1920
Human Mesenchymal Stem Cell Donor Effects on Apparent Diffusion Coefficient in a Rodent Stroke Model at 21.1 T
F. Andrew Bagdasarian1,2, Shannon Helsper1,2, Xuegang Yuan1,2, Jens T. Rosenberg1, and Samuel Colles Grant1,2
1National High Magnetic Field Laboratory, Florida State University, Tallahassee, FL, United States, 2Chemical & Biomedical Engineering, FAMU-FSU College of Engineering, Tallahassee, FL, United States
1National High Magnetic Field Laboratory, Florida State University, Tallahassee, FL, United States, 2Chemical & Biomedical Engineering, FAMU-FSU College of Engineering, Tallahassee, FL, United States
Synopsis
This study extends diffusion weighted imaging at 21.1-T to identify the pattern of potential recovery of apparent diffusion coefficient (ADC) in rodent ischemic stroke with novel stem cell therapy using dissociated aggregate human mesenchymal stem cells (d-hMSC) from different donors. All scanning was performed at 21.1 T with the goal of quantitatively assessing treatment efficacy longitudinally, spanning a 3 weeks post ischemia. Results show donor resultant ADC discrepancies at various time points and regions.
Introduction
Stroke incidence, a leading cause of death in the United States, is expected to rise with an aging population1. Previous studies have demonstrated therapeutic potential for 2D cultured hMSC for ischemic stroke2, and intracerebral administration of intact 3D hMSC aggregates correlates to a reduced sodium volume over time, highlighting recovery of cellular homeostasis, potentially due to their resistance in ischemic environments3,4. Diffusion-weighted imaging (DWI) provides internal biomarkers, demonstrating pathological evidence for ischemia and quantifying the extent of ischemic penumbra. Previous results have indicated that intra-arterial injection (IA) of d-hMSC showed better improvement when compared to intracerebral ventricular (ICV) injection as verified through DWI5. This study aims to expand on those previous results by utilizing DWI outcomes with high spatial discrimination applied to a rat stroke model to assess the therapeutic efficacy of different donors of aggregated dissociated hMSC (d-hMSC) applied during the sub-acute phase.Methods
Animal and Cell Model: Male Sprague Dawley rats (220-250 g) underwent 1-h transient middle cerebral arterial occlusion (MCAO) followed by immediate IA injection of 1 mill d-hMSC from Donor 1 (n=5), Donor 2 (n=6) or saline as control (n=8). Donors had pre-determined levels of proliferation and senescence based on extended culture assays. Prior to injection, d-hMSC were incubated with 7.47-µg/mL micron-sized particles of iron oxide (MPIO) for 12 h.MR Techniques: Using the 21.1-T ultra-widebore magnet at the US National High Magnetic Field Laboratory and a linear 1H/23Na birdcage coil, high resolution images were acquired at days 1, 3, 7 and 21 post-MCAO/injection. DWI utilized conventional spin echo acquisitions over 4 b values (0-3 ms/mm2) with a slice package centered on the ischemic lesion, resolution=400x400x1500 μm and TE/TR=30/2250 ms. Scan time was 8 min. d-hMSC localization required a standard 2D FLASH sequence: TE/TR=4/1000 ms, resolution=50x50x500 μm, 21 slices and acquisition time of 17 min.
Data Analysis: ADC maps were processed in MATLAB. Resultant maps from day 1-21 were segmented with reflected lesion ROI in the ispi- and contralateral striatal and stroke regions to assess longitudinal changes. Statistical analysis was performed to determine significance longitudinally and between groups for each ROI.
Results
In vitro analysis showed that Donor 2 had lower senescence and higher colony forming units than Donor 1. Successful IA d-hMSC injections were achieved (Fig 1), and retention levels of MPIO-labeled d-hMSC was consistent between groups across all time points. Ischemic lesions were identified in T2W images (Fig 2a).In the striatum ROI, Donor 2 and controls show near-linear increases in ADC through 21 d in the ischemic hemisphere (IH), with Donor 2 having higher values. Group differences were evident at 21 d, with Donor 1 displaying significantly lower ADC compared to other groups and earlier time points. Additional striatal group differences are only observed in the contralateral hemisphere (CH) (Fig 3b) through 7 d. Donor 1 ADC is consistently lower than Donor 2 and control. Donor 2 ADC was on average highest at all time points in both hemispheres.
In the stroke ROI, all groups show near-linear increases in ADC over time, though without significance (Fig 4a). Hemispheric differences in the stroke lesion (Fig 4) follow striatal trends. No group differences were observed in the stroke-IH ROI. In the stroke-CH, Donor 1 ADC was lower consistently than other groups through 21 d (Fig 4b).
Discussion & Conclusion
In the striatal-IH (Fig 3a), Donor 1 has a significantly lower ADC at 21 d than both Donor 2 and control, indicating Donor 1 may not have a long-term neuroregenerative or protective effect. Further, striatal-CH results may show that Donor 1 has a negative impact in non-ischemic tissue, shown by reduced CH ADC. With higher senescence and lower ADC than Donor 2, it is possible that Donor 1 may be amplifying ischemic effects localy and beyond the immediate penumbra, possibly due to a metabolic shift in the implanted cells.In contrast, Donor 2 ADC was significantly higher than both groups in the stroke-CH, illustrating a heightened global response (i.e. paracrine effect) that may protect at-risk and contralateral cerebral tissue. These results display donor source importance, as compromised sources may exacerbate ischemic insult, as well as threaten non-ischemic hemisphere measurements, even when compared to untreated stroke.
In conclusion, ADC outcomes as an internal biomarker for ischemic stroke treatment efficacy as it relates to different hMSC donors shows promise. These results demonstrate that restoration of brain tissue ADC may be highly dependent on the cell source condition, with impacts that propagated beyond the cell impact and initial site of injury. Donor 2 ADC response appears to improve in both the stroke and striatum, while the compromised Donor 1 shows potentially worse long-term response in both hemispheres. These findings highlight the importance of cell source, and the necessity for multi-donor analyses regarding the treatment of stroke.
Acknowledgements
All work has been conducted in accordance with the FSU Animal Care and Use Committee. This work was supported by the NIH (RO1-NS102395). The National High Magnetic Field Laboratory is funded by the NSF (DMR-1644779) and the State of Florida.References
- Benjamin EJ, et al. 2017. AMA, Statistics Committee and Stroke Statistics Subcommittee.
- Wakabayashi K., et al. 2010. JNR. 88:1017-1025.
- Ma T., et al. 2015. Tissue Eng Part A. 21(9-10):1705-1719.
- Ma T., et al. 2014. Tissue Eng Part B Rev. 20(5):365-380.
- Bagdasarian, FA. 2019. Quantitative Assessment of Treatment Efficacy in Acute Ischemia Using Perfusion and Diffusion Weighed Imaging at 21.1 T. ISMRM. E-Poster: 2820.
Figures
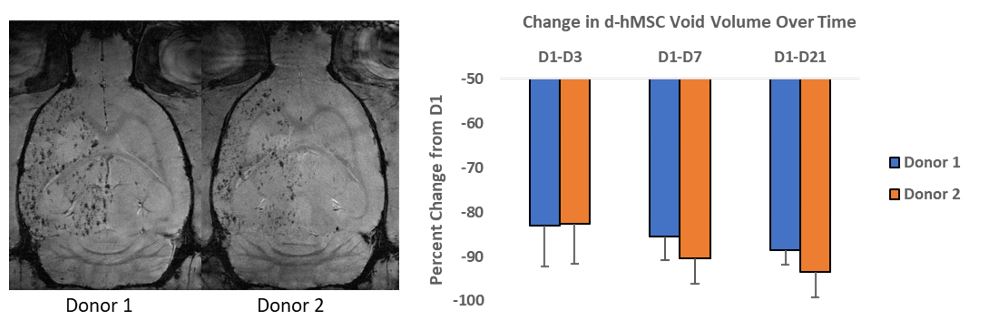
Figure 1. FLASH showing successful injection of MPIO-labeled d-hMSC from Donors 1
and 2 post-MCAO at day 1. Percent decrease in d-hMSC for each group is presented.
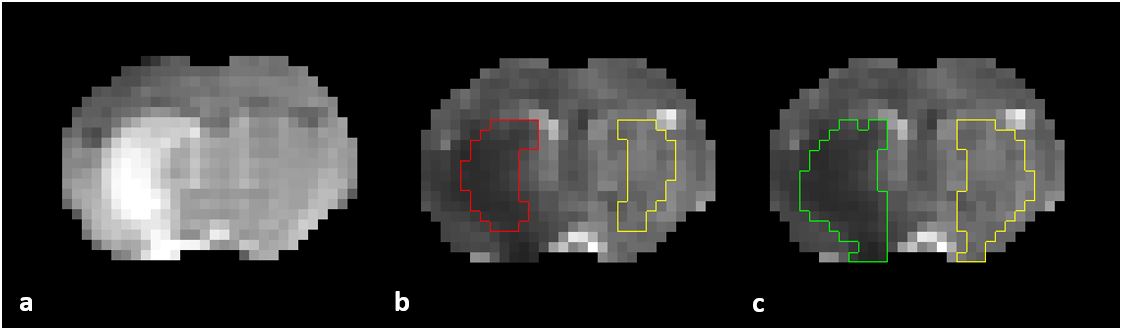
Figure 2. (a) T2W scan showing lesion hyper-intensity, (b) resultant
ADC map with ipsi- (red) and contralateral (yellow) segmentation of striatum, and
(c) ADC map showing ipsilateral stroke ROI (green) and reflected contralateral
ROI (yellow).
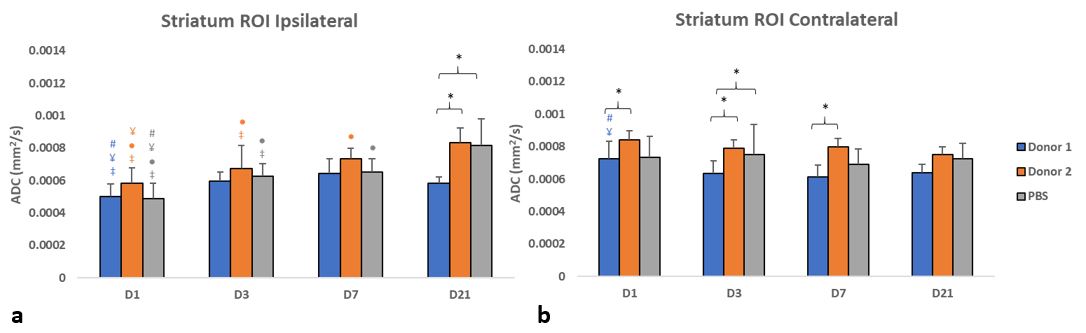
Figure 3. Striatum ROI ADC measurements from Donor 1, 2, and PBS (control) groups at days 1,
3, 7 and 21 after MCAO/injection in the (a) ipsilateral and (b) contralateral hemisphere. ‡ = significant
difference between ipsi- and contralateral measurements within groups on
specified day. # = significant difference from D3, ¥ = significant difference
from D7, ● = significant difference from D21. * = significant difference
between groups within same day. p<0.05.
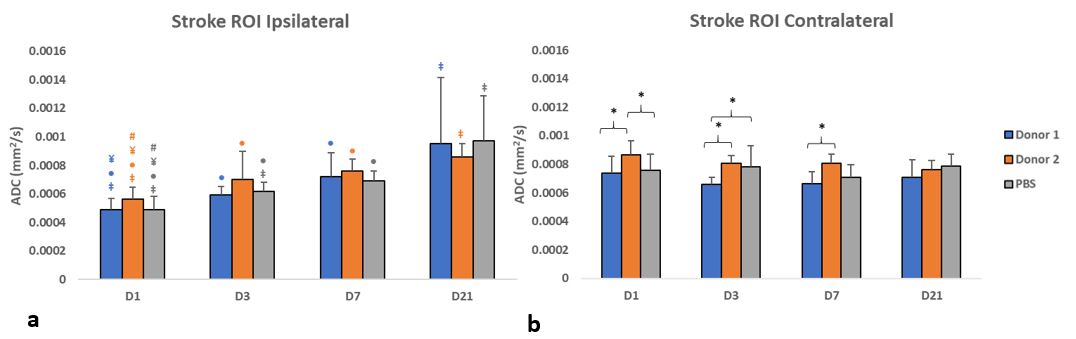
Figure 4. Stroke ROI ADC measurements from Donor 1, 2, and PBS (control) groups at days 1, 3, 7 and 21 after MCAO/injection in the (a) ipsilateral and (b) contralateral hemisphere. ‡ = significant difference between ipsi- and contralateral measurements within groups on specified day. # = significant difference from D3, ¥ = significant difference from D7, ● = significant difference from D21. * = significant difference between groups within same day. p<0.05.