1689
Velocity and pulsatility in small cerebral perforators of CADASIL patients compared to healthy controls
Tine Arts1, Hilde van den Brink2, Anna Kopczak3, Martin Dichgans3, Jeroen Hendrikse1, Jeroen Siero1,4, Jaco Zwanenburg1, and Geert Jan Biessels2
1Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Neurology, University Medical Center Utrecht, Utrecht, Netherlands, 3Institute of Stroke and Dementia Research, Munich, Germany, 4Spinoza Centre for Neuroimaging, Amsterdam, Netherlands
1Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Neurology, University Medical Center Utrecht, Utrecht, Netherlands, 3Institute of Stroke and Dementia Research, Munich, Germany, 4Spinoza Centre for Neuroimaging, Amsterdam, Netherlands
Synopsis
CADASIL is a monogenic form of cerebral small vessel disease that leads to ischemic brain lesions at mid-adult age. We studied arterial perforator blood flow velocity and pulsatility in CADASIL patients and matched controls. We found significantly lower velocity and higher pulsatility in the basal ganglia and in normal appearing white matter (NAWM) of the centrum semi-ovale (CSO) in patients compared to controls. Within patients, no differences in velocity and pulsatility were found between CSO NAWM and white matter hyperintensities. This shows that small vessel disease in CADASIL patients is reflected in abnormal small vessel function also beyond lesioned areas.
Introduction
CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy) is the most common monogenetic variant of cerebral small vessel disease. In CADASIL, granular osmiophilic material (GOM) is deposited in small artery membranes, leading to smooth muscle cell degeneration and thickening of the vascular wall. This particularly affects cerebral perforators, resulting in mid-adult onset of ischemic stroke, cognitive decline progressing to dementia, subcortical infarcts and white matter lesions.1–5 Recent MRI developments enable detection of small perforating arteries, with quantitative measurements of blood flow velocity and pulsatility in the basal ganglia (BG) and centrum semi-ovale (CSO) using 2D phase contrast angiography (PCA) on 7 Tesla MRI.6,7 The main goal of this study is to investigate small perforator blood flow velocity and pulsatility in CADASIL patients, in comparison to matched healthy controls, to explore if small vessel disease in these patients can be detected in the vessels themselves. We study the perforators in the BG and normal appearing white matter (NAWM) and lesioned tissue of the CSO.Methods
BG and CSO imaging data of 22 CADASIL patients (age 52±10) and 12 controls (age 47±13) were collected at the University Medical Center Utrecht (7 Tesla MRI data) and the Ludwig-Maximilians-University Munich (3 Tesla MRI data) from the Zoom@SVDs study, as part of the SVDs@target program (supported by European Union's Horizon 2020 programme grant agreement 666881). Using a 2D PCA acquisition on 7 Tesla MRI (Philips) with a 32-channel head coil (Nova Medical), small perforators were detected in the BG and CSO. Scans were acquired with a 0.3mm in-plane resolution and encoding velocity of 20 and 4 cm/s for the BG and CSO, respectively.6 The CSO white matter (WM) was segmented using a 3D T1-weighted image (SPM12). The BG was segmented manually. In the CSO, ghosting artefacts were automatically removed from the WM segmentation.8 BG perforators oriented non-perpendicular to the PCA imaging plane were excluded. Finally, for the CSO and BG, perforators closer together than six voxels (1.8mm) were excluded, since these are mostly located on larger, non-perforating arteries. Perforator outcome measures are the mean blood flow velocity during the cardiac cycle (Vmean) and the pulsatility index (PI=(Vmax-Vmin)/Vmean). Because the number of detected perforators (Ndetected) depends on the mask size, the perforator count is expressed as a density (number of perforators/cm2 mask, Ndensity). In addition, we compared perforator outcome measures in CADASIL patients between NAWM and white matter hyperintensities (WMH) in the CSO. These WMH were manually delineated on a 3 Tesla FLAIR image.Results and discussion
One PC control scan was excluded due to scanner problems. One CSO control scan and one CSO patient scan were excluded due to motion artefacts, as were three BG control and two BG patient scans. One CSO control scan was excluded due to triggering problems.Vmean, PI and Ndensity in controls and CADASIL patients for the BG and NAWM of the CSO, are given in Table 1. Patients’ perforators showed a significantly lower Vmean and higher PI compared to controls in the BG and NAWM of the CSO. To note, the lower Vmean does not fully account for the higher PI values. In Figure 1, the mean velocity traces are normalized by division by Vmean and shown of all perforators combined, of patients and controls in the BG and the NAWM of the CSO. The figure clearly shows a larger velocity span and thus a higher pulsatility in patients compared to controls. The higher PI in patients agrees with known CADASIL characteristics: in CADASIL the walls of small perforators are thickened and stiffened by GOM accumulation leading to stenosis.3 This results in a decrease in perforator diameter and compliance, which can lead to a higher pulsatility and lower flow.9 However, it remains arguable how this affects velocity, since the diameter change due to GOM accumulation in our population is unknown. Also, the vascular tree is complex and composed of arteries, veins and small perforators which are interconnected, but differently affected in CADASIL disease.4 Finally, a smaller vessel diameter leads to a larger Vmean underestimation which may partly explain the lower values in patients.10
Ndensity in the BG and NAWM in the CSO is not significantly different between patients and controls. This indicates that although the perforators show altered hemodynamics, this does not lead to a significant change in the number of detected perforators. However, the density of perforators with velocities below the detection threshold may be different.
Table 2 shows the comparison in CADASIL patients between NAWM and WMH in the CSO. Vmean, PI and Ndensity are not significantly different. This could indicate that perforator impairment in CADASIL patients is not merely or mainly present in the WMH, but has a widespread presence in the brain.
Conclusion
In CADASIL patients, the velocity in small perforating arteries in the CSO and BG is significantly lower and the pulsatility significantly higher compared to controls. In the CSO of patients, these differences are not limited to WMH but also present in NAWM. These results show that small vessel disease in CADASIL patients can now be detected non-invasively in the form of functional changes in the small vessels themselves.Acknowledgements
We acknowledge the support from the European Union's Horizon 2020 research and innovation programme under grant agreement 666881.References
1. Yamamoto Y, Craggs LJL, Watanabe A, et al. Brain microvascular accumulation and distribution of the NOTCH3 ectodomain and granular osmiophilic material in CADASIL. J Neuropathol Exp Neurol. 2013;72(5):416-431. doi:10.1097/NEN.0b013e31829020b5 2. Hack R, Rutten J. Summary Clinical characteristics. 2019:1-29. 3. Stojanov D, Aracki-Trenkic A, Vojinovic S, et al. Imaging characteristics of cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy (CADASIL). Bosn J Basic Med Sci. 2015;14(3):1-8. doi:10.17305/bjbms.2015.247 4. Kalimo H, Miao Q, Tikka S, et al. CADASIL: The Most Common Hereditary Subcortical Vascular Dementia. Future Neurol. 2008;3(6):683-704. 5. Ling C, Fang X, Kong Q, et al. Lenticulostriate Arteries and Basal Ganglia Changes in Cerebral Autosomal Dominant Arteriopathy With Subcortical Infarcts and Leukoencephalopathy, a High-Field MRI Study. Front Neurol. 2019;10(August):1-9. doi:10.3389/fneur.2019.00870 6. Geurts L, Biessels GJ, Luijten P, Zwanenburg J. Better and faster velocity pulsatility assessment in cerebral white matter perforating arteries with 7T quantitative flow MRI through improved slice profile, acquisition scheme, and postprocessing. Magn Reson Med. 2018;79(3):1473-1482. doi:10.1002/mrm.26821 7. Geurts LJ, Luijten PR, Klijn CJM, Zwanenburg JJM, Biessels GJ. Higher Pulsatility in Cerebral Perforating Arteries in Patients With Small Vessel Disease Related Stroke, a 7T MRI Study. Stroke. 2018;50(1):62-68. doi:10.1161/strokeaha.118.022516 8. Arts T, Siero J, Biessels GJ, Zwanenburg J. Method for vessel selection effects the outcome and reproducibility of velocity and pulsatility measures in cerebral penetrating arteries. In: Annual Meeting of the International Society of Magnetic Resonance. Montreal; 2019:#3264. 9. J. Gordon Betts, Kelly A. Young, James A. Wise, Eddie Johnson, Brandon Poe, Dean H. Kruse, Oksana Korol, Jody E. Johnson, Mark Womble PD. Blood Flow, Blood Pressure, and Resistance. In: Anatomy and Physiology. Houston, Texas: OpenStax; 2013. https://openstax.org/books/anatomy-and-physiology/pages/20-2-blood-flow-blood-pressure-and-resistance. 10. Bouvy WH, Geurts LJ, Kuijf HJ, et al. Assessment of blood flow velocity and pulsatility in cerebral perforating arteries with 7-T quantitative flow MRI. NMR Biomed. 2016;29(9):1295-1304. doi:10.1002/nbm.3306Figures
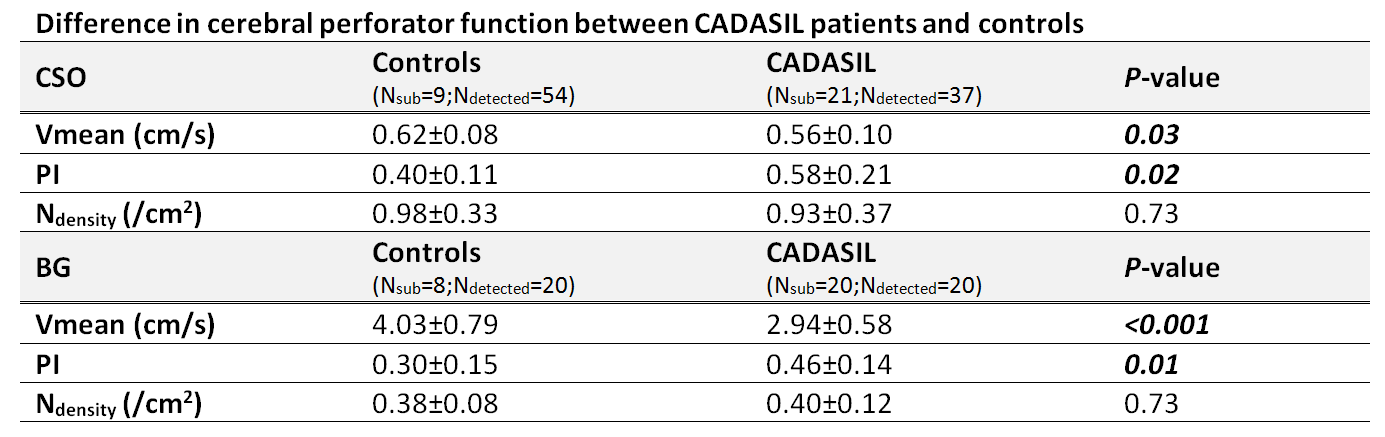
Table 1: Comparison between controls and CADASIL patients for Vmean,
PI and Ndensity in the BG and in normal appearing white matter of the
CSO. Results are average values±standard deviations
of all subjects combined. CSO, centrum semi-ovale; BG, basal ganglia; Vmean,
mean velocity over the cardiac cycle; PI, pulsatility index; Ndensity,
number of detected perforators per cm2 of mask; Nsub, number of included subjects; Ndetected,
mean number of detected perforators. Bold P-values are significant.
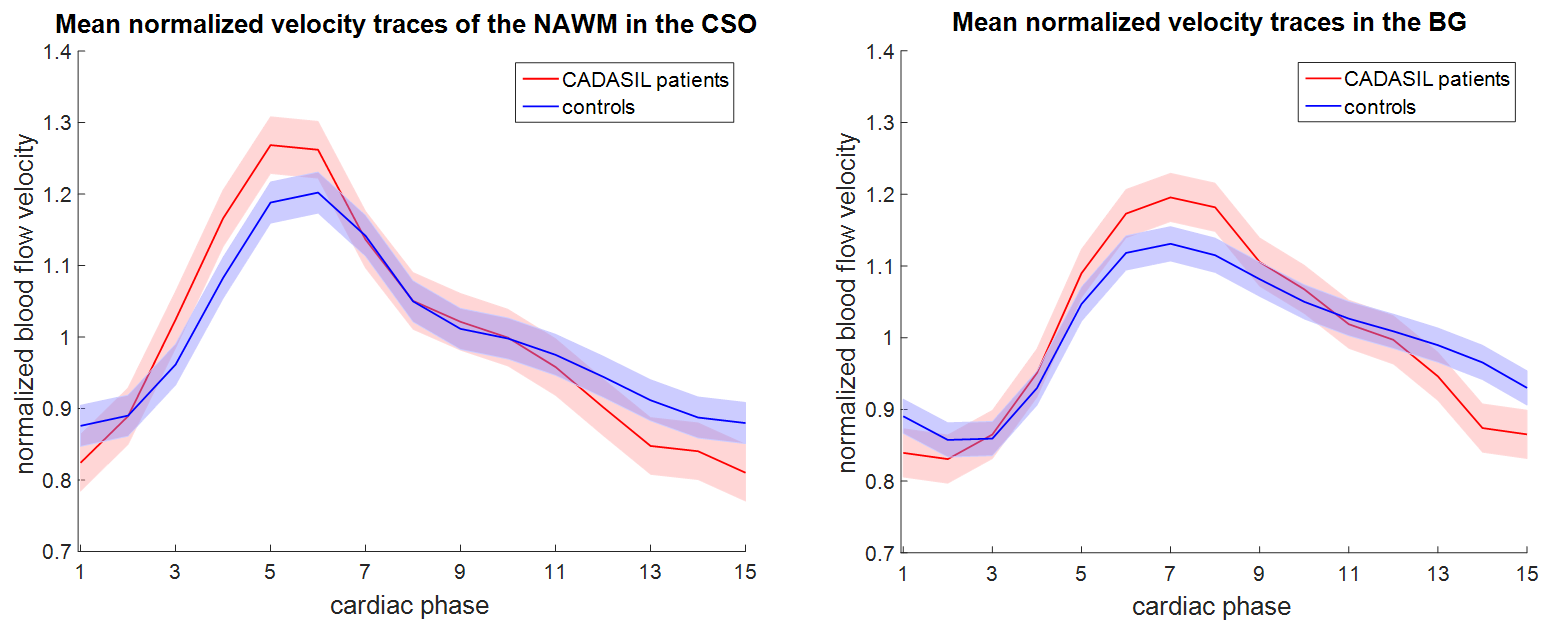
Figure 1: Mean normalized (division by the mean) velocity traces
of all detected perforators combined, interpolated to the maximum number of
occurring cardiac phases. Traces of CADASIL patients and controls in the basal
ganglia (BG) and normal appearing white matter (NAWM) of the centrum semi-ovale
(CSO) are shown. Shaded regions indicate ±standard error of the mean.

Table 2: Comparison within CADASIL patients between normal appearing
white matter (NAWM) and white matter hyperintensities (WMH) for Vmean,
PI and Ndensity in the CSO. Results
are average values±standard deviations of all subjects combined. CSO, centrum
semi-ovale; BG, basal ganglia; Vmean, mean velocity over the cardiac
cycle; PI, pulsatility index; Ndensity, number of detected
perforators per cm2 of mask; Nsub, number of included
subjects; Ndetected, mean number of detected perforators.