1778
Multi-planar, multi-contrast and multi-timepoint analysis tool (MOCHA) for intracranial vessel wall imaging review1University of Washington, Seattle, WA, United States, 2Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Synopsis
A visualization technique (MOCHA) was developed to facilitate intracranial artery review using 3D Magnetic Resonance vessel wall imaging. Multiple intracranial MR scans, either from multiple contrasts or timepoints, are registered, then the artery of interest is traced and straightened using multiplanar reformation. Scans of 15 subjects with intracranial atherosclerosis were reviewed using MOCHA by a novice reader, with the traditional review method as comparison. The results showed higher sensitivity for plaque identification and higher accuracy for quantifying plaque features with MOCHA. MOCHA is promising for artery reviews using multiple scans, such as identifying plaque components and monitoring vessel wall thickening.
Introduction
Atherosclerosis is one of the leading causes of transient or permanent cerebral ischemic events, and can present with severe luminal narrowing or less stenotic unstable lesions due to arterial remodeling. A high rate of stroke related mortality occurs in Asian countries (1), but pathological evidence of intracranial atherosclerosis is also shown in 80–97% of the European population by the age of 65 years (2).MRI with multiple contrast weightings and multiple timepoints are useful in plaque compositional analysis and plaque progression monitoring. The traditional review of locating the same plaque from multiple scans or timepoints then quantifying plaques through a fixed view angle is neither convenient nor reliable, thus not likely to be used in the clinical setting.
Due to the slightly different scanning orientations and possibly different scanning resolutions, reliable registrations of all the contrast weighted images in multiple timepoints to the same artery region are critical for vessel wall review. However, registration is not easily achievable due to the imaging resolution, various signal patterns of different weighted images, and the tortuous structure of arteries, especially for intracranial arteries.
Multiplanar reformation (MPR) of arteries, considered as straightening the artery along its centerline, has been used in clinical reading and reported to be beneficial for coronary and renal artery stenosis detection (3,4). MPR view incorporates neighboring information along the artery centerline and is better suited for plaque identification in a long tortuous intracranial artery.
Therefore, we developed and validated a semi-automated visualization technique (Multi-planar, multi-contrast and multi-timepoint view for artery characterization, MOCHA) for plaque identification and measurement, including the critical steps of multi-contrast weighted or timepoint registration and MPR reformation, which is streamlined for clinical use.
Methods
MOCHA includes three components: multi-contrast and multi-timepoint registration, artery tracing, MPR generation.Registration: Images of different resolutions were resampled into the same isotropic resolution. Then images of different contrasts were registered using mutual information as the similarity metric. It was previously shown that the method is robust for registering pairs of scans from different timepoints but the same contrast, and any pairs of contrasts among black blood vessel wall images such as T1, contrast enhanced T1, T2, proton density, and MR angiography (MRA) sequences such as Time-of-Flight (ToF) and Simultaneous Noncontrast Angiography and intraPlaque hemorrhage (SNAP) (5).
Artery tracing: An automatic artery tracing method was used to accurately identify artery centerlines from MRA (6). A human reviewer can edit the automatically generated centerlines to correct mistakes with a graphical user interface.
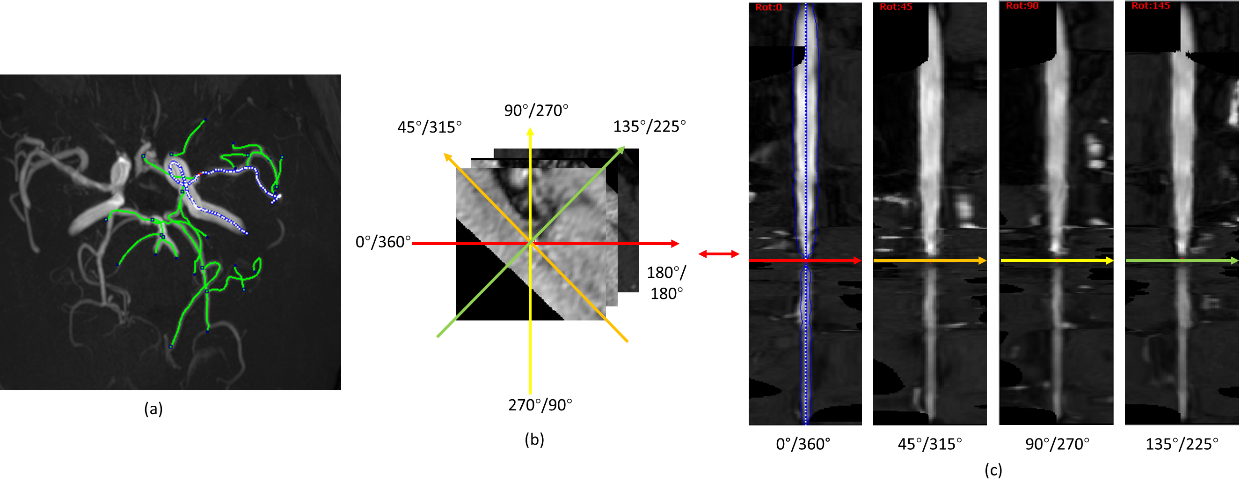
MPR generation: After registration, coordinates of the centerline can be used to interpolate in different scans for MPR images, which can be considered as stacked profiles of cross-sectional images along the centerline with a gap of 1 pixel. Rotation of profiles in each cross-sectional image leads to rotated MPR views for comprehensive display of the artery. An illustration for rotated MPR is shown in Figure 1.
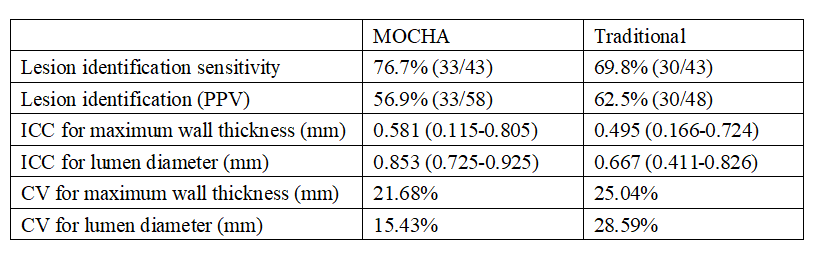
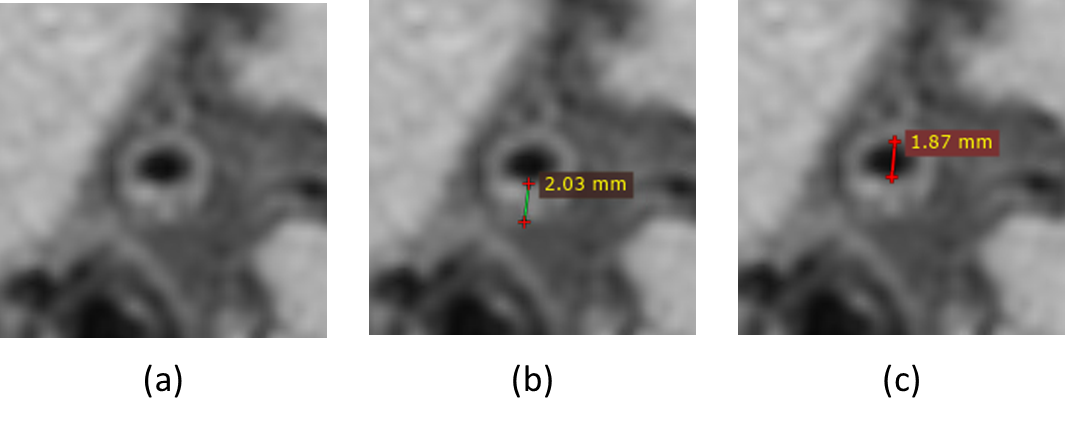
Validation: Scans from fifteen subjects with known intracranial plaques were used to validate MOCHA for intracranial review. A qualified radiologist but with limited vessel wall review experience (6 months) identified all plaque locations, and measured the maximum wall thickness and the corresponding lumen diameter at the cross-sectional slice with maximum thickening of each plaque using MOCHA, in addition to the traditional review. The measurements were performed using the RadiAnt DICOM Viewer (Meixant, Poznan, Poland), shown in Figure 4. The two reviews were performed with a gap of three weeks for washout. The consensus review results from two experienced reviewers, both with more than 5 years of vessel wall review experience were used as the ground truth. Sensitivity and Positive Predictive Value (PPV) for lesion identification, plaque measurement agreements (represented from intraclass coefficient [ICC], and coefficient of variation [CV]) were used to evaluate the review performance.
Results
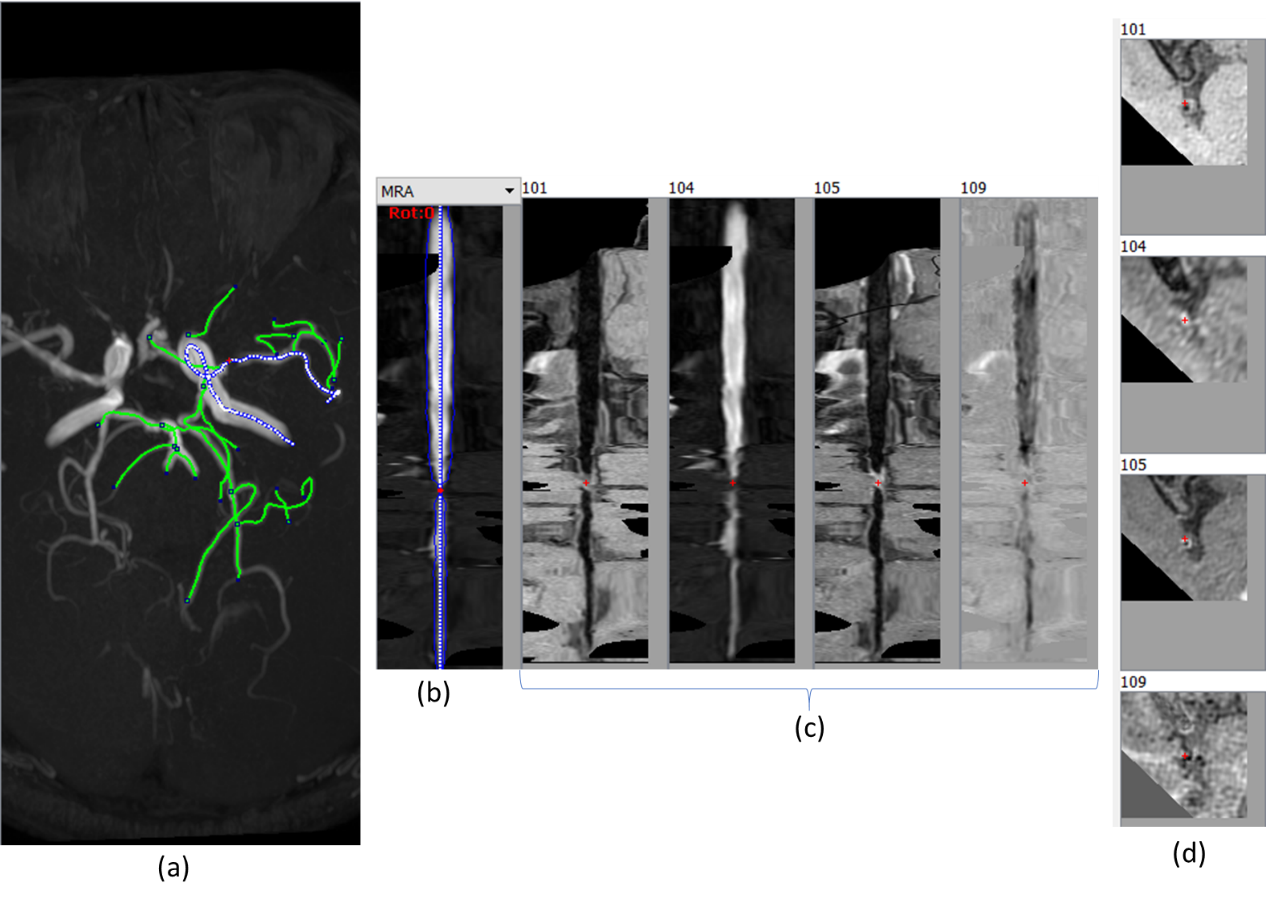
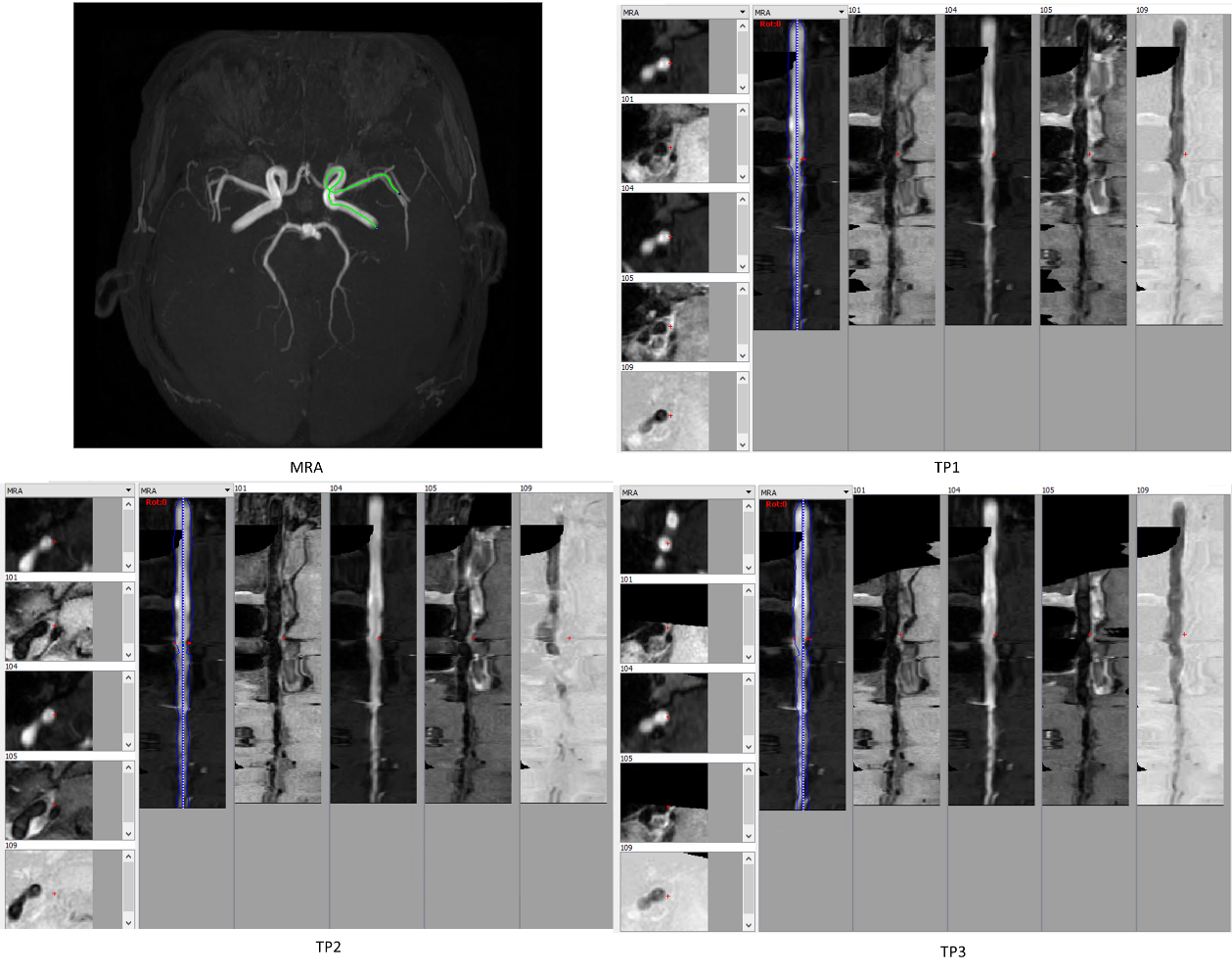
Two sets of generated MPR and cross-sectional views from four contrast weighted images in a single and three timepoints of an intracranial artery is shown in Figure 2 and Figure 3.The review performance comparison for intracranial plaques using MOCHA and the traditional method is shown in TABLE 1. Review using MOCHA shows a slightly higher sensitivity for plaque identification but lower PPV, and better plaque measurement agreements with ground truth.
Discussion
Through registration, tracing and MPR reformation, MOCHA is able to display the structures of tortuous arteries in straight lines, which allows easier interpretation of arteries and the plaques on the vessel wall. The automated artery tracing as well as the robust registration method capable of registering images of different resolutions and contrast weightings is essential to MOCHA. The review results show that the technique is reliable for intracranial artery review even for novice reviewers, whereas the traditional review suffers from the need for frequent changes in viewpoint orientation.Conclusion
MOCHA is a useful tool for semi-automated registration, tracing and MPR reformation for plaque review of multiple contrast weighted and/or timepoints scans, especially in tortuous arteries.Acknowledgements
This research is supported by grants from National Institutes of Health (R01-NS092207).References
1. Johnston SC, Mendis S, Mathers CD. Global variation in stroke burden and mortality: estimates from monitoring, surveillance, and modelling. Lancet Neurol. [Internet] 2009;8:345–354. doi: 10.1016/S1474-4422(09)70023-7.
2. Bos D, Van Der Rijk MJM, Geeraedts TEA, Hofman A, Krestin GP, Witteman JCM, Van Der Lugt A, Ikram MA, Vernooij MW. Intracranial carotid artery atherosclerosis: Prevalence and risk factors in the general population. Stroke 2012;43:1878–1884. doi: 10.1161/STROKEAHA.111.648667.
3. Ropers D, Baum U, Pohle K, Anders K, Ulzheimer S, Ohnesorge B, Schlundt C, Bautz W, Daniel WG, Achenbach S. Detection of Coronary Artery Stenoses With Thin-Slice Multi-Detector Row Spiral Computed Tomography and Multiplanar Reconstruction. Circulation [Internet] 2003;107:664–666. doi: 10.1161/01.CIR.0000055738.31551.A9.
4. Berg MH, Manninen HI, Vanninen RL, Vainio PA, Soimakallio S. Assessment of renal artery stenosis with CT angiography: usefulness of multiplanar reformation, quantitative stenosis measurements, and densitometric analysis of renal parenchymal enhancement as adjuncts to MIP film reading. J. Comput. Assist. Tomogr. [Internet] 1998;22:533–40.
5. Wang J, Börnert P, Zhao H, et al. Simultaneous noncontrast angiography and intraPlaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation. Magn. Reson. Med. 2013;69:337–345. doi: 10.1002/mrm.24254.
6. Chen L, Mossa-Basha M, Balu N, Canton G, Sun J, Pimentel K, Hatsukami TS, Hwang JN, Yuan C. Development of a quantitative intracranial vascular features extraction tool on 3D MRA using semiautomated open-curve active contour vessel tracing. Magn. Reson. Med. [Internet] 2018;79:3229–3238. doi: 10.1002/mrm.26961.
7. Chen L, Sun J, Canton G, Balu N, Zhao X, Li R, Hatsukami TS, Hwang J, Yuan C. Automated Artery Localization and Vessel Wall Segmentation of Magnetic Resonance Vessel Wall Images using Tracklet Refinement and Polar Conversion. arXiv [Internet] 2019.
8. Peterfy CG, Schneider E, Nevitt M. The osteoarthritis initiative: report on the design rationale for the magnetic resonance imaging protocol for the knee. Osteoarthr. Cartil. [Internet] 2008;16:1433–1441. doi: 10.1016/j.joca.2008.06.016.
Figures