1792
Blood-Brain Barrier Imaging as a Biomarker for Cognitive Decline in Systemic Lupus Erythematosus1Department of Medical Neuroscience, Dalhousie University, Halifax, NS, Canada, 2Department of Diagnostic Radiology, Dalhousie University, Halifax, NS, Canada, 3Biomedical Translational Imaging Centre (BIOTIC), QEII Health Sciences Centre, Halifax, NS, Canada, 4Departments of Psychiatry, Psychology & Neuroscience and Medicine, Dalhousie University, Halifax, NS, Canada, 5Nova Scotia Health Authority, Halifax, NS, Canada, 6Department of Anesthesia, Pain Management and Perioperative Medicine, Dalhousie University, Halifax, NS, Canada, 7Acquired Brain Injury (Epilepsy Program), Nova Scotia Health Authority, Halifax, NS, Canada, 8Department of Physics, Dalhousie University, Halifax, NS, Canada, 9Research Methods Unit, Nova Scotia Health Authority, Halifax, NS, Canada, 10Department of Physiology and Cell Biology, Medicine, Ben-Gurion University of the Negev, Beer Sheva, Israel, 11QEII Health Sciences Center, Halifax, NS, Canada, 12Department of Medicine and Division of Rheumatology, Dalhousie University, Halifax, NS, Canada
Synopsis
This study addresses the need for mechanism-based understanding of cognitive impairment in systemic lupus erythematosus (SLE). Using dynamic contrast-enhanced MRI we identified extensive blood-brain barrier (BBB) leakage in 16 of 46 SLE patients. Extensive BBB leakage was associated with worse overall cognitive performance, affecting primarily information processing speed and executive abilities. Our study provides the first compelling evidence for BBB damage in SLE, and links BBB leakage to cognitive dysfunction. These findings highlight the diagnostic potential of BBB imaging and call for research into BBB-targeting therapies.
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease, in which circulating autoantibodies can target different organs, such as the kidneys, skin, and joints. A major source of morbidity and mortality in SLE are the neuropsychiatric manifestations of the disease, with cognitive decline being the most commonly reported feature.1–3 To date there are no evidence-based biomarkers or treatments for neuropsychiatric SLE (NPSLE), as the etiology of these complications remains poorly understood. Several potentially complementary mechanisms have been thus far implicated in NPSLE, with one central commonality − dysfunction of the brain’s microvasculature, i.e. the blood-brain barrier (BBB).4,5 Dysfunction of the BBB exposes brain cells to blood components that are normally barred from the brain, and can underlie neuropathology even in the absence of SLE autoantibodies. One such example is the neuroinflammatory cascade triggered by the extravasation of serum albumin, leading to neuronal hyperexcitability and neurodegeneration.6–9 In SLE, BBB disruption is also hypothesized to allow the infiltration of autoantibodies into the brain.10 This hypothesis is supported by animal studies demonstrating the existence of autoantibodies that can cause neuronal dysfunction/death and cognitive impairment when injected directly into mouse brains.11,12 Emerging in vitro findings also identify specific SLE autoantibodies, pro-inflammatory cytokines and complement activation proteins that can damage the endothelial cells of the BBB.13,14 However, to date there is no compelling evidence for BBB leakage in SLE patients, and the role of BBB leakage in human manifestations of NPLSE remains unknown.Methods
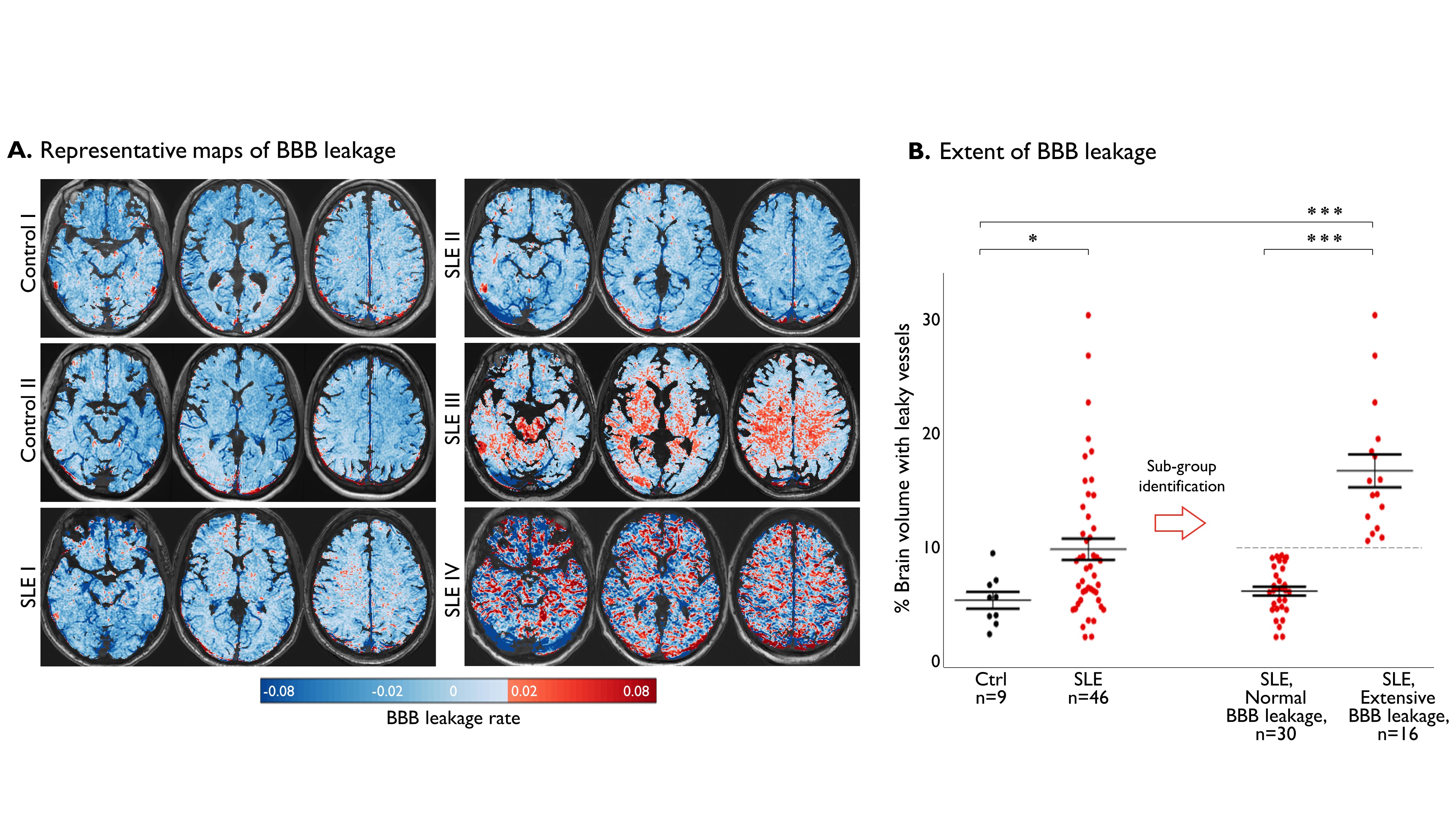
We studied the BBB of 46 SLE patients and 9 controls (matched for sex and age), using dynamic contrast-enhanced MRI. Participants were intravenously injected with the magnetic contrast agent Gadobenate Dimeglumine (0.1 mmol/kg, MultiHance, Bracco Imaging Canada, Montreal, QC), and its dynamics in the brain were monitored for a period of 20 minutes using T1-weighted MRI (3T GE Discovery MR750). MRI analysis was performed as previously described.15–18 In brief, the accumulation rate of the contrast agent during the slow enhancement period of the scan (6-20 min) was derived for each voxel as a measure of BBB leakage. Leakage rates were considered pathological when exceeding 0.02, the 95th percentile of all values in a cohort of control subjects.17 The percent of suprathreshold voxels was used as a measure reflecting overall BBB leakage. To identify sub-levels of BBB leakage, an unsupervised 2-means cluster analysis was performed (partitioning all 55 participants into two distinct clusters). All patients also underwent clinical assessments, blood sampling and psychometric testing of five cognitive domains: information processing speed,19,20 executive abilities,21 attention span, new learning, and delayed recall.22 Raw scores were standardized based on published normative data, and converted to Z-scores.21 Z-scores for each of the five tests were averaged to produce a global cognitive score. The Wilcoxon rank sum test and the Chi square test were used for comparisons of continuous and categorical variables, respectively. The threshold for significance was set at p-value<0.05, and adjusted for multiple comparisons using the false discovery rate method.Results
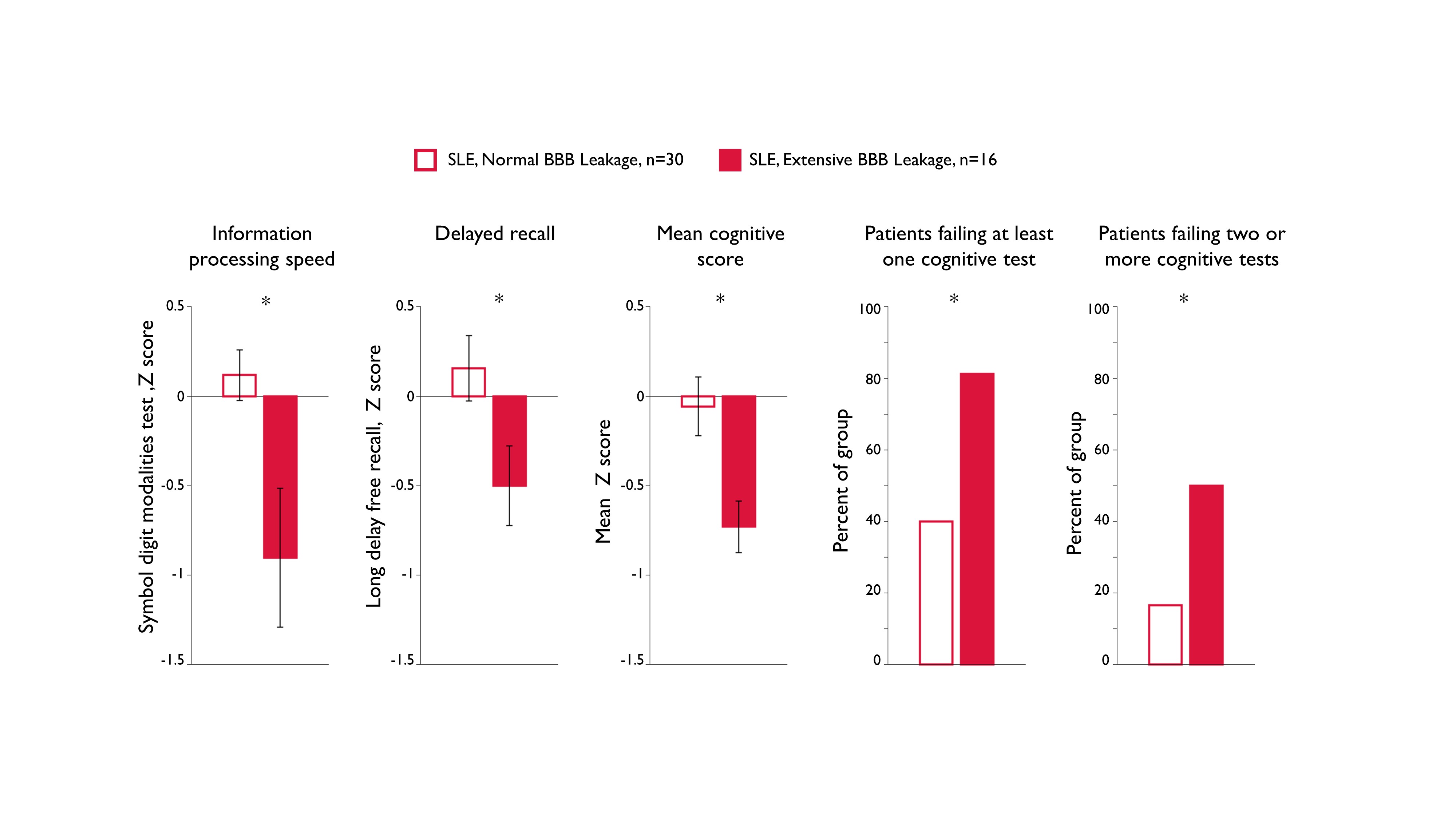
A map of BBB permeability was constructed for each subject (Fig. 1A), with shades of red representing voxels with pathological leakage. Quantification of the percent of brain volume with pathological leakage in each subject revealed significantly higher values in the SLE cohort compared to controls (p<0.05, Fig. 1B left). An exploration of potential BBB-based divisions (using 2-means clustering of all 55 participants) revealed the existence of two distinct clusters, with a threshold of 10.2% separating the groups (p<0.001, Fig. 1B right). The group with the lower mean (5.6%) included all control participants and 30 SLE patients, while the higher mean group (16.5%) consisted of 16 SLE patients exclusively and was labelled the “extensive BBB leakage” group. As there were no differences between the controls and SLE patients within the lower mean group, this group was referred to as “normal BBB leakage”. Comparison of cognitive scores revealed that SLE patients with extensive BBB leakage performed significantly worse on tests of information processing speed and executive abilities (p<0.05, Fig 2). Patients with extensive leakage also scored lower on the global cognitive measure, with 81% failing at least one cognitive test and 50% failing two or more (compared to 50% and 16% of the “normal BBB leakage” group, respectively).Discussion
Our study is the first to provide direct evidence of extensive BBB leakage in a sub-group of SLE patients, and to show an association between BBB leakage and cognitive impairment. We propose that BBB leakage may alter the functionality of affected brain regions, leading to region-associated symptomatology.Conclusion
Our findings highlight the potential role of BBB dysfunction in the development of cognitive impairment in SLE, and call for future studies into BBB-targeting treatments. We suggest that BBB imaging may serve as a mechanism-based biomarker for NPSLE, and as a tool for monitoring disease progression and response to treatment. Future large-scale prospective studies are warranted to determine the association between distinct NPSLE manifestations and region-specific BBB leakage.Acknowledgements
This study was supported by the Canadian Institutes of Health Research (CIHR: PJT 159703), Nova Scotia Health Authority research fund (NSHA RF), Brain Canada (Platform Support Grant), and MITACS. The funders of the study had no role in study design, patient recruitment, data collection, analysis, interpretation or publication.References
1. Ahn, G. Y. et al. Prevalence , risk factors , and impact on mortality of neuropsychiatric lupus : a prospective , single-center study. 1338–1347 (2018). doi:10.1177/0961203318772021
2. Hanly, J. G. Diagnosis and management of neuropsychiatric SLE. Nat. Publ. Gr. 10, 338–347 (2014).
3. Meszaros, Z. S., Perl, A. & Faraone, S. V. Psychiatric Symptoms in Systemic Lupus Erythematosus : 993–1001 (2012). doi:10.4088/JCP.11r07425
4. Stock, A. D., Wen, J. & Putterman, C. Neuropsychiatric lupus , the blood brain barrier , and the TWEAK / Fn14 pathway. 4, 1–9 (2013).
5. Abbott, N., Mendonca, L. & Dolman, D. The blood – brain barrier in systemic lupus erythematosus. 908–915 (2003).
6. Bar-Klein, G. et al. Losartan prevents acquired epilepsy via TGF-β signaling suppression. Ann. Neurol. 75, 864–75 (2014).
7. Weissberg, I. et al. Albumin induces excitatory synaptogenesis through astrocytic TGF-β/ALK5 signaling in a model of acquired epilepsy following blood-brain barrier dysfunction. Neurobiol. Dis. 78, (2015).
8. David, Y. et al. Astrocytic dysfunction in epileptogenesis: consequence of altered potassium and glutamate homeostasis? J. Neurosci. 29, 10588–99 (2009).
9. Cacheaux, L. P. et al. Transcriptome profiling reveals TGF-beta signaling involvement in epileptogenesis. J. Neurosci. 29, 8927–35 (2009).
10. Mader, S., Brimberg, L. & Diamond, B. The Role of Brain-Reactive Autoantibodies in Brain Pathology and Cognitive Impairment. 8, (2017).
11. Kowal, C. et al. Human lupus autoantibodies against NMDA receptors mediate cognitive impairment. (2006).
12. Bravo-zehnder, M. et al. Anti – Ribosomal P Protein Autoantibodies From Patients With Neuropsychiatric Lupus Impair Memory in Mice. 67, 204–214 (2015).
13. Yoshio, T., Okamoto, H., Hirohata, S. & Minota, S. IgG Anti – NR2 Glutamate Receptor Autoantibodies From Patients With Systemic Lupus Erythematosus Activate Endothelial Cells. 65, 457–463 (2013).
14. Mahajan, S. D. et al. C5a alters blood – brain barrier integrity in a human in vitro model of systemic lupus erythematosus. 130–143 (2015). doi:10.1111/imm.12489
15. Veksler, R., Shelef, I. & Friedman, A. Blood-brain barrier imaging in human neuropathologies. Arch. Med. Res. 45, 646–652 (2014).
16. Chassidim, Y. et al. Quantitative imaging assessment of blood-brain barrier permeability in humans. Fluids Barriers CNS 10, 9 (2013).
17. Weissberg, I. et al. Imaging blood-brain barrier dysfunction in football players. JAMA Neurol. 71, (2014).
18. Kamintsky, L. et al. Blood-brain barrier imaging as a potential biomarker for bipolar disorder progression. NeuroImage Clin. 102049 (2019). doi:10.1016/j.nicl.2019.102049
19. Smith, A. Symbol Digit Modalities Test. 9th ed: Western Psychological Services. (2002).
20. Berrigan, L. I. et al. Reliability of regression-based normative data for the oral symbol digit modalities test: An evaluation of demographic influences, construct validity, and impairment classification rates in multiple sclerosis samples. Clin. Neuropsychol. (2014). doi:10.1080/13854046.2013.871337
21. Walker, L. A. S. et al. Canadian Normative Data for Minimal Assessment of Cognitive Function in Multiple Sclerosis. Can. J. Neurol. Sci. 44, 547–555 (2017).
22. Delis, D. C., Kramer, J. H., Kaplan, E. & Ober, B. A. California Verbal Learning Test – second edition. Adult version. Manual. (Psychological Corporation, 2000).
Figures