1666
White matter hyperintensity features in Neuropsychiatric Systemic Lupus Erythematosus: a retrospective case-control study.1Department of Radiology, Leiden University Medical Center, Leiden, Netherlands, 2Department of Rheumatology, Leiden University Medical Center, Leiden, Netherlands
Synopsis
Systemic Lupus Erythematosus (SLE) often presents with neuropsychiatric (NP) symptoms. These symptoms can be directly associated with SLE (NP-SLE) or not (non-NP-SLE). We investigated whether white matter hyperintensity (WMH) features (such as type, volume and shape) may contribute to the diagnosis of NP-SLE. Patients with NP-SLE more often had deep WMH (DWMH) compared to patients with non-NP-SLE. There were no significant differences in WMH volume and shape features between NP-SLE patients compared to non-NP-SLE patients. In conclusion, NP-SLE patients more often had DWMH compared to non-NP-SLE patients and this may help in the diagnostic process of NP-SLE.
INTRODUCTION
Systemic Lupus Erythematous (SLE) is an autoimmune disease that may present with a broad spectrum of neuropsychiatric (NP) symptoms1,2. Attribution of NP symptoms directly to the disease (NP-SLE), or to an alternative etiology such as side effects of medication or the involvement of other organs (non-NP-SLE)3 is highly uncertain, as no gold standard exists. Currently, MRI features can only contribute in a limited way in the diagnostic process. Discovering MRI biomarkers may help in the diagnostic process.White matter hyperintensities (WMH) in the brain are related to both NP-SLE and non-NP-SLE4,5. WMH lesions are currently mainly expressed in terms of volume, but this does not contribute to distinguishing between different etiologies6. On the other hand, type and shape of WMH lesions may provide additional etiological information7.
In this retrospective study, we investigated whether conventional (volume) and advanced WMH (type and shape) features are different in NP-SLE patients versus non-NP-SLE patients.
MATERIAL AND METHODS
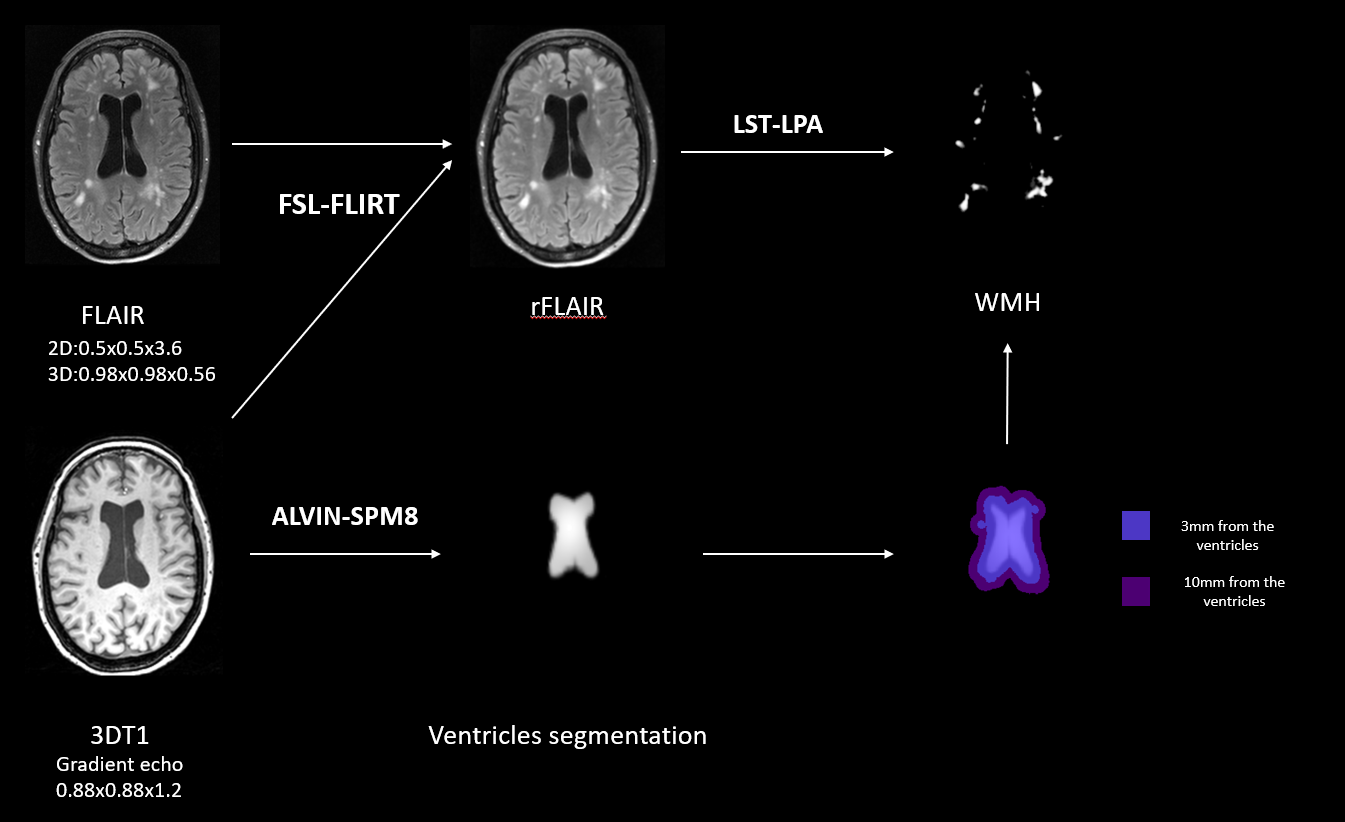
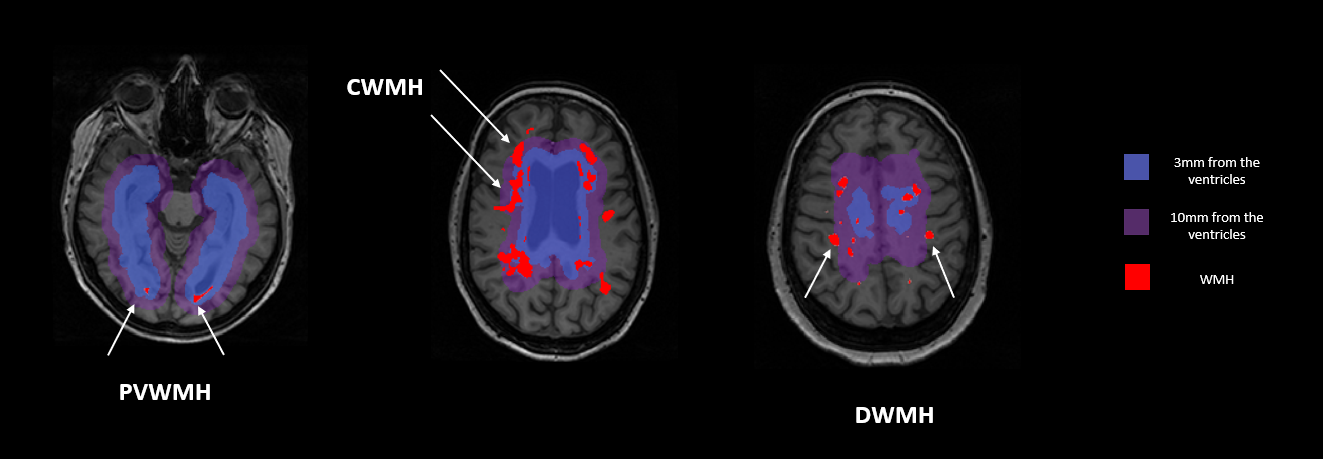
130 patients were included in this study: 29 with NP-SLE and 101 with non-NP-SLE. Patients were diagnosed following a one-day standardized evaluation comprising a combination of multidisciplinary medical assessments, including a brain MRI scan on a Philips Achieva 3T MRI scanner. The MRI acquisition protocol included 3D T1-weighted and fluid-attenuated inversion recovery (FLAIR) sequences.The FLAIR images were registered to the 3D T1-weighted images8. WMH segmentations were performed on the registered FLAIR and thresholded on a probability of 0.29. Lateral ventricular segmentation was performed on the 3D T1 image or on the registered FLAIR to the T110. Figure 1 shows the image-processing pipeline. The Periventricular WMH (PVWMH) type was assigned to WMH within 10 mm from the lateral ventricles. The Confluent WMH (CWMH) type was assigned to PVWMH that extended to more than 10 mm from the lateral ventricles. The Deep WMH (DWMH) type was assigned to WMH that were located >10mm from the lateral ventricles. Figure 2 shows WMH types. WMH shape features were calculated from the WMH segmentation. Solidity, convexity, concavity index and fractal dimension were used for PVWMH and CWMH. Eccentricity and fractal dimension were used for DWMH10. Mean or median values per feature were calculated per patient.
Group differences in WMH volumes, WMH type and WMH shape features between groups were studied by linear or logistic regression analyses corrected for age and gender and for WMH volume additionally for total intracranial volume (TIV). All analyses were performed in IBM SPSS version 23.
RESULTS
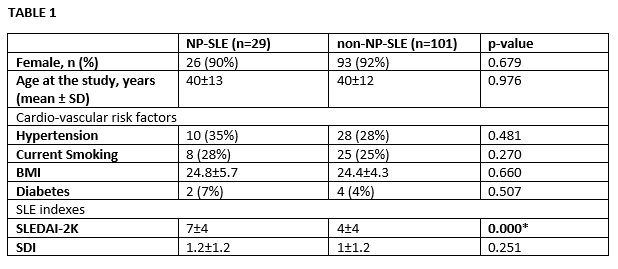
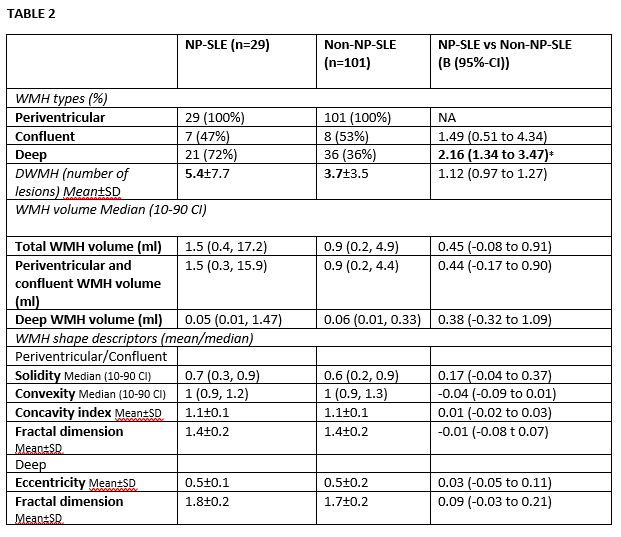
Table 1 shows the characteristics of the patient population. No significant differences between the two patient groups (NP-SLE and non-NP-SLE) were found, except for the SLE disease activity index (SLEDAI), which was higher in NP-SLE.The DWMH type was more often present in NP-SLE patients compared to non-NP-SLE patients (Table 2). Although NP-SLE patients showed a higher number of deep lesions per patients, a higher volume of total WMH and PV/CWMH compared to non-NP-SLE patients, these differences were not statistically significant (Table 2). No significant between group differences were found in WMH shape features for both PV/CWMH and DWMH (Table 2).
DISCUSSION AND CONCLUSION
We found that NP-SLE patients more often had deep white matter hyperintensities compared to non-NP-SLE patients.Studying WMH features besides volumes is relatively new10 and this is the first study on SLE patient populations to our knowledge. This approach may lead to improve our understanding on the etiology and underlying prognostic information of diseases, as well as to differentiate between WMH of presumed vascular origin from other causes11. In particular, previous brain histopathological studies showed that different type and features of WMHs are associated with different brain parenchymal changes12.
It has been shown that DWMH lesions have different functional, microstructural and clinical characteristics compared to PVWMH lesions. In particular, DWMH lesions are related to disruption of short connections in the white matter, are more heterogeneous compared to PVWMHs, and are characterized by more axonal loss, vacuolization and arteriolosclerosis. DWMH lesions are also related to more hypoxic/ischemic changes compared to PVWMH13.
In conclusion, we showed that NP-SLE patients more often had deep white matter hyperintensities compared to non-NP-SLE patients. This finding may contribute to the diagnosis of NP-SLE and this may suggest that NP symptoms are related more to DWMH load than load of other WMH types. Furthermore, there may be a different underlying etiology of WMH lesions between NP-SLE and non-NP-SLE patients. Further studies are needed to fully understand the relation between DWMH and NP symptoms.
Acknowledgements
No acknowledgement found.References
1. Arbuckle, M.R., McClain, M.T., Rubertone, M.V., Scofield, R.H., Dennis, G.J., James, J.A. et al. (2003). "Development of autoantibodies before the clinical onset of systemic lupus erythematosus." N Engl J Med. 2003;349(16):1526-1533.
2. Brey, R.L., Holliday, S.L., Saklad, A.R., Navarrete, M.G., Hermosillo-Romo, D., Stallworth, C.L. et al. (2002)." Neuropsychiatric syndromes in lupus: prevalence using standardized definitions ." Neurology (2002); 58(8):1214-1220.
3. Hanly JG, Kozora E, Beyea SD, Birnbaum J. Review: Nervous System Disease in Systemic Lupus Erythematosus: Current Status and Future Directions. Arthritis Rheumatol. 2019 Jan;71(1):33-42.
4. Magro-Checa C, Kumar S, Ramiro S, Beaart-van de Voorde LJ, Eikenboom J, Ronen I, de Bresser J, van Buchem MA, Huizinga TW, Steup-Beekman GM. Are serum autoantibodies associated with brain changes in systemic lupus erythematosus? MRI data from the Leiden NP-SLE cohort. Lupus. 2019 Jan;28(1):94-103.
5. Yeoh H, Lee JY, Lee YJ, Park DW, Kim TY, Ahn GY, Bae SC, Kim YS, Kim HY, Kim CK, Kim JY, Kim H, Han JW. Relationship between cerebral microbleeds and white matter MR hyperintensities in systemic lupus erythematosus: a retrospective observational study. Neuroradiology. 2019 Mar;61(3):265-274.
6. Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, Lindley RI, O'Brien JT, Barkhof F, Benavente OR, Black SE, Brayne C, Breteler M, Chabriat H, Decarli C, de Leeuw FE, Doubal F, Duering M, Fox NC, Greenberg S, Hachinski V, Kilimann I, Mok V, Oostenbrugge Rv, Pantoni L, Speck O, Stephan BC, Teipel S, Viswanathan A, Werring D, Chen C, Smith C, van Buchem M, Norrving B, Gorelick PB, Dichgans M; STandards for ReportIng Vascular changes on nEuroimaging (STRIVE v1). Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013 Aug;12(8):822-38.
7. Artero S, Tiemeier H, Prins ND, Sabatier R, Breteler MM, Ritchie K. Neuroanatomical localisation and clinical correlates of white matter lesions in the elderly. J Neurol Neurosurg Psychiatry. 2004 Sep;75(9):1304-8.
8. M. Jenkinson, P.R. Bannister, J.M. Brady, and S.M. Smith. Improved optimisation for the robust and accurate linear registration and motion correction of brain images. NeuroImage, 17(2):825-841, 2002.
9. Schmidt P. PhD thesis, Ludwig-Maximilians-Universität München; 2017. Chapter 6.1: Bayesion inference for structured additive regression models for large-scale problems with applications to medical imaging.
10. Kant IMJ, Mutsaerts HJMM, van Montfort SJT, Jaarsma-Coes MG, Witkamp TD, Winterer G, Spies CD, Hendrikse J, Slooter AJC, de Bresser J; BioCog Consortium. The association between frailty and MRI features of cerebral small vessel disease. Sci Rep. 2019 Aug 5;9(1):11343.
11. de Bresser J, Kuijf HJ, Zaanen K, Viergever MA, Hendrikse J, Biessels GJ; Utrecht Vascular Cognitive Impairment Study Group. White matter hyperintensity shape and location feature analysis on brain MRI; proof of principle study in patients with diabetes. Sci Rep. 2018 Jan 30;8(1):1893.
12. Ghaznawi R, Geerlings MI, Jaarsma-Coes MG, Zwartbol MH, Kuijf HJ, van der Graaf Y, Witkamp TD, Hendrikse J, de Bresser J; SMART Study Group. The association between lacunes and white matter hyperintensity features on MRI: The SMART-MR study. J Cereb Blood Flow Metab. 2018 Sep 11:271678X18800463.
13. Griffanti L, Jenkinson M, Suri S, Zsoldos E, Mahmood A, Filippini N, Sexton CE, Topiwala A, Allan C, Kivimäki M, Singh-Manoux A, Ebmeier KP, Mackay CE, Zamboni G. Classification and characterization of periventricular and deep white matter hyperintensities on MRI: A study in older adults. Neuroimage. 2018 Apr 15;170:174-181.
Figures