1767
Accelerating magnetic resonance angiography using Compressed SENSE technology - a prospective multi-center study1Department of Radiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2Beijing Royal Integrative Medicine Hospital, Beijing, China, 3First Affiliated Hospital of Dalian Medical University, Dalian, China, 4Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Jiangsu, China, 5Shengjing Hospital of China Medical University, Shenyang, China, 6the First Affiliated Hospital of Chongqing Medical University, Chongqing, China, 7Philips Healthcare, Beijing, China
Synopsis
Clinical feasibility of using Compressed SENSE (CS-SENSE) technology to shorten the scan time of Time-of-flight (TOF) magnetic resonance angiography (MRA) and optimal acceleration factor were investigated via a multi-center study. Ninety subjects underwent 8 customized TOF-MRA sequences including sequences with CS-SENSE technology, SENSE technology and without acceleration technology. Subjective assessments including evaluations of artery branches and artifacts, and objective measurements including signal-to-noise ratio, contrast-to-noise ratio and peak signal-to-noise ratio were performed. The results indicated that TOF-MRA using CS-SENSE with an optimal acceleration factor (4 to 6) provided comparable results compared with traditional TOF-MRA sequences, and significantly increased the scan efficiency.
Introduction
Time-of-flight (TOF) magnetic resonance angiography (MRA) is one of the most commonly used MR sequences in the cerebrovascular examinations. Although contrast agent injection is not needed for TOF-MRA, it takes a relatively long scan time which needs patient cooperation1. Application of Compressed SENSE (CS-SENSE) technology can shorten the scan time of MRA and increase the efficiency. However, the clinical feasibility and the optimal acceleration factor of CS-SENSE technology in MRA have not been investigated.Objective
This study aimed to evaluate the clinical application and effectiveness of accelerated TOF-MRA by employing CS-SENSE technology.Methods
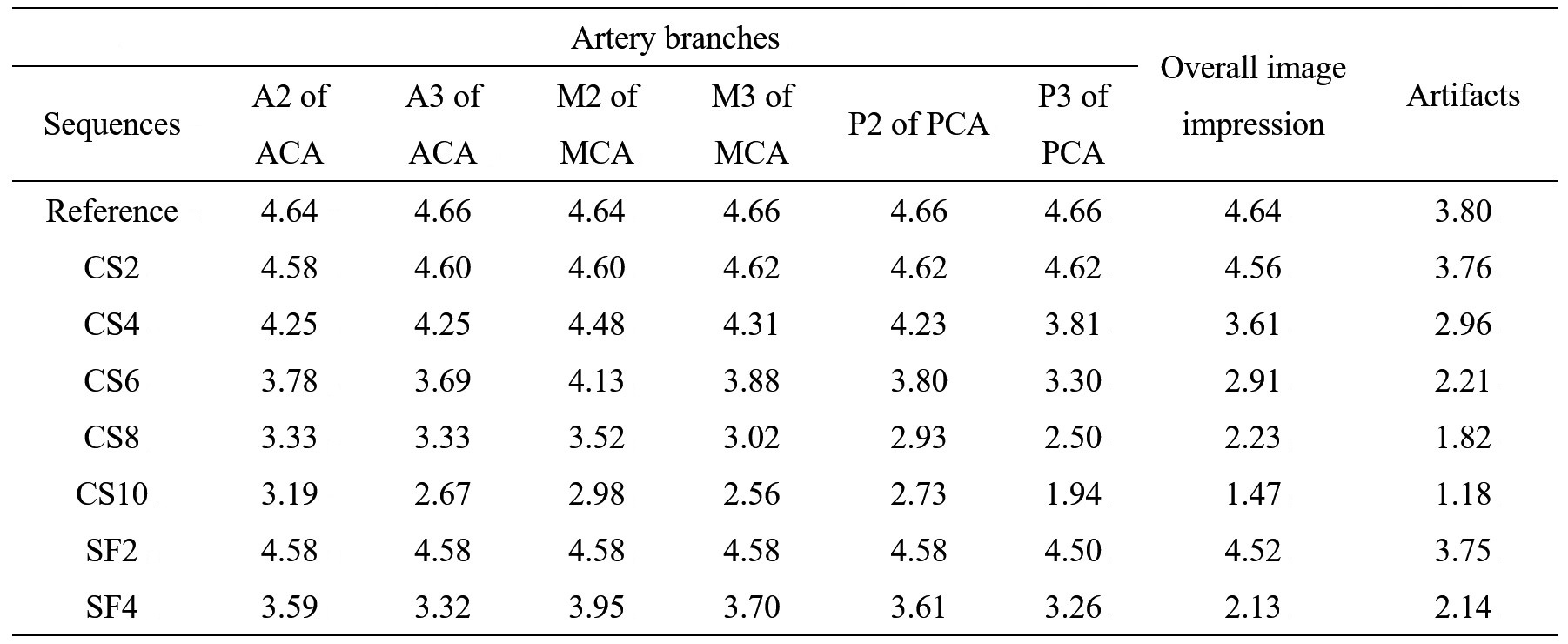
Ninety subjects including 42 healthy volunteers and 48 patients with cerebrovascular diseases were enrolled in this study with informed consents (49 males and 41 females with age ranged from 12 to 71), and all the data were prospectively acquired from a multi-center study with 5 sites (including Beijing Tiantan Hospital, Capital Medical University, 26 cases; Beijing Royal Integrative Medicine Hospital, 24 cases; Shengjing hospital of China Medical University, 15 cases; Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, 15 cases; and First Affiliated Hospital of Dalian Medical University, 10 cases) on 3.0T MR systems (Ingenia CX, Philips Healthcare, the Netherlands). All patients underwent 8 different customized TOF-MRA sequences which included 5 sequences utilizing CS-SENSE technology with different acceleration factors (2, 4, 6, 8 and 10, denoted as CS2, CS4, CS6, CS8 and CS10 respectively), 2 sequences utilizing traditional SENSE technology with different SENSE factors (2 and 4, denoted as SF2 and SF4 respectively), and 1 sequence without acceleration technology used as reference. Signal to noise ratio (SNR), contrast to noise ratio (CNR) and peak signal to noise ratio (PSNR) were calculated by setting distal M1 segment of the middle cerebral artery as the region of interest (ROI) and setting the splenium of the corpus callosum which revealed a relatively uniform intensity distribution as a contrast2,3. The image quality which focused on the visualization of artery branches (including A2 and A3 of the anterior cerebral artery, M2 and M3 segments of the middle cerebral artery, and P2 and P3 segments of the posterior cerebral artery) and overall image impression was independently evaluated by two experienced radiologists using a five-grade scoring system (1~unsatisfactory, 2~fair, 3~average, 4~good, and 5~excellent.). The artifacts were evaluated using a four-grade scoring system (1~severe artifact, 2~moderate artifact, 3~mild artifact, and 4~no artifact.). Finally, one optimal sequence for each patient was determined by each radiologist after comprehensively considering the scan time and image quality. Statistical analysis was carried out using SPSS 19.0.Results
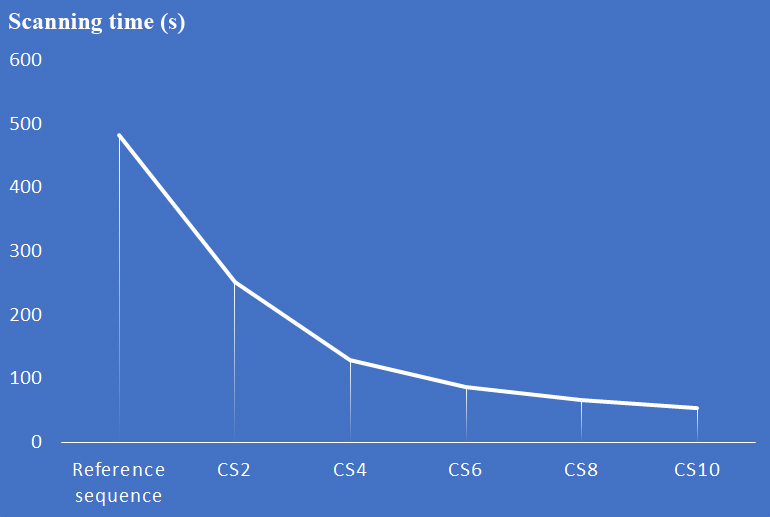
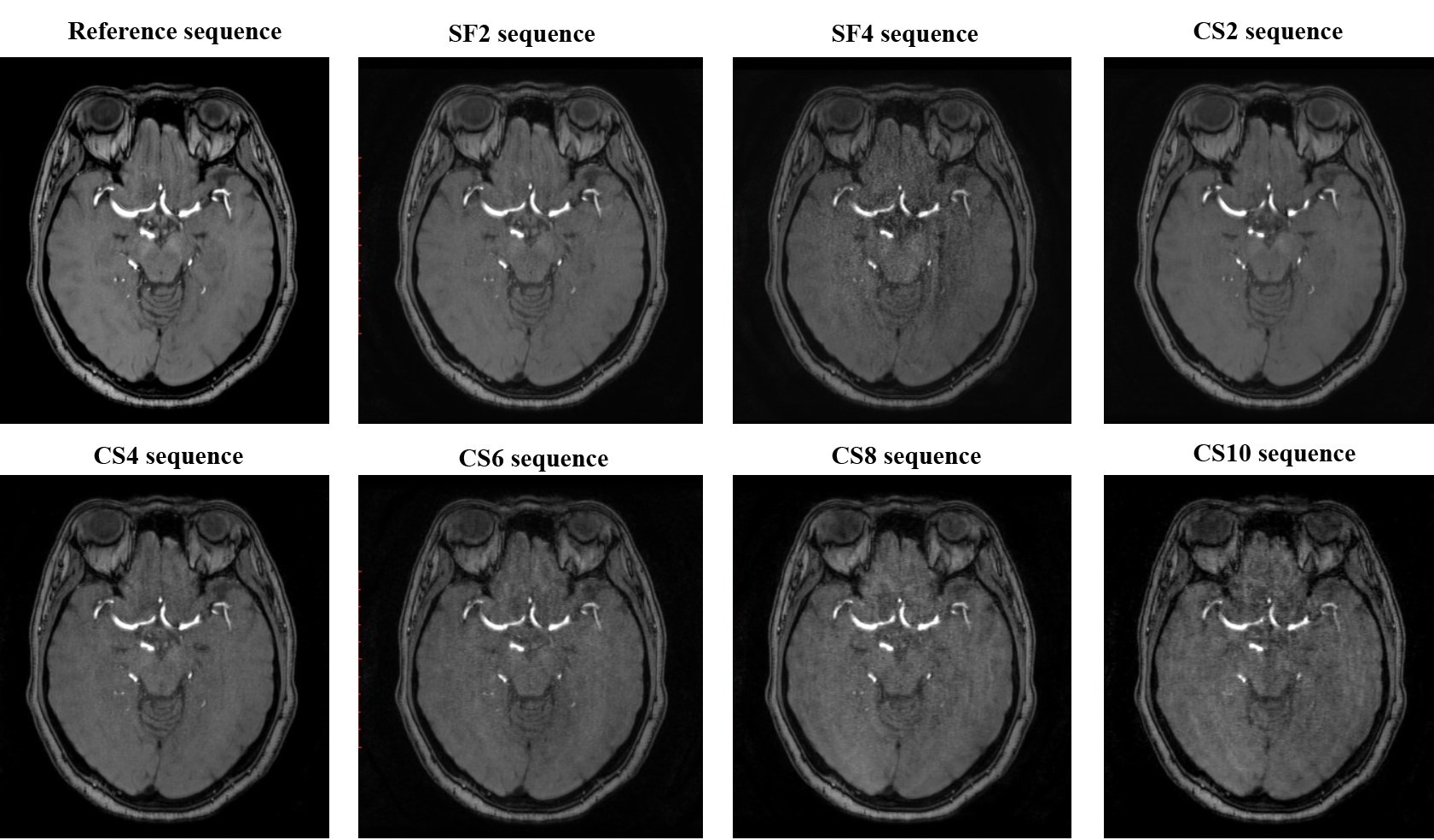
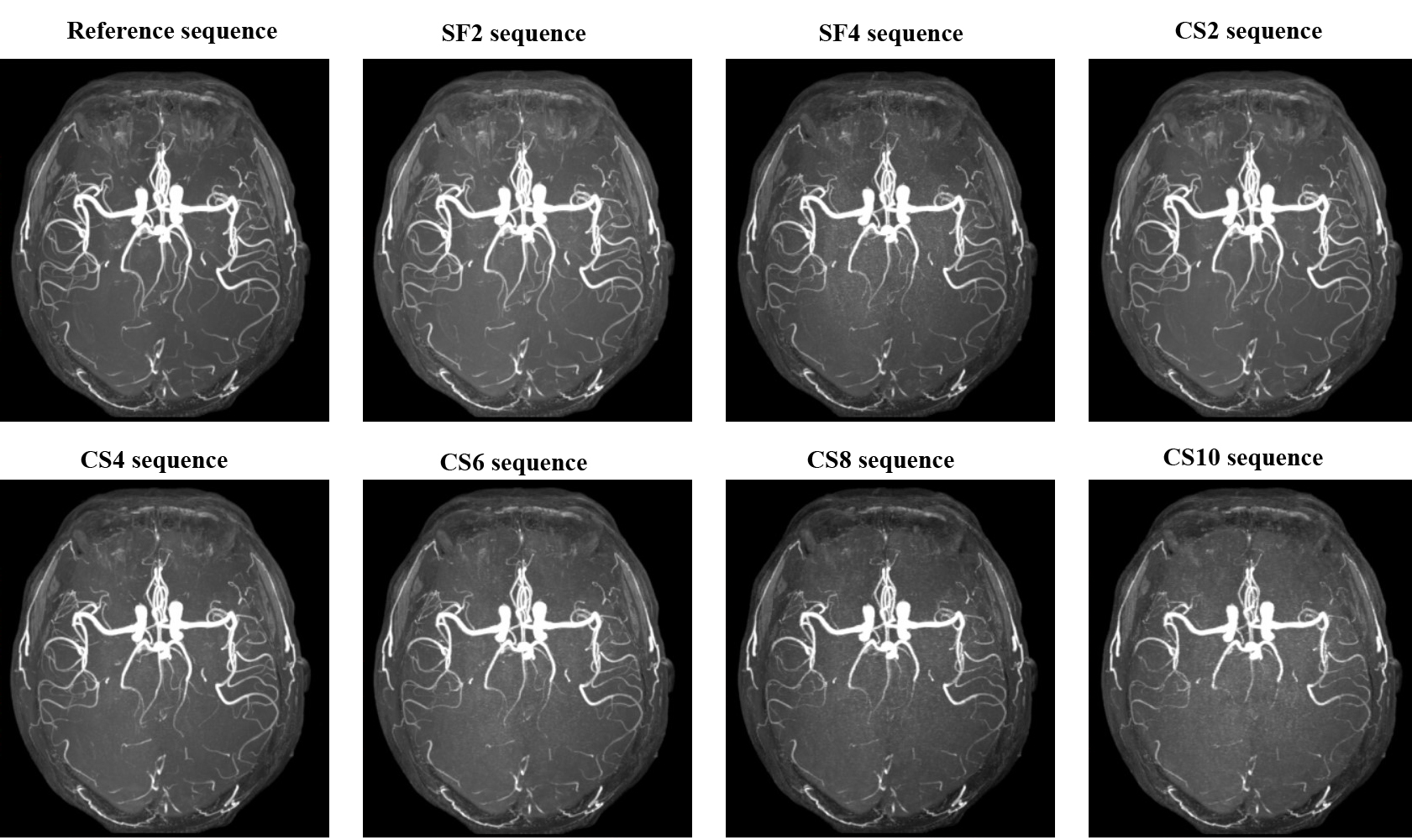
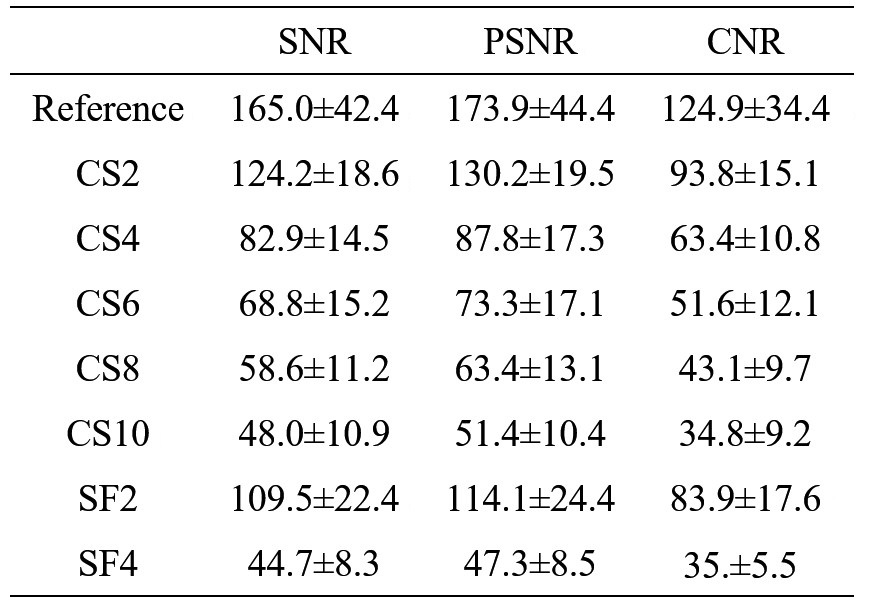
Compared with the reference sequence, the scan times of TOF-MRA were reduced by 47.9%, 73.2%, 82.0%, 86.3% and 89.0% by setting the CS-SENSE acceleration factor as 2, 4, 6, 8 and 10 respectively (Figure 1). The SNR, PSNR and CNR of the 8 sequences are listed in Table 1. The scorings of artery branches, overall image impression and artifacts of the eight sequences are shown in Table 2. For the scoring system, there was a good consistency between the results from different radiologists (K=0.872, P<0.05). Image scorings of CS2 sequence and SF2 sequence were nearly the same, however, image scoring of SF4 was obviously lower than that of CS4 and CS6 sequence. CS4 sequence (72%) and CS6 sequence (28%) were determined by two radiologists as the optimal choices after comprehensively considering the scan time and image quality. Axial images at the middle cerebral artery level of the 8 sequences for a patient with cerebrovascular disease are shown in Figure 2 and typical MIP images are shown in Figure 3. The distal tiny branches were unclear or even missing when the CS-SENSE acceleration factor was set too high (such as CS-SENSE acceleration factor was bigger than 6, as Figure 3 shows).Discussion and Conclusion
For TOF-MRA sequence, image quality is generally acceptable or even better by employing optimal CS-SENSE acceleration factor compared to the traditional SENSE technology. The subjective scorings and objective measurements degrade with the increase of CS-SENSE acceleration factor. The optimal CS-SENSE acceleration factor of 4 to 6 is recommended by balancing the shortened scan time and diagnostic image quality and thus the image acquisition efficiency increases by about 274% to 454% compared to the reference. There are some limitations in the current study. It only presents a preliminary analysis of CS-SENSE technology in the application of TOF-MRA utilizing the data acquired from multi-center till now. In the future study, more patients will be enrolled in this study, and more comprehensive subjective assessments and objective measurements will be performed in the cerebrovascular diseases, especially for hemadostenosis and aneurysm.Acknowledgements
References
1. Gaa J, Weidauer S, Requardt M, et al. Comparison of Intracranial 3D-ToF-MRA With and Without Parallel Acquisition Techniques at 1.5T and 3.0T: Preliminary Results[J]. Acta Radiologica, 2004, 45(3):327-332.
2. Bratke G, Rau R, Weiss K, et al. Accelerated MRI of the Lumbar Spine Using Compressed Sensing: Quality and Efficiency[J]. Journal of Magnetic Resonance Imaging, 2019, 49(7):e164-e175.
3. Vranic J E, Cross N M, Wang Y, et al. Compressed Sensing–Sensitivity Encoding (CS-SENSE) Accelerated Brain Imaging: Reduced Scan Time without Reduced Image Quality[J]. American Journal of Neuroradiology, 2019, 40(1):92-98.
Figures