1664
Quantitative evaluation of magnetic susceptibility effects in carotid artery CE-MRA with different injected flow rate of contrast medium1Departments of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2MR Collaborations, Siemens Healthcare Ltd, Shenzhen, China
Synopsis
Contrast-enhanced magnetic resonance angiography (CE-MRA) is the main modality used for assessing carotid artery stenosis in the vessel lumen, but limited to the susceptibility artifact, which would result in artifactual stenosis of artery adjacent to the subclavian vein on the injection side of contrast medium. This study aims to explore the quantitative influence of different injected flow rates of contrast medium on the susceptibility effect in the subclavian arterial image of CE-MRA on a 3T MR scanner. The result indicated that the magnetic susceptibility artifact can be reduced by improving the injection speed of contrast agent
Introduction
Carotid artery stenosis, induced by carotid atheromatous plaques has a relatively high morbidity in most cases(1). Currently, contrast-enhanced magnetic resonance angiography (CE-MRA) is the main modality used for assessing carotid artery stenosis in the vessel lumen(2-4), but limited to the susceptibility artifact due to its sensitivity to the T2* shortening effect with three-dimensional spoiled gradient echo sequence (3D-GRE),which would result in artifactual stenosis of artery adjacent to the subclavian vein on the injection side of contrast medium.(5). This study aims to explore the quantitative influence of different injected flow rates of contrast medium on the susceptibility effect in the subclavian arterial image of CE-MRA on a 3T MR scanner.Methods
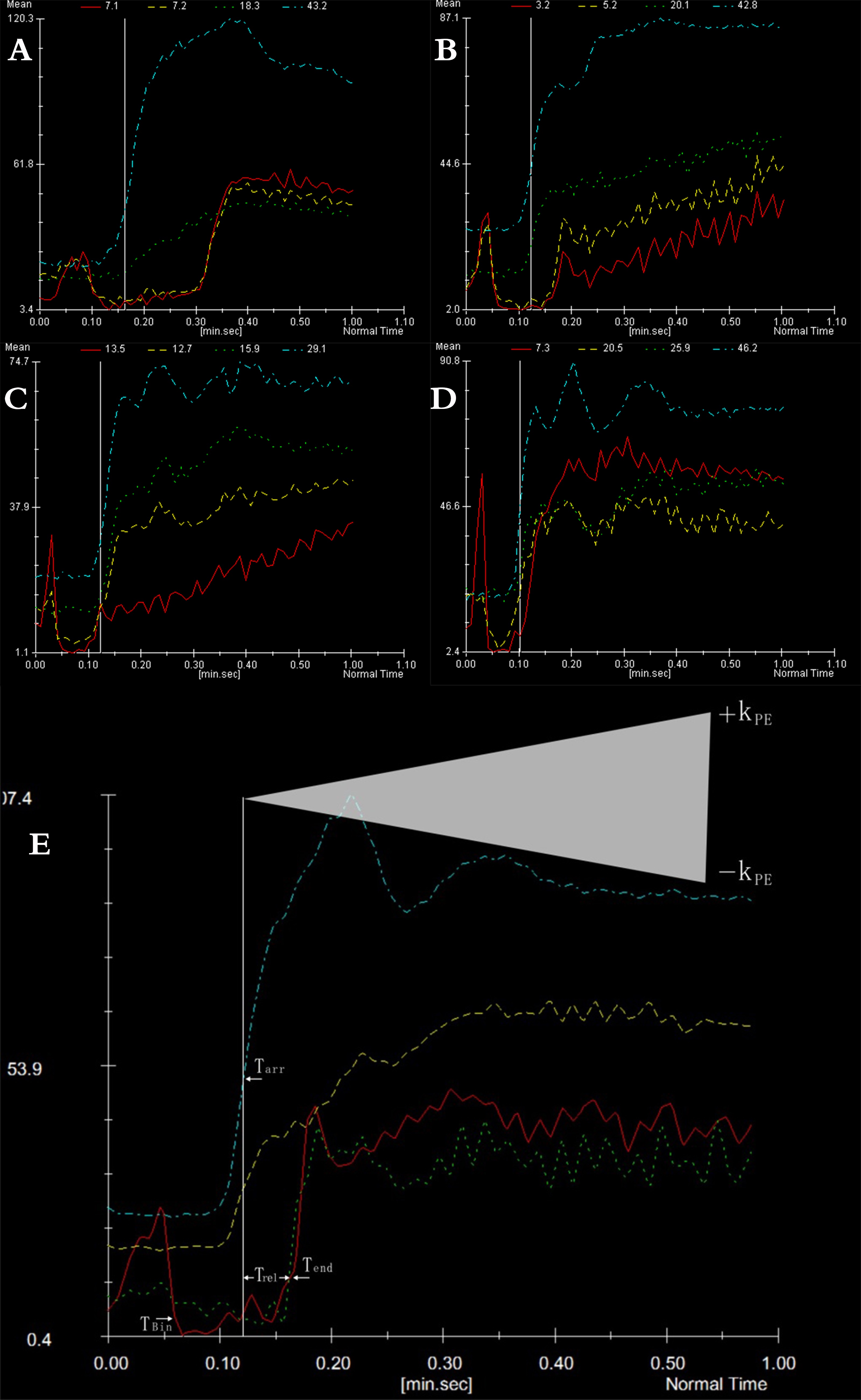
All the IRB-approved MR examinations were performed on a 3 Tesla MR scanner (Magnetom Skyra, Siemens Medical Solution,Erlangen, Germany) using commercially available 12-channel head coil and 8-channel neck phased-array coil. 80 patients excluded with cardiac insufficiency were enrolled in this study and randomly separated into 4 groups (A, B, C, and D) to undergo neck contrast-enhanced MR examination. All patients underwent carotid artery real-time bolus tracking using CARE bolus system, and Care bolus examination was performed based on the vascular scout view to measure the relationship between time and signal intensity. An electronic power injector (Spectris; Medrad, Pittsburgh, Pa) was used for contrast material injection with 20 ml of Magnevist solution (Magnevist, 0.5 mmol/ml), and 15 ml of normal saline via the right ulnar vein. The injection rate for the defined four groups were 1 ml/s for group A, 2 ml/s for group B, 3 ml/s for group C, and 4 ml/s for group D. Coronal MR examinations was performed with the contrast agents at different injection rates using the following parameters: TR=44.3 ms, TE=1.56 ms, bandwidth=400 Hz/pixel, FOV=400 mm, slice thickness=40 mm, flip angle =25° , imaging matrix =256x180. The time-signal intensity curve of the couple subclavian arteries, subclavian vein, and the carotid artery were obtained. The duration of susceptibility effect of subclavian arteries and its ipsilateral veins during intravenous injection were calculated, and the reference time of susceptibility effect disappearance (Trel) was measured for comparison. The difference in the susceptibility effect at different injected rates of contrast medium was determined using One-way ANOVA variance analysis. Statistical significance was defined as p < 0.05.Results
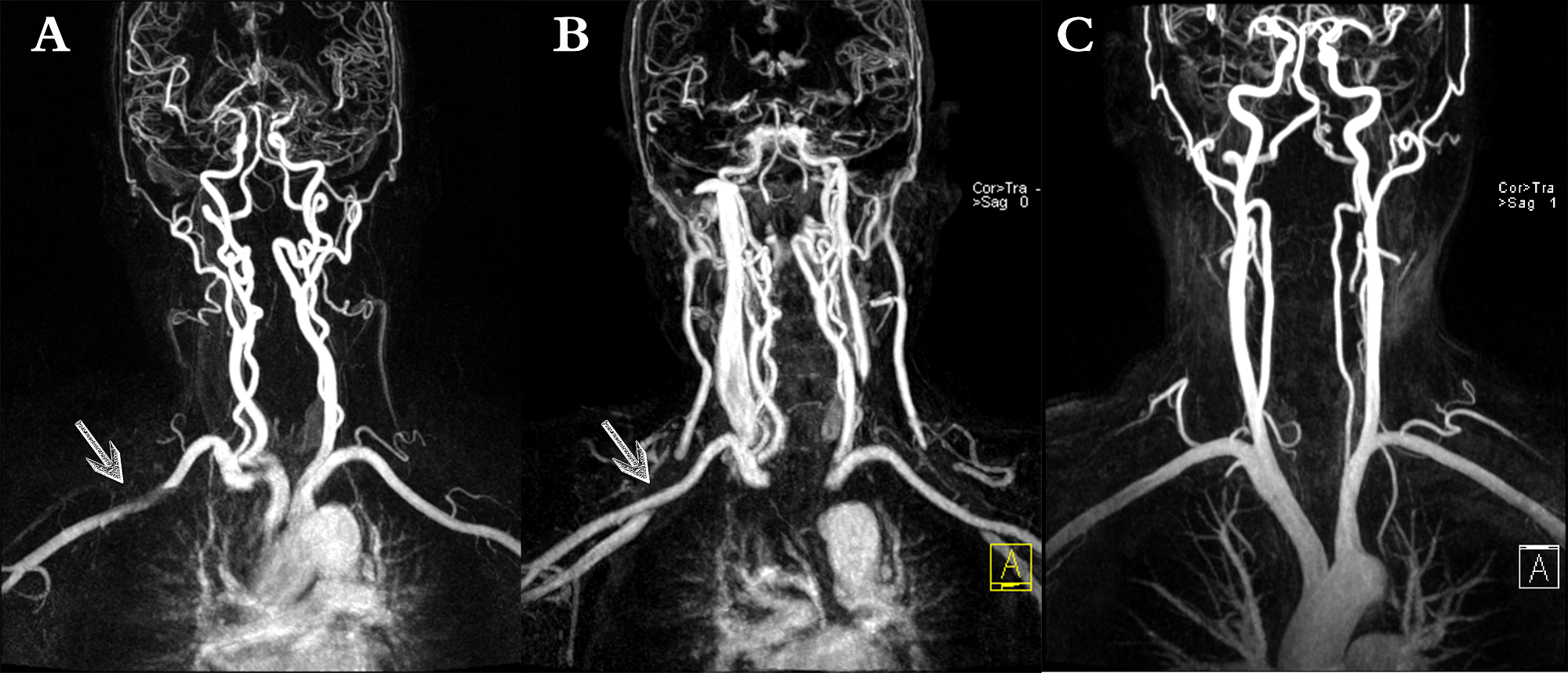
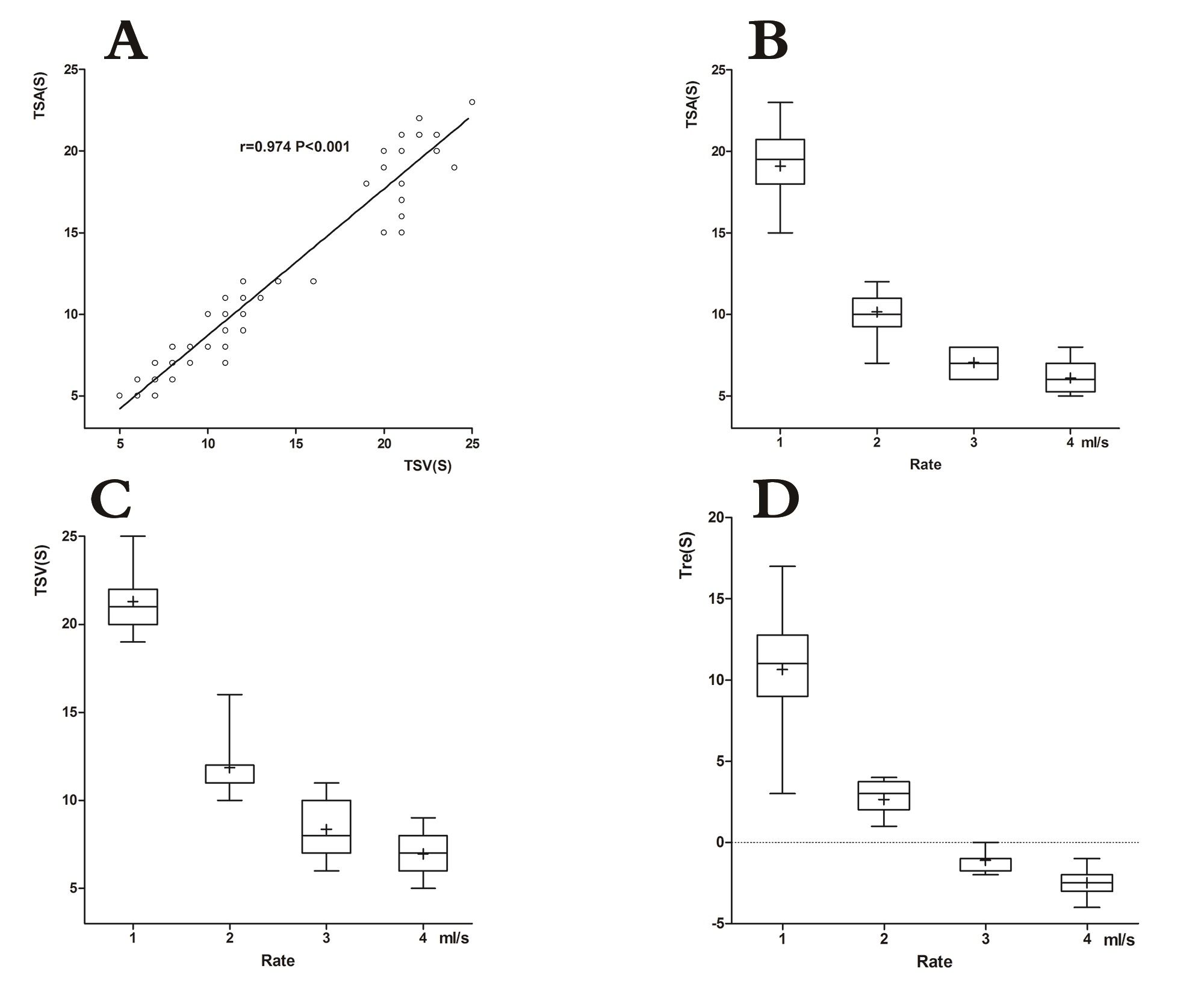
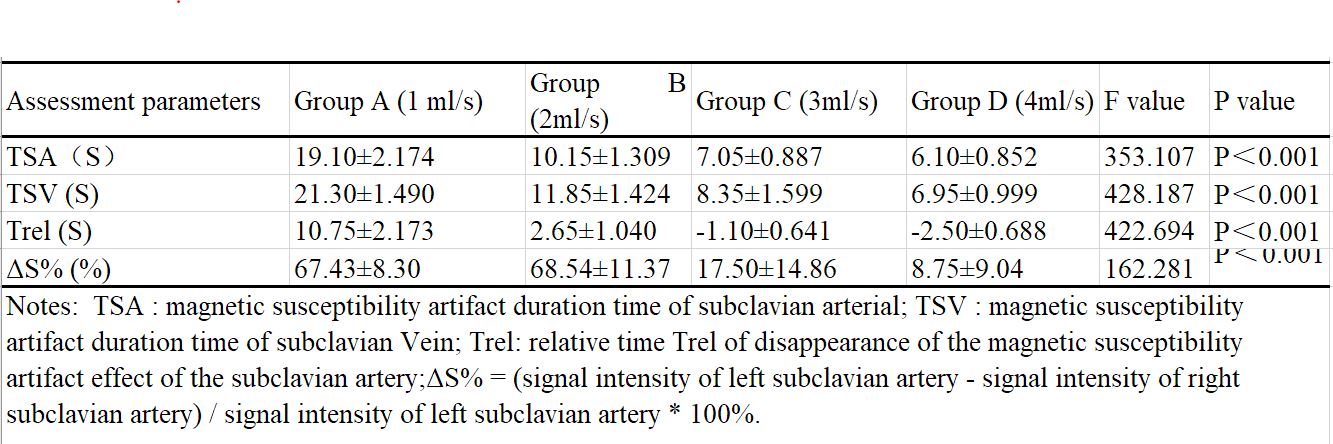
As the injection rate of contrast medium was increased from 1.0 ml/s to 4.0 ml/s, there were significant differences at the duration of susceptibility effect at subclavian arteries among these 4 groups (p<0.01)(Table 1). Furthermore, there was a negative correlation between the duration of susceptibility effect and the rate of injection (Correlation coefficient rs =-0.918, p<0.001)(Fig 3). There were significant differences in reference time (Trel) among the 4 groups at different injected rates of contrast medium (p<0.01), and while the injection rate was higher, the reference time Trel was smaller(Fig 1). Furthermore, the susceptibility artifact can be reduced with the injection of contrast agent at the injected rate ≥3ml/s(Fig 2).Discussion and Conclusion
The susceptibility artifact that caused false positive stenosis isolated to the subclavian artery in carotid artery CE-MRA was due to the highly concentrated gadolinium in the adjacent subclavian vein. This study sought to study the influence of the first-pass magnetic susceptibility artifact in neck CE-MRA using care bolus analysis, which clearly revealed the influential mechanism of the magnetic susceptibility artifact. The result indicated that the magnetic susceptibility artifact can be reduced by improving the injection speed of contrast agent, and the injected rate over 3 ml/s could obviously improve the issues of the first-pass magnetic susceptibility effect. Characterized with its excellent operability, repeatability and practicability, its application for controlling image quality can be promoted.Acknowledgements
Many thanks to MR Collaborations, Siemens Healthcare, Shenzhen, China.Many thanks to Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology.References
1.Rothwell PM, Coull AJ, Silver LE, et al. Population-based study of event-rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet 2005;366(9499):1773-1783.
2.Momjian-Mayor I, Burkhard P, Murith N, et al. Diagnosis of and treatment for symptomatic carotid stenosis: an updated review. Acta Neurol Scand 2012;126(5):293-305.
3.Kakisis JD, Avgerinos ED, Antonopoulos CN, Giannakopoulos TG, Moulakakis K, Liapis CD. The European Society for Vascular Surgery guidelines for carotid intervention: an updated independent assessment and literature review. Eur J Vasc Endovasc Surg 2012;44(3):238-243.
4.Zhang H, Maki JH, Prince MR. 3D contrast-enhanced MR angiography. J Magn Reson Imaging 2007;25(1):13-25.
5.Anzalone N, Scotti R, Iadanza A. MR angiography of the carotid arteries and intracranial circulation: advantage of a high relaxivity contrast agent. Neuroradiology 2006;48 Suppl 1:9-17.
Figures