1764
Evaluation of 4D ultrashort TE MR Angiography using Variable Inversion Time.1Department of Radiology, Graduate School of Medicine, University of Tokyo, Tokyo, Japan, 2Department of Radiology, Juntendo University Graduate School of Medicine, Tokyo, Japan, 3Department of Radiology, Juntendo University Hospital, Tokyo, Japan
Synopsis
We developed a novel method, Variable TI, to improve the visibility of ASL based UTE 4D-MRA. In the phantom study and the volunteer study, the Variable TI UTE 4D-MRA offered a higher signal intensity and improved visualization of arteries in late phase compared to the conventional method. The Variable TI technique can improve clinical usability of 4D-MRA because this technique not only offered better visibility of arteries but also realized the data efficacy and reduced reconstruction time.
Introduction
Non-contrast enhanced 4D dynamic MR angiography has been applied to visualize hemodynamic flow characteristics of pathological cerebral veins. It is especially important for a range of clinical applications such as assessment of the endovascular embolization of arteriovenous malformations/fistulas (AVMs/AVFs). 3D-TOF imaging is capable of imaging arterial components of AVMs, however, it does not routinely visualize venous structures nor hemodynamic information which is important in assessing AVMs. However, even with Arterial Spin Labeling based ultrashort TE 4D MR Angiography (UTE 4D-MRA), sufficient visualization of AVMs can be challenging because the arterial phase requires high temporal resolution, increasing number of RF excitations causes signal decay in later phase, besides large amounts of data lead to long reconstruction time. Venous imaging can be limited because of transit-time signal decay.$$$^{1-3}$$$ On the other hand, less acquisition in early phase can reduce sensitivity of identification of small arterial feeders. In this study, we applied variable inversion time (VTI) to UTE 4D-MRA in order to overcome the limitations of conventional method and evaluated this innovative approach with phantom and volunteer study.Methods
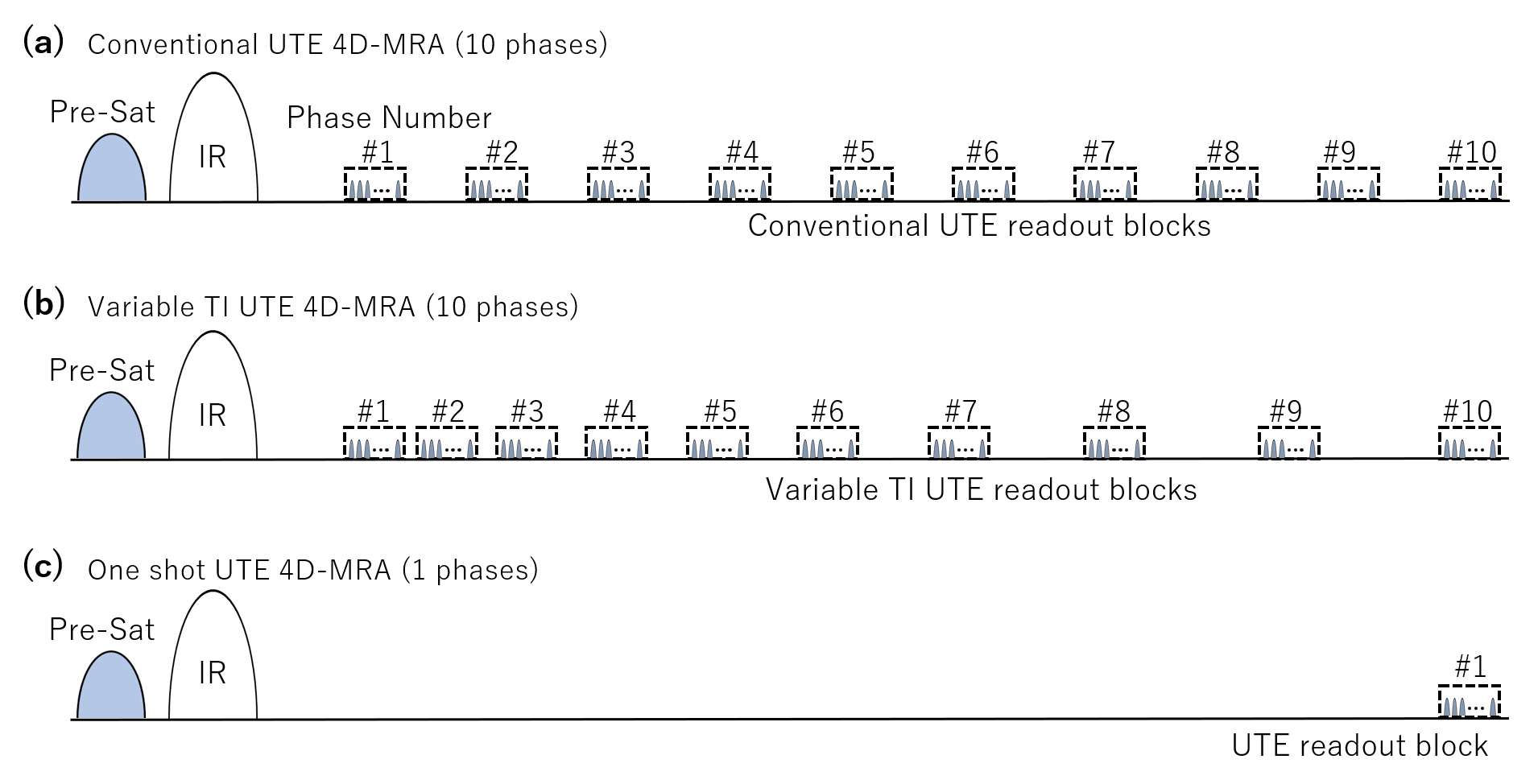
All subjects were scanned on a 3 Tesla MRI scanner (Vantage Galan 3T ZGO, Canon Medical Systems Corporation, Japan) using a 16-channel head coil for signal reception. The data acquisition was based on a 3D radial sampling, and ASL technique was used as a preparation pulse to visualize blood flow. The UTE readout consisted of a series of blocks, data from each readout block were used to construct a single image, using half sinc pulses with a duration of about 30 μs and flip angles up to 6°. Imaging parameters were as follows: FOV = 224 x 224 mm$$$^{2}$$$, number of slices = 200, resolution = 1 x 1 x 1 mm$$$^{3}$$$, TR/TE = 3.7/0.1 ms, shot interval = 3000 ms, 4050 radial projections were acquired within 15 minutes. The signal intensity was evaluated using flow phantom 8 cm/s of flow velocity whose $$$T_{1}$$$ relaxation time was adjusted to 1200 ms with gadolinium agent. For the conventional method, we used 10 TI steps from 200 to 2810 ms with equally spaced intervals. For the VTI method, we used 10 TI phases ranging from 200 to 2810 ms with a manner of progression of difference, as shown in figure 1. For comparison, single TI phase (TI = 2810 ms) acquisition was performed using otherwise identical imaging parameters. Three healthy volunteers (2 males, 1 female; mean age, 39 years) without history of cerebrovascular diseases were scanned and evaluated for visibility of arteries. For comparison, volunteers were scanned with the conventional and VTI method, in VTI method we evaluated with several TI phase using otherwise identical imaging parameters.Results
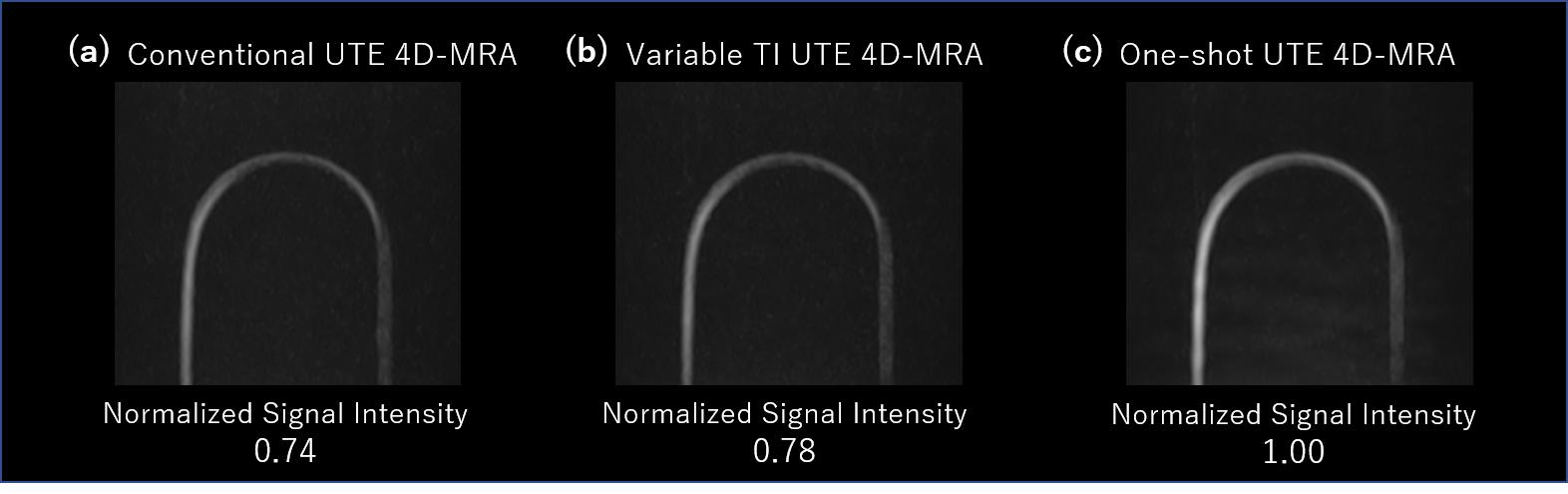
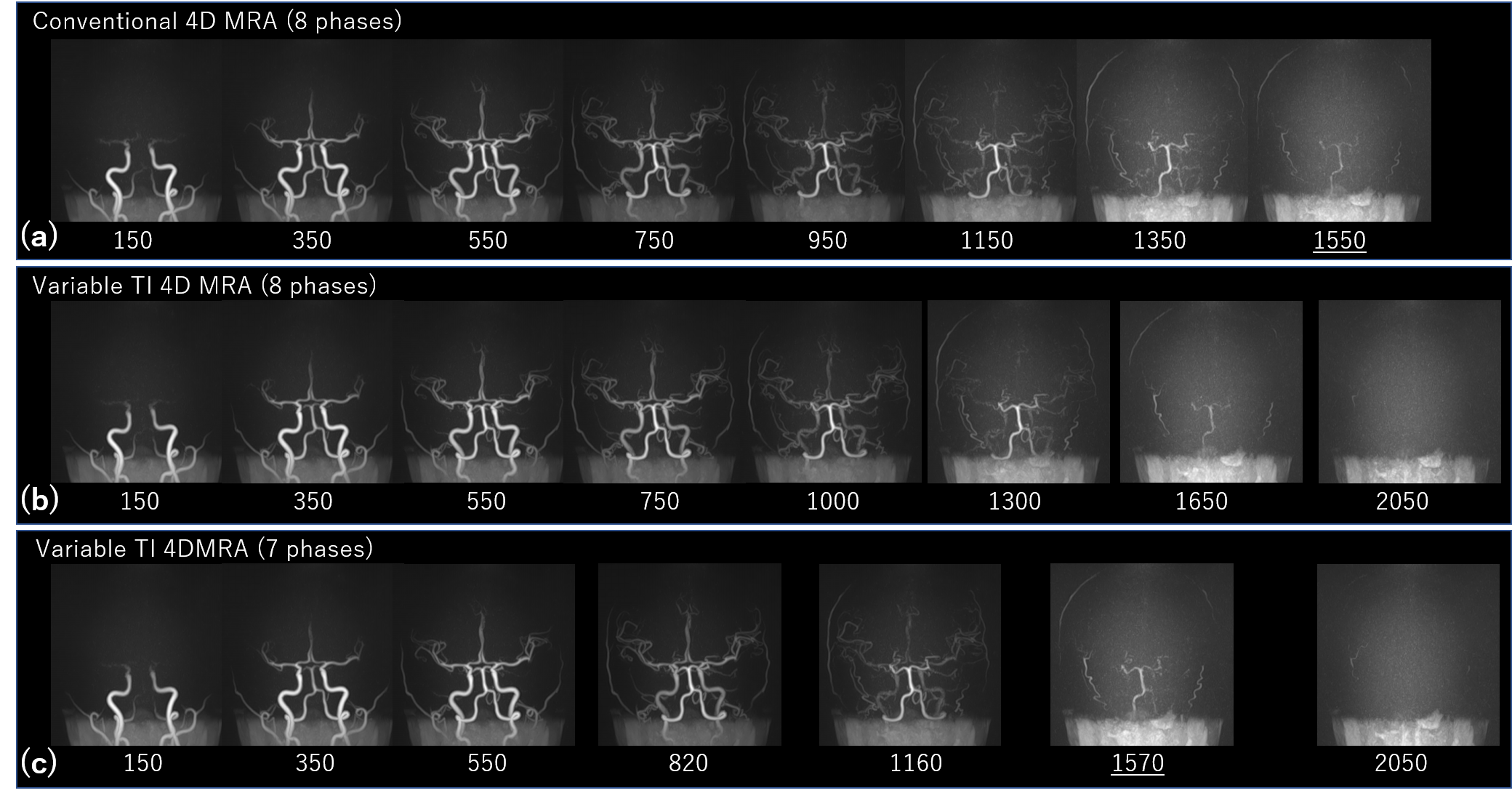
The late phase signals of VTI UTE 4D-MRA were higher than those achievable with conventional method. In the last phase (TI = 2810 ms) of the phantom study, the signal intensity acquired with VTI was approximately 5% higher than that of conventional sequence. In the volunteer study, as indicated in figure. 3, VTI UTE 4D-MRA allowed improved visualization of the arteries in later phase. Reduced number of acquisitions in late phase did not cause lack of the structural information because the distal part of blood flow was relatively slow. The reconstruction time was shortened roughly in proportions to number of phases.Discussion
In the phantom study, the late phase signals of VTI UTE 4D-MRA were higher than that of the conventional method. In 4D MRA, the apparent blood $$$T_{1}$$$ may be shorter than the true blood $$$T_{1}$$$ and $$$T_{2}$$$ decay also made shorted by the influence of blood flow velocity and imaging parameter such as the repetition of UTE RF pulse and flip angle. In comparison with the one shot acquisition, the signal of the 10th acquisition had lost approximately 26% of its signal, which indicated there was significant $$$T_{2}$$$ decay in series of 9 phases of UTE readout process. For a RF pulse with bandwidth is much greater than $$$1/T_{2}$$$, the longitudinal magnetization after a pulse, neglecting $$$T_{1}$$$, will be approximately:$$ M_{z}(T_{2}) \cong M_{0} \left(1-T_{2}\int_{-\infty}^{\infty} A_{1}(t)^{2}dt\right) $$
$$ = M_{0} \left(1-T_{2}\int_{-\infty}^{\infty} \mid F_{1}(f)\mid\ ^{2} df \right), $$
Where $$$A_{1}(t)$$$ is the RF pulse amplitude and $$$F_{1}(f)$$$ is its Fourier transform$$$^{4}$$$. This indicates that the change in longitudinal magnetization is proportional to $$$T_{2}$$$ and the RF power which is from the inversion pulse and series of UTE acquisition process. RF pulse with large power and wide bandwidth tips more of the short-$$$T_{2}$$$ magnetization into the transverse plane, causing more $$$T_{2}$$$ relaxation to occur. In this point of view, it is appropriate to reduce the number of acquisitions in late phases where high temporal resolution is not necessary. For clinical setting, further refinement of TI phase setting would be required.
Conclusion
In this study, we presented a novel VTI UTE 4D-MRA technique, which provides better image quality in late phase compared to the conventional method. This approach can improve the clinical usability of 4D-MRA by improving visibility of the late phase and reducing redundant data, which also reduces reconstruction time. This new method has the potential to improve the assessment of many cerebrovascular diseases.Acknowledgements
The author would like to thank to the Juntendo University, Tokyo University, Canon Medical Systems, and Hiroshi Kusahara for his assistance with the programming.References
1. Tyler DJ, Robson MD, Henkelman RM, Young IR, Bydder GM. Magnetic resonance imaging with ultrashort TE (UTE) PULSE sequences: technical considerations. J Magn Reson Imaging 2007; 25: 279–289.
2. Gönner F, Heid O, Remonda L, et al. MR angiography with ultrashort echo time in cerebral aneurysms treated with Guglielmi detachable coils. AJNR Am J Neuroradiol 1998;19:1324–28 pmid:9726477
3. Nielsen HTC, Gold GE, Olcott EW, Pauly JM, Nishimura DG. Ultra-short echo-time 2D time-offlight MR angiography using a half-pulse excitation. Magn Reson Med 1999;41:591–599.
4. Larson PEZ, Conolly SM, Pauly JM, Nishimura DG. Using adiabatic inversion pulses for long-T2 suppression in ultrashort echo time (UTE) imaging. Magn Reson Med. 2007;58(5):952–961.
Figures