1806
Amide Proton Transfer Brain Imaging with Compressed Sense: Comparison of Different Acceleration Factors and Conventional Parallel Imaging1The First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijing, China
Synopsis
Amide proton transfer (APT) imaging is a novel and promising MRI contrast method, but it can be time-consuming. Common parallel imaging methods, like SENSE, can lead to reduced quality of APT. Here, compressed sensing technique is evaluated for the acceleration of APT in brain. The purpose of the present study is to explore feasibility of different acceleration factors in brain APT. The results show that it is feasible to apply accelerator factor 5 to APT display of brain tissue and brain tumor, which could reduce the scan time with in 1 min.
Introduction
Amide proton transfer (APT) imaging, a variant of the CEST‐based molecular MRI technique, is based on the chemical exchange between free bulk water protons and the amide protons(‐NH) of endogenous mobile proteins and peptides in tissue. [1, 2] The early clinical applications of APT are very promising, but have been limited primarily because of the long scan time required. The application of compressed sensing (CS) technology solves this problem [3, 4], but whether different accelerators have effects on APT remains to be further explored. The aim of the current study was to compare SENSE with compressed sensing for brain APT, including the evaluation of a number of different acceleration factors.Methods
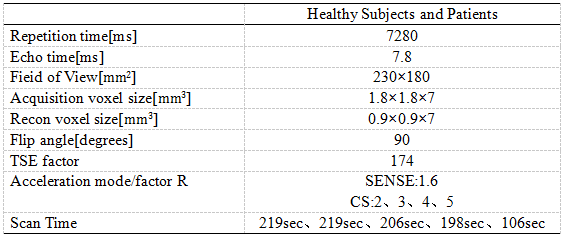
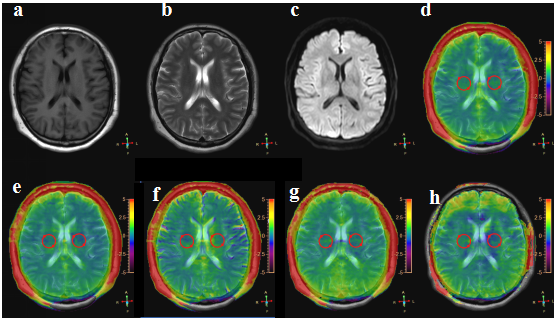
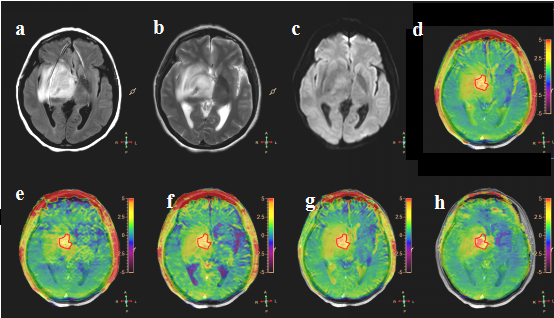
CS-accelerated APT images were performed on a 3T whole‐body human scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands) using a body coil for RF transmit and a 32‐channel head coil in our hospital in 11 healthy volunteers (26.64±7.79, range: 23-37years, 5 women) and 6 brain tumor patients (44.00±19.65, range:11-64 years ,3 women). For the APT imaging, compressed sensing acceleration factor (AF) of 2, 3, 4 and 5 was compared with conventional SENSE 1.6. The other scan parameters were shown in Table 1. The APTW images were transfer to the Philips IntelliSpace Portal for the APT value measurement. Two ROIs(200±10mm2) were placed symmetrical on the left and right sides around the lateral ventricle of healthy volunteers for APT measurement (Figure 1). In addition, the ROI was placed according to the edge of the tumor in patients based on the APT and T2WI FLAIR Imaging fusion image. (Figure 2). The independent samples Kruskal-Wallis test was used to identify APT values under different AF in healthy volunteers and brain tumor patients.Results
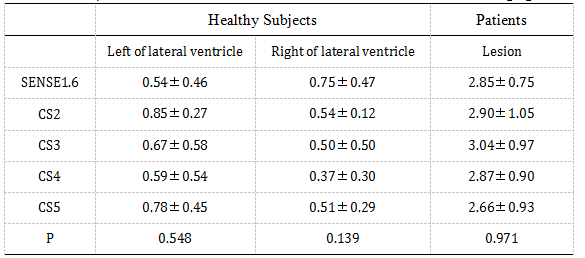
The APT signals obtained from the CS with AF of 2、3、4、5 were well‐preserved as compared with the reference image (SENSE = 1.6) both in brain tumor and healthy volunteer studies. There was no significant APT difference between the CS-accelerated images and the reference image both in healthy volunteers and brain tumor patients.(P=0.793,P=0.971).(Table 2) The scan time of CS-accelerated APT imaging was dramatically reduced to 59.3 S (CS5)as compared to SENSE1.6 (3:39minutes)Discussion and Conclusion
In the current study, brain APT imaging using CS was superior to that using SENSE. In comparison with the original sequence, CS may be a reliable method for APT with comparable image quality and quantitative values. According to our result, the acceleration factor 4 for Compressed Sense technique was recommended in future study, saving at least 70% time compared to the SENSE acceleration. Compressed sensing acceleration could successfully extended to APT imaging without compromising image quality and quantification. The CS based APT imaging can easily be integrated into clinical protocols and would be beneficial for a wide range of applications.Acknowledgements
No acknowledgement found.References
[1] Zhou J, Heo HY, Knutsson L, van Zijl P, Jiang S. APT‐weighted MRI: techniques, current neuro applications, and challenging issues. Magn Reson Imaging. 2019,50(2):347-364.
[2] By S, Barry RL, Smith AK, et al. Amide proton transfer CEST of the cervical spinal cord in multiple sclerosis patients at 3T. Magn Reson Med. 2018;79:806–814.
[3]Bratke G, et al. Accelerated MRI of the Lumbar Spine Using Compressed Sensing: Quality and Efficiency. Magn Reson Imaging 2018; 49: e164-e175.
[4]Vu KN, Gilbert G, Chalut M, et al. MRI-determined liver proton density fat fraction, with MRS validation: Comparison of regions of interest sampling methods in patients with type 2 diabetes. Magn Reson Imaging, 2016, 43(5): 1090-1099.
Figures