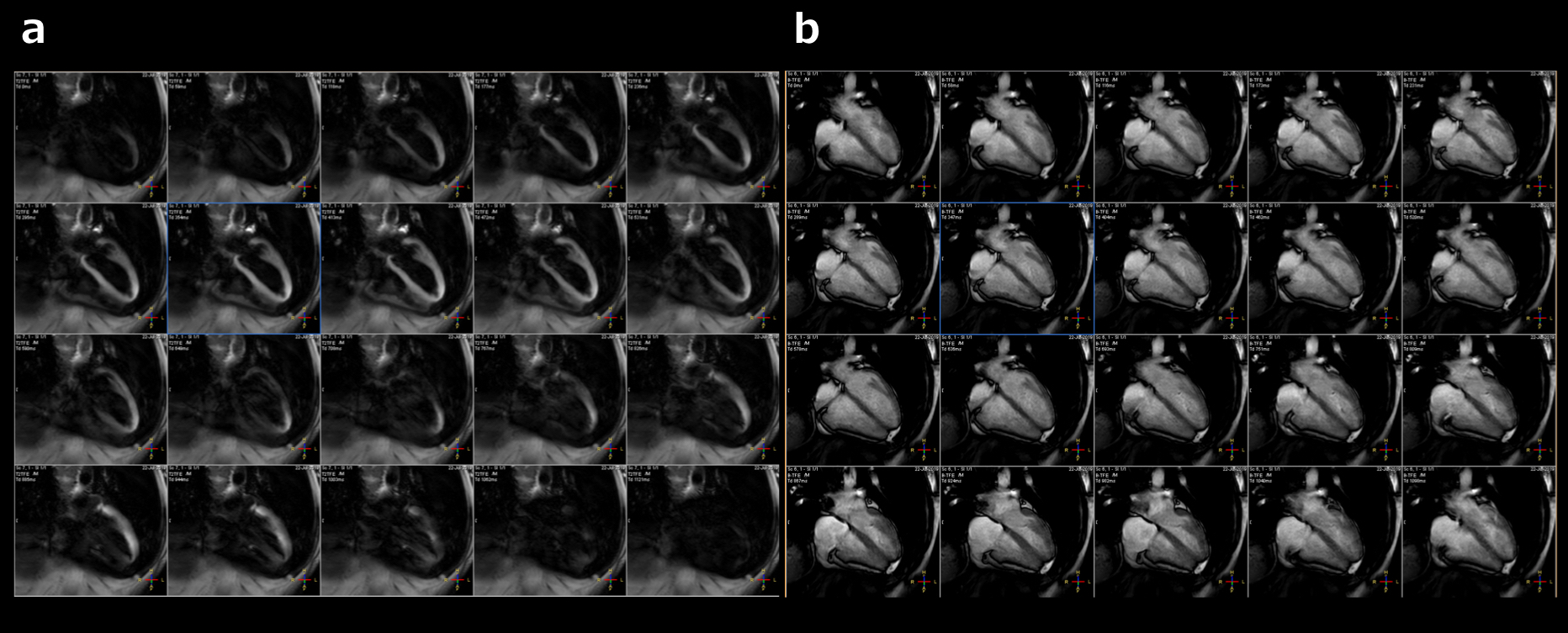
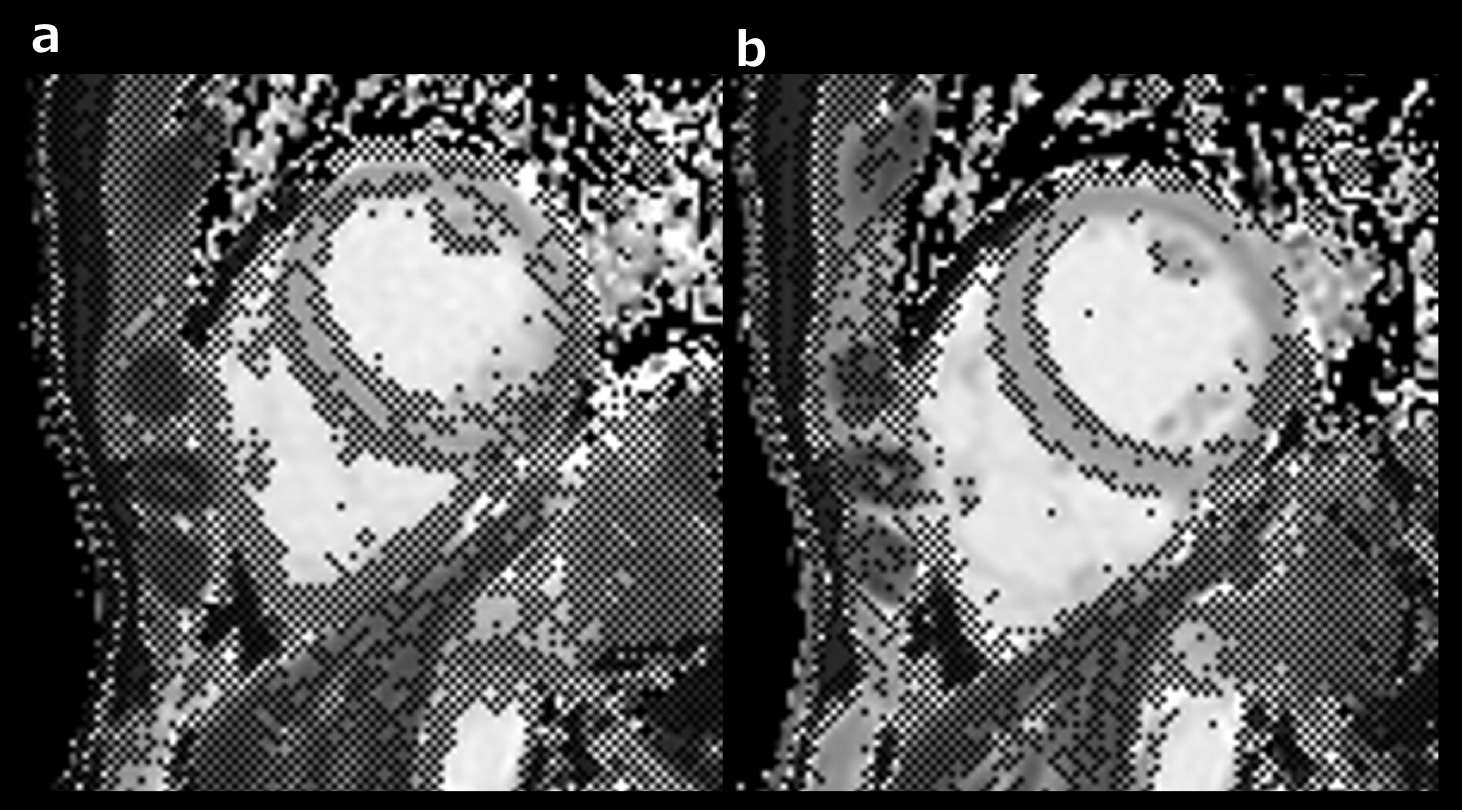
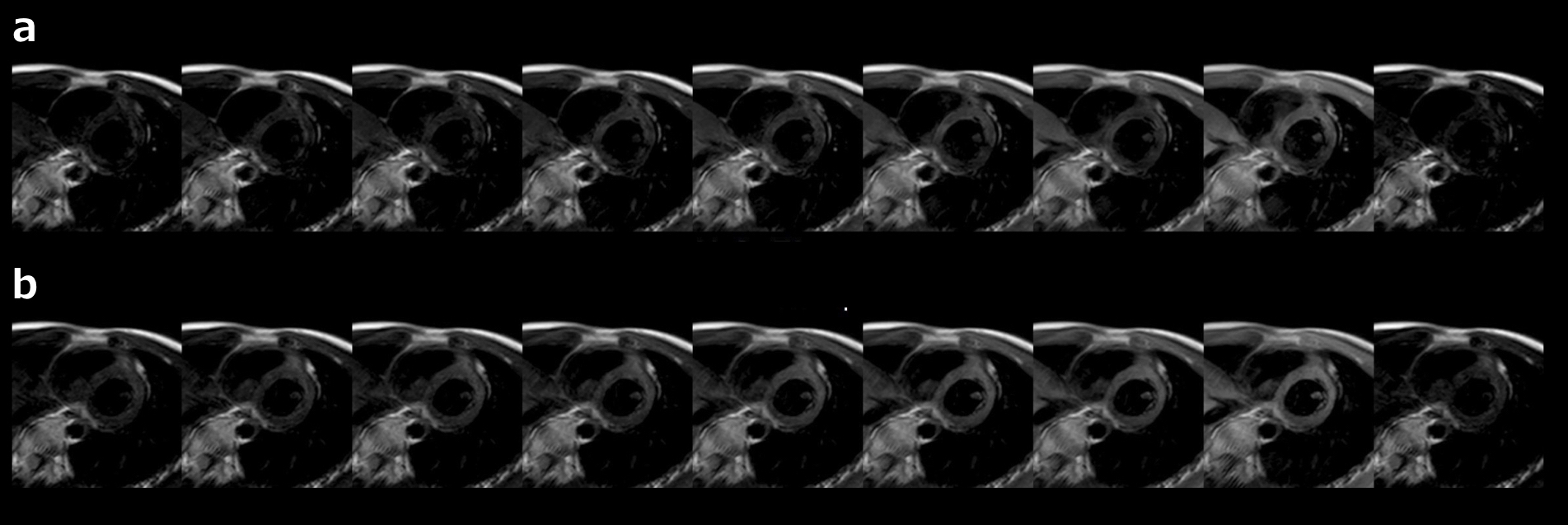
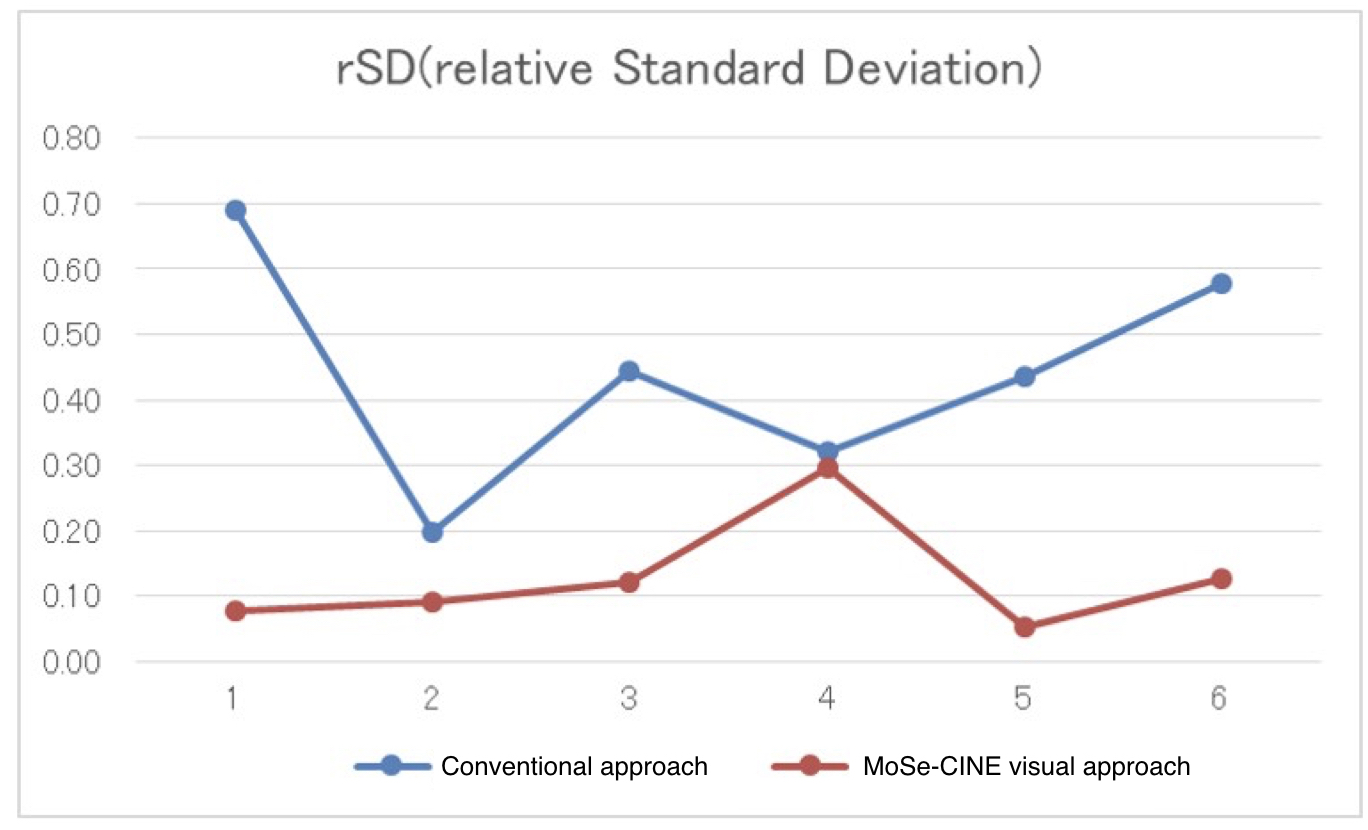
Representative two examples of MoSe-CINE images and conventional bSSFP CINE images are shown in Figure 1 and 2. bSSFP CINE clearly showed cardiac morphology changes. In contrast to bSSFP CINE imaging, MoSe-CINE images showed not actual morphology changes but it depicted signal decrease due to cardiac motion and it pointed out when is the best timing to trigger for both systole and diastole, to prevent signal loss and/or motion artifacts effectively. Compared with the conventional approach, MoSe-CINE approach clearly depict the “heart freeze” timing and the operator was easily able to determine the exact TD for the quantitative mapping.Figure 3 and 4 shows the examples of comparison between conventional and MoSE-CINE visual approach. In Figure 3, MoSE-CINE visual approach clearly improved the accuracy on T1 confidence map. On the other hand, in Figure 4, MoSE-CINE visual approach improved the image quality of T2map across the all slices. MoSe-CINE approach indicated lower rSD for 16-segment ROIs on the T1map [Fig.5], which reflects improved image uniformity, compared with conventional approach. This suggests that MoSe-CINE imaging could be helpful to increase the robustness by exact TD selection.
Conclusion
MoSe-CINE imaging, based on T2FFE sequence, could clearly visualize the motion-insensitive cardiac-phase timing (especially, when is the accurate systole or diastole) due to its motion sensitivity. Confirming the MoSe-CINE imaging in addition to conventional bSSFP CINE imaging could be useful to determine accurate TD setting which leads to increase the robustness of image quality in quantitative myocardial mapping and other imaging such as T2-weighted imaging and diffusion-weighted imaging.Acknowledgements
No acknowledgements found.References
1. Hamlin SA, et.al. Mapping the future of cardiac MR imaging: case-based review of T1 and T2 mapping techniques. Radiographics. 2014 Oct; 34(6):1594-611.
2. Scott AD,et al. Motion in cardiovascular MR imaging Radiology. 2009 Feb; 250(2):331-51.
3. van Heeswijk RB,et.al. Motion compensation strategies in magnetic resonance imaging. Crit Rev Biomed Eng. 2012; 40(2):99-119.
4. Chavhan GB, Babyn PS, Jankharia BG, Cheng HL, Shroff MM. Steady-state MR imaging sequences: physics, classification, and clinical applications. RadioGraphics. 2008;28:1147–60.
5. Zur Y, Wood ML, Neuringer LJ. Motion-insensitive, steady-state free precession imaging. Magn Reson Med. 1990;16:444–59.
6. Yoneyama M, et al: Reevaluation of T2-weighted fast field echo (T2FFE): application to rapid volumetric black-blood imaging. Radiol Phys Technol 6: 305-12, 2013.
7. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation,105:539-42,2002.
Figures