2007
7T resting state connectivity applied to HIFU procedures for planning and efficacy
Stephen Jones1, Jessica Cooperrider1, Daniel Lockwood1, Sean Nagel1, Emmanuel Obusez1, Richard Rammo1, Paul Ruggieri1, Andre Machado1, and Mark Lowe1
1Cleveland Clinic, Cleveland, OH, United States
1Cleveland Clinic, Cleveland, OH, United States
Synopsis
High Intensity Focused Ultrasound (HIFU) in now entering clinical practice, for example to treat essential tremor by causing small lesions in the thalamus. Due to small size of treatment lesions, treatment success depends critically on targeting, which is classically done using measurments and landmarks. We explore an alternative method using functional imaging to guide targeting, specifically using 7T resting state connectivity. We present preliminary data of the patterns of connectivity possible with 7T using a concatenated series of healthy subjects. Finally, we show the changes in connectivity in a post-HIFU patient from the thalamus to the cortex.
Background
High Intensity Focused Ultrasound (HIFU) is a new treatment for essential tremor (ET) using an MR guided array of 1024 transducers transmitting extracranial ultrasound at 650 kHz to a focal spot to thermally ablate the ventral intermediate nucleus of the thalamus (ViM). The size of the thermal cavity is a sphere about 6 mm in diameter, while the size ViM is slightly larger, around 5x7 mm. If the HIFU lesion is misaligned to extend into adjacent thalamic nuclei, unwanted side effects can occur such as ataxia or pain. Currently, positioning is guided by a long experience using brain measurements, which is fairly constant among all adults. Alternative methods use direct targeting using structural imaging to thalamic landmarks. Nevertheless, given the precision possible with the modern HIFU technology, there is great utility in providing a target evidenced by functional imaging, rather than numbers or structure. We propose to use 7T resting state fMRI to address two clinical problems using HIFU: (1) initial targeting of the HIFU lesion; (2) objectively evaluating the effect of a HIFU procedure by computing a functional imaging metric. Currently, the post-HIFU location of the cavity is visualized on structural sequences, and compared with distances to the posterior limb of the internal capsule, but such simple measurements may not reflect variability of functional efficacy and durability of the result. We start approaching this research using a cutting edge dataset of concatenated resting state data at 7T on normal healthy controls.Methods
Before studying individual 7T resting state connectivity to ViM, general patterns of connectivity are studied using a special dataset comprising 19 NHC scanned in a resting state protocol on a Siemens Magnetom 7T, using 132 repetitions of 81-1.5mm thick slices acquired using simultaneous multi-slice GE-EPI: TE/TR=19ms/2800 ms, 128x128 matrix, MB=3, Grappa=2, 1.2mm x 1.2mm resolution. The subject were scanned with eyes closed and refraining from voluntary motion. Data analysis started with physiologic noise removal, retrospective motion correction, and temporal filtering (lowpass < 0.1Hz). No spatial filtering was applied. Concatenation: Individual T1w images were aligned to EPI scan using linear registration, thereafter transformed to the MNI template using a non-linear transformation with ANTS. Each time point of the EPI was then registered to MNI space using the transformation matrix from the T1w registration. Data was detrended using a third order polynomial. Finally, all studies were concatenated using AFNI’s 3dTcat. Functional Connectivity Analysis: Connectivity was measured two ways: from larger ROIs in the sensorimotor cortex to the thalamus; and from single voxels in the thalamus to the sensorimotor cortex. All calculations used Instacorr from the AFNI. In the former method, ROIs 5 mm in diameter were placed in anatomic regions associated with face, hand, and leg areas. In the latter method, a rectangular grid of seed points in an axial plane through the thalamus were explored, systematically computing the temporal correlation coefficient to all voxels in the sensorimotor cortex (as defined by using a coregistered FreeSurfer cortical segmentation). We hypothesize that the region of highest connectivity -colocalized with ViM. To evaluate clinical efficacy of a HIFU treatment, we acquire 7T rsfMRI in patients after HIFU, and example alterations in connectivity from the thalamus to remaining cortex. To date, 3 patient have been scanned at 7T between 1 to 7 months after a clinically successful HIFU procedure, with each procedure causing a unilateral lesion in the region of ViM.Results
(1) Resting state connectivity maps from three seeds in the left sensorimotor cortex to the thalamus are shown in Fig. 1, specifically from the face, hand, and leg areas, showing connectivity asymmetrically stronger to the left thalamus, in the region of the ViM. While the face and arm regions nearly overlap, the leg region is slightly posterior-lateral, as is known in clinical practice. (2) Voxel-wise resting state fMRI connectivity maps from an entire axial plane in the thalamus to the entire sensorimotor cortex show regions of increased connectivity that are proximal to expected location of ViM. Figure 2 shows one example in a plane 1mm above the AC-PC, with the region of highest connectivity involving portions portions of ViM. This technique can also be applied to other deep nuclei, such as the dentate, which is shown in Figure 3. (3) Figure 4 shows two post-HIFU connectivity maps in one patient, with the seed being in either the HIFU cavity itself, or in the contralateral thalamus at the presumed location of the ViM. In both cases there is connectivity from the thalamus to the sensorimotor cortex, and supplementary motors regions in the medial frontal convexities. This connectivity is reduced with the seed is the HIFU lesion, versus the seed in contralateral ViM. .Conclusion
7T resting state provides a promising technique to help identify the regions of the thalamus with highest connectivity to the cortex. Such maps can help guide targeting based on functional activity. Secondly, 7T resting state can potentially be an imaging biomarker of efficacy of a HIFU treatment.Acknowledgements
No acknowledgement found.References
No reference found.Figures
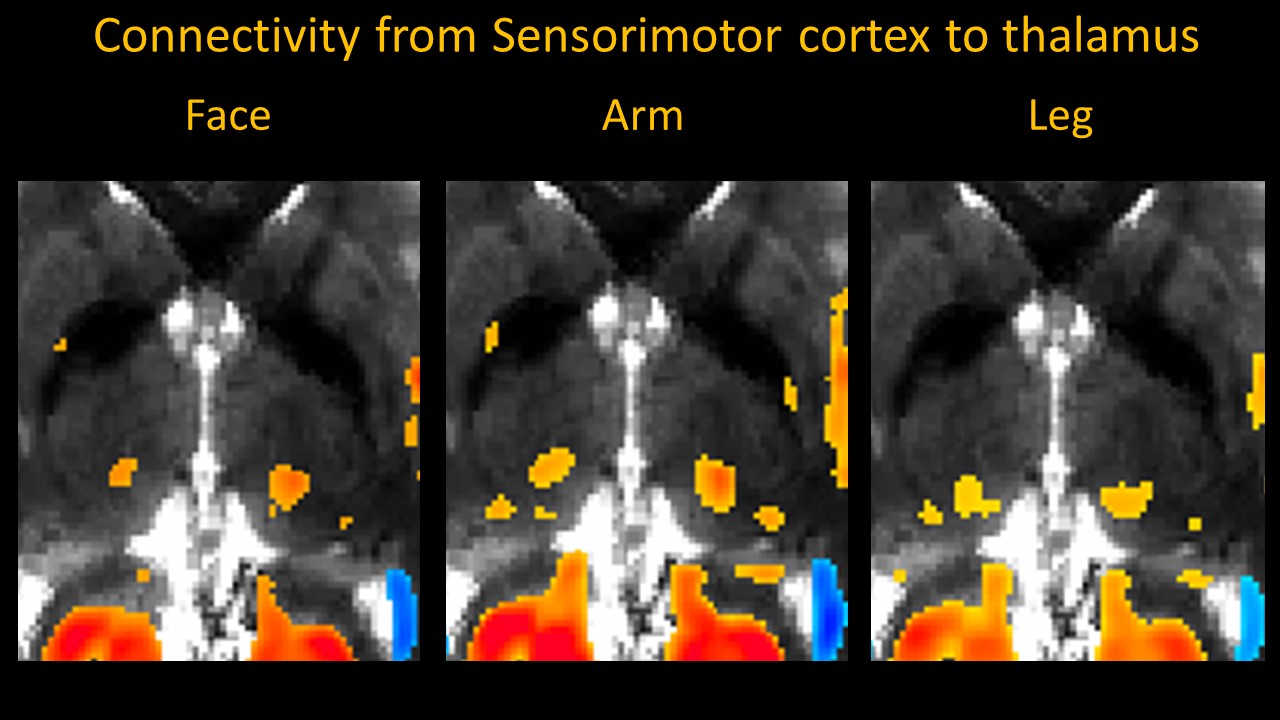
Figure 1: 7T resting-state connectivity from 3 ROIs in the left sensorimotor strip to an axial plane in the thalamus at the level of ViM (+1 mm in MNI coordinates). The three panels correspond to different seeds in the expected regions of the face, hand, and leg motor regions (seed diameter 4 mm). The face and arm/hand regions co-localize, as expected from clinical experience, while the leg region is more posterior-lateral. While there is bilateral connectivity, it is strongest in the ipsilateral thalamus.
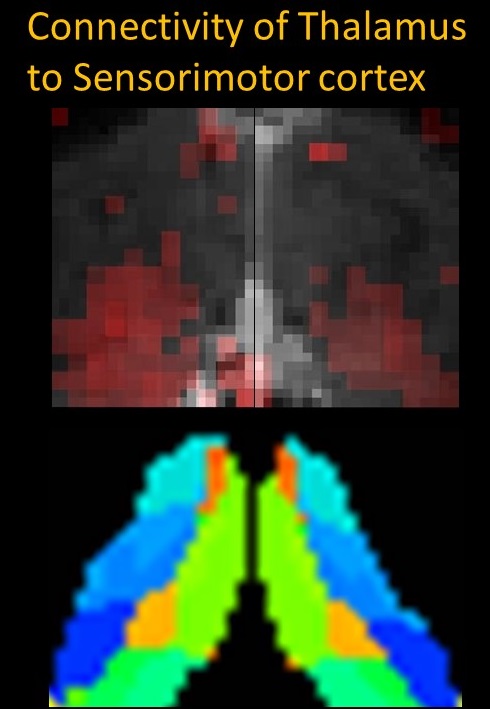
Figure 2: Top: map of voxel-wise 7T resting-state connectivity from an axial plane in the thalamus containing ViM to the entire bilateral sensorimotor strip Significant voxels are shown with a red overlay. Bottom: corresponding image of thalamic parcellations derived from FreeSurfer, which confirms the co-localization of highest activation to ViM.

Figure 3: Similar to Fig. 2, a map of voxel-wise 7T resting-state connectivity to sensorimotor strip, from an axial plane including both dentate nuclei. Top: 7T EPI anatomic image showing the dentate nuclei outlined by dashed green lines. Bottom: corresponding connectivity maps with significant voxels overlaid in red. Note that a majority of the right dentate shows significant connectivity to the both sensorimotor cortex, which is asymmetrically stronger than the left dentate. Portions of the vermis (posterior midline) also show strong connectivity.
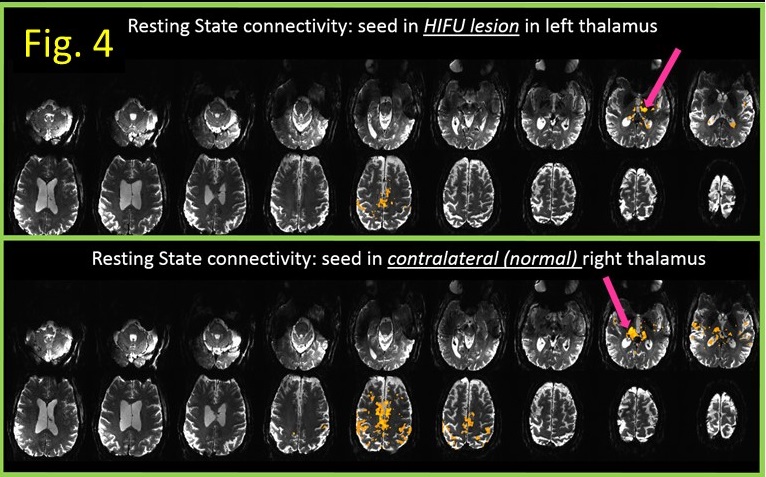
Figure 4: Two 7T resting-state connectivity maps from one patient after a HIFU ablation of left ViM. Top: seed in left thalamic HIFU cavity itself; Bottom: seed in the contralateral (left) thalamus in the presumed location of ViM. In both cases there is connectivity from
the thalamus to the sensorimotor cortex, and supplementary motors regions in
the medial frontal convexities. This connectivity is reduced with the seed is
the HIFU lesion, versus the seed in contralateral ViM.