1761
Improved presentation of brachial plexus at 3T using diffusion-weighted imaging with multiple interleaves in the phase-encode direction
Ke Jiang1, Jiazheng Wang1, and Yuefei Ma1
1Philips Healthcare Greater China, Beijing, China
1Philips Healthcare Greater China, Beijing, China
Synopsis
Diffusion weighted imaging for brachial plexus can provide useful information for clinical applications. However, clinical DWI usually employs single-shot EPI for signal acquisition, which suffers from image distortion or signal loss especially in the imaging in the head-neck regions due to the spatial variation in B0 field. This work demonstrated the application of a multi-interleave DWI sequence that achieves quality brachial plexus imaging with a resolution of 1.9x1.9 mm2 at 3T system.
Introduction
Diagnosis of brachial plexopathy remains a challenge as the symptoms are usually non-specific and enough localization of lesions is difficult[1]. DWI with single-shot EPI trajectory (ssDWI) as the clinical routine may suffer from image distortion due to the B0 field inhomogeneity and long-term eddy currents. Recently, DW-EPI with multiple excitations and interleaved phase-encoding (msDWI) was proven to reduce image distortion with increased sampling-bandwidth in the phase-encode direction [2]. So far the value of msDWI has not been established for brachial plexus. This work aims to demonstrate the feasibility of msDWI for brachial plexus at 3T system.Method
A schematic diagram of the msDWI sequence is shown in Figure 1, where a series of navigator signals were acquired through a second spin echo after the regular readout train, the two trains split by a second refocusing pulse. Each regular readout train only traverse a portion of the k-space (interleave) and the navigator was designed to cover a k-space with smaller coverage. A comparison of the navigator phase maps between interleaves reveals the relative motion which could be removed before the reconstruction of the final image. The brachial plexus DWI experiment was conducted at 3.0 T (Ingenia Elition, Philips healthcare, Best, the Netherlands) on a healthy volunteer, study approved by a local IRB. Common scan parameters for both ssDWI and msDWI: FOV = 300*119mm2, voxel size=1.9*1.9mm2, TR=3000ms, b=800s/mm2, NSA for b0/800 =1/5. The msDWI was acquired using 2 interleaves, resulting in a shorter TE than the ssDWI (77 v.s. 127 ms). The scan time was 3.6 min for msDWI and 1.8 min for ssDWI. SPTR (Spectral Pre-saturation with Inversion Recovery) was used for fat suppression and non-coplanar excitation (ZOOM) was used for the reduced FOV for both sequences.Result
Figure 2 shows the brachial plexus DWI images acquired by both ssDWI and msDWI and MIP was done to better display brachial plexus. Severe signal loss was observed only on ssDWI (white arrowed). msDWI was also shown to better present the fine-structures (yellow arrow) due to the reduced signal displacement.Discussion
We demonstrated the feasibility of msDWI for brachial plexus imaging using multiple interleaves and navigators to remove motion-induced phase-mismatch between interleaves. Compared to ssDWI, signal loss and geometry distortion was less obvious on msDWI image. The scan efficiency of msDWI may be further improved by reducing TR or utilizing acceleration acquisition technique.Conclusion
For brachial plexus DWI, image without signal loss can be acquired by msDWI.Acknowledgements
No acknowledgement found.References
[1]. Carlos Torres, .et al. Neuroradiol J. 2013 Dec; 26(6): 699–719.
[2]. Ha-Kyu Jeong, et al. Magn Reson Med. 2013 Mar 1; 69(3): 793–802.
Figures
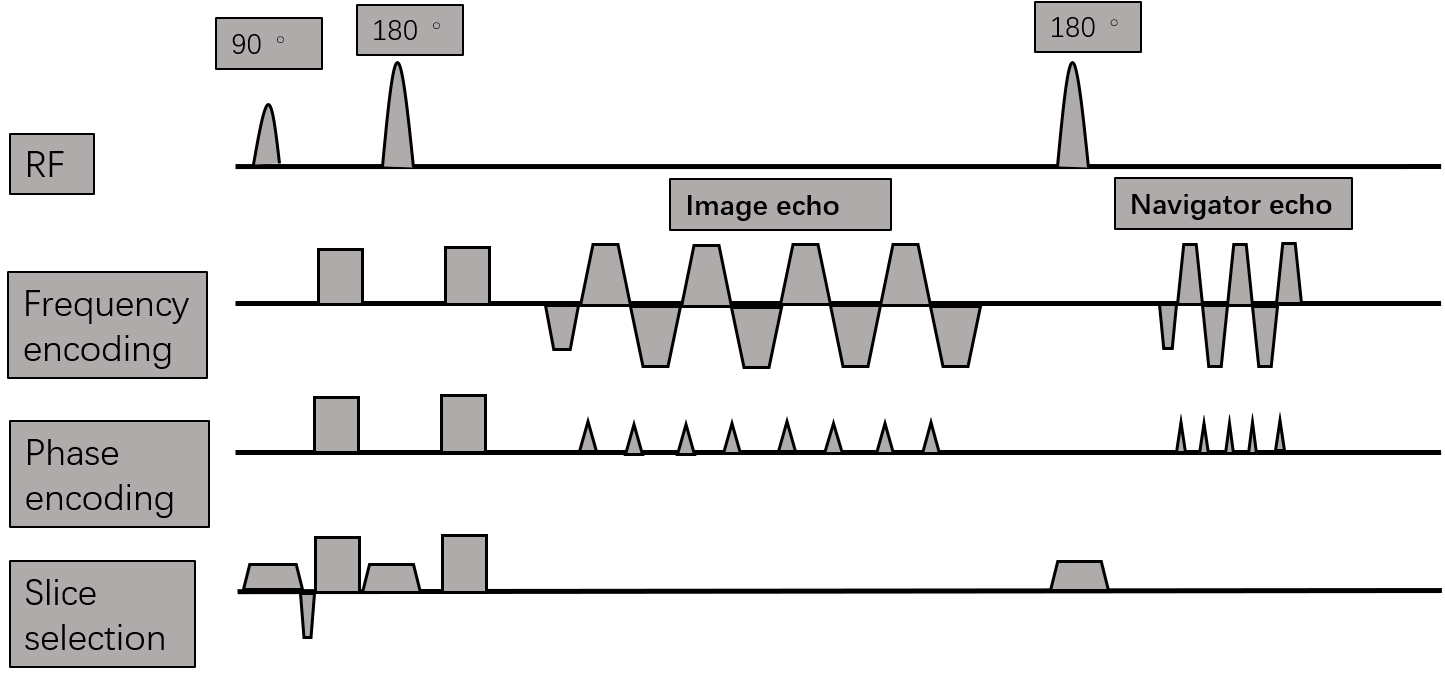
Figure 1. Schematic diagram of msDWI. Additional navigator echo is acquired following conventional image echo after refoucing.
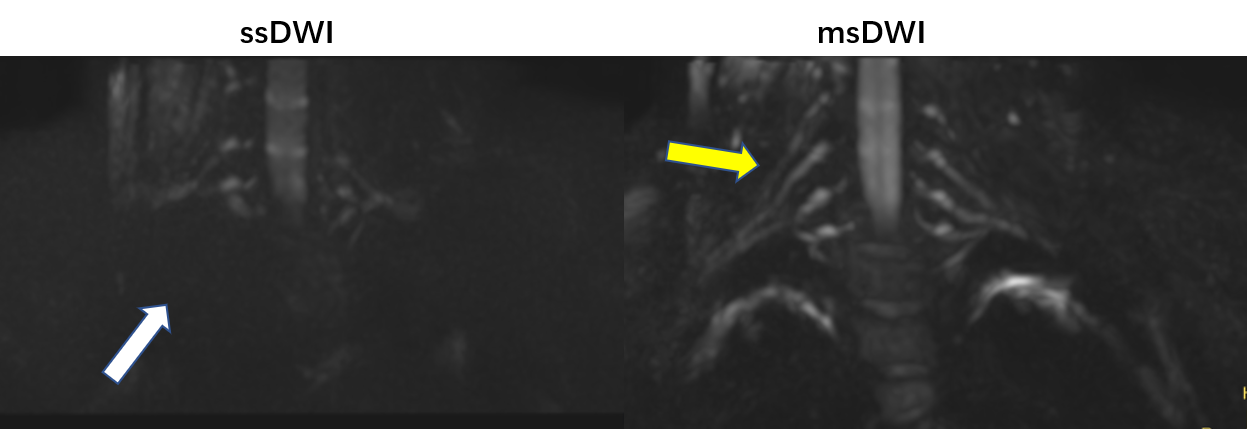
Figure 2. Representative brachial
plexus images obtained from ssDWI (left) and msDWI (right) after MIP. Signal loss observed on ssDWI is indicated by white arrow. Better presentation of brachial plexus on msDWI is indicated by yellow arrow.