2026
Motivation and Feasibility for Low Field Imaging of Stroke1Medical Imaging Research Center,Dayananda Sagar College of Engineering, Bangalore, India, 2Dept. of Electronics and Communication, BMS Institute of Technology and Management, Bangalore, India, 3Institute for Systems and Robotics /Department of Bioengineering, Instituto Superior Técnico, Universidade de Lisboa, Lisbon, Portugal, Lisbon, Portugal, 4Dept. of Radiology, Columbia University Medical Center, New York, NY, Newyork, NY, United States
Synopsis
Stroke is one of the major reasons for death and disability globally. The abstract aims to review stroke imaging in geographies with limited access to scanners, particularly North Eastern India and the interior regions of Portugal. The critical operating window of treatment to reverse the damage is of few hours. Neuroimaging plays a significant role in diagnosis and treatment of stroke. It is necessary to explore accessible methods to deliver point of care MR stroke services in such regions. The current work includes stroke incidence, disability adjusted life years, scanner density and feasibility of low field MRI for stroke.
Role of neuroimaging and ischemic stroke therapy
Neuroimaging plays prominent role in stroke to identify the type of the strokes, finding the location and size of the clots, delineating the presence and extent of the ischemic core and penumbra. Ischemic stroke is more commonly treated with recombinant tissue plasminogen activator (rtPA)1. This drug dissolves intravascular clots and reestablishes normal blood supply to cerebral tissue. This can only be administered up to 3-4.5 hours after the onset of stroke symptoms, else it can cause additional brain damage. Diffusion Weighted MRI is recommended as gold standard for acute stroke imaging. This feasibility review is aimed to exploring accessible methods to deliver critical MR stroke services to North Eastern India and interior parts of Portugal.Stroke Incidence and prevalence
A stroke study in 2015 in India revealed the annual incidence of stroke is 105 to 152 per 100,000 people, while annual prevalence reaches up to 559 per 100,000 people2. But developed countries on a global level have a much lower incidence rate (61-111 per 100,000 population) and higher prevalence rate (1,015-1,184 per 100,000 population)2. Portugal witnessed annual stroke incidence of 75.4 per 100,000 people and prevalence rate of 423.9 per 100,000 population in 20172.Accessibility of MR imaging for stroke
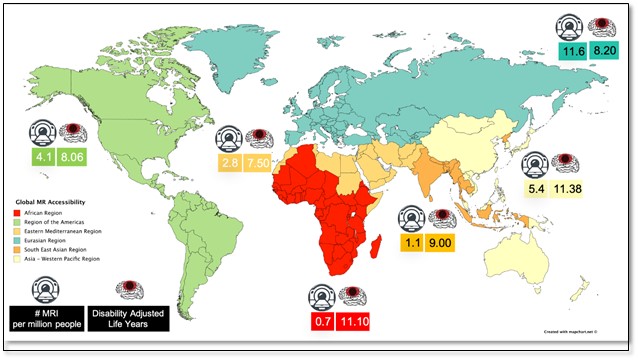
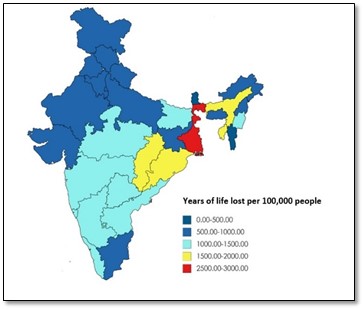
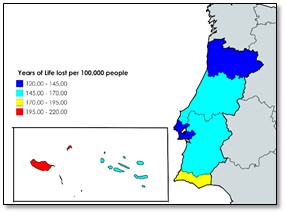
World Health Organization (WHO) reported 90% of the world does not have access to MRI in 20083.Recent global MR scanner density data, DALYs rate across six geographical regions based on the WHO classification is collated and shown in figure 1. Portugal has good scanner density at coastal areas. But poor access of scanners in hilly regions. India has less than 1 scanner pmp3. The DALYs rate for stroke in India and Portugal is captured in figure 2 and 3.Utility of low field regimes in MR imaging
Low field scanners offer an opportunity to deliver the scanner to the patient as a point-of-care device3. Low field scanners offer flexibility in designing open bore MR system. Intraoperative assistance and permit quick access for interventions such as anesthesia or intravenous thrombolysis in case of stroke with such systems4. MR systems at ULF (<10mT) allows imaging in the presence of metal and offer better T1 contrast. Very low field (VLF) (10-100mT) are compatible with MagnetoEncephaloGraphy (MEG) and Neodymium Iron Boron (NdFeB) to produce required magnetic field3,4,5. MR systems at ULF and VLF suffer from thermal drifts, deprived SNR, and safety challenges due to their operations in unshielded environments. MR scanners at low field (LF)(0.2-0.5T) offer better SNR and are commercially available systems4,5. They have also been used for stroke imaging.Low field stroke imaging
Diffusion imaging has an increased dependence on strong gradients than the field strength alone (accounting for concomitant fields) and thus can be performed at low field. Hence, the gradient coils play key role in the low field systems. Tamura et. al. showed that ADC is independent of field strength and comparable across different vendor machines, with fixed acquisition parameters and strong gradients6. The line scan diffusion imaging sequence7 was implemented on 0.5T and l.5T Signa, GE Systems with a maximum gradient strength of 10mT/m. With 108 scans obtained, line scan diffusion imaging provided virtually artefact-free, independent of slice location and orientation, and rapid localization of stroke. The total acquisition time for 14 slices with 7mm thickness was 8 minutes at 0.5 T and 7 minutes at 1.5 T. Forty acute stroke patients were retrospectively examined on a Gyroscan ACS-NT Philips 1.5T system (diffusion-weighted single shot spin echo EPI) and AIRIS II Hitachi Medical Co. 0.3T open MR scanner 8. The mean acquisition time at 0.3T was 210 seconds in comparison with 23.4 seconds at 1.5T. The 0.3T DW-MR images detected 92% of infarcts detected by 1.5T. Fast Field-Cycling (FFC) MRI has been used to identify ischemic stroke at ULF9. Nine sub-acute stroke patients were examined at 0.2mT-0.2T. T1 weighted FFC-MRI images demonstrated hyper-intense regions, with increase in contrast and decreasing field strength, achieving maximum contrast at 0.2 mT. A portable, open design and point-of-care MRI scanner by Hyperfine can operate without trained technicians and does not require a hospital set up for deployment10.Conclusion
Figure 1 collates MR scanner density and DALYs rate across six geographical regions based on the WHO classification, African and South East Asia are with lesser scanner density and higher DALYs rate. Figure 2 and 3 depicts DALYs rate in India and Portugal. The states with the highest rate of stroke DALYs were West Bengal and Odisha in the east, Tripura and Assam in the northeast, and Chhattisgarh in central India. DALYs rate for stroke significantly more and almost three times higher than the national average. It is clear that remote and hilly regions are witnessing more death and disability in both the countries. Utility of low field regimes in stroke imaging is discussed in the study. Irrespective of limitations at low field strength, many commercially available systems proved to be good for stroke imaging. Recently, research interest in low field MR has been resurrected through significant advances in MR subsystem hardware, acquisition and reconstruction methods and image analysis. This allows the larger low field community to research and develop new methods and systems at low field.Acknowledgements
This work was supported by Department of Science and Technology under an Indo-Portugal Grant, Development of low field MRI scanner for stroke imaging, Int/Portugal/P-09 /2017 and Fundação para a Ciência e a TecnologiaReferences
1. Miller, Daniel J., Jennifer R. Simpson, and Brian Silver. "Safety of thrombolysis in acute ischemic stroke: a review of complications, risk factors, and newer technologies." The Neurohospitalist 1, no. 3 (2011): 138-147.
2. Katan M, Luft A. Global burden of stroke. InSeminars in neurology 2018 Apr (Vol. 38, No. 02, pp. 208-211). Thieme Medical Publishers
3. Geethanath S et al., Accessible magnetic resonance imaging: A review. Journal of Magnetic Resonance Imaging. 2019
4. Wald, Lawrence L., Patrick C. McDaniel, Thomas Witzel, Jason P. Stockmann, and Clarissa Zimmerman Cooley. "Low‐cost and portable MRI." Journal of Magnetic Resonance Imaging (2019).
5. Kraus R Jr, Espy M, Magnelind P, Volegov P. Ultra-low field nuclear magnetic resonance: A new MRI regime. Oxford, UK: Oxford University Press; 2014.
6. Ogura A, Tamura T, Ozaki M, Doi T, Fujimoto K, Miyati T, Ito Y, Maeda F, Tarewaki H, Takahashi M. Apparent diffusion coefficient value is not dependent on magnetic resonance systems and field strength under fixed imaging parameters in brain. Journal of computer assisted tomography. 2015 Sep 1; 39 (5):760-5.
7. Maier S, Gudbjartsson H, Patz S, Hsu L, Lovblad KO, Edelman RR, Warach S, Jolesz FA. Line scan diffusion imaging: characterization in healthy subjects and stroke patients. AJR. American journal of roentgenology. 1998 Jul; 171(1):85-93.
8. Terada H, Gomi T, Harada H, Chiba T, Nakamura T, Iwabuchi S, Nemoto H, Kawasaki S, Watanabe S, Nagamoto M, Kawawa Y. Development of diffusion-weighted image using a 0.3 T open MRI. Journal of neuroradiology. 2006 Feb 1;33(1):57-61.
9. Fast field cycling MRI for ischemic stroke at ultra low field magnetic strength https://www.abdn.ac.uk/research/ffc-mri/.../abstract_MacLeod_BCISMRM_2018.pdf
10. Hyperfine, https://www.hyperfine.io/
Figures