1660
The application of High-Resolution Vessel Wall MRI(HR-VW-MRI) in determining the stability of intracranial MCA and BA plaques1Jilin University First Hospital, Changchun, China, 2Philips healthcare, Guangzhou, China
Synopsis
The stability of intracranial of the middle cerebral artery(MCA) and basilar artery( BA) plaques related to the stroke events is a crucial issue. However, the discrimination of the plaque’s stability could be rather challenging. Compared with traditional imaging methods such as CTA, MRA or DSA, high-resolution vessel wall MR imaging(HR-VW-MRI) method could demonstrate the abnormality of the vessel wall .It could also potentially evaluate the stability of the intracranial artery. This study aims to compare HR-VW-MRI’s characteristic features of MCA plaque with BA plaque, and to figure out the relationship between plaques’ imaging features with the stroke events
Purpose
To study HR-VW-MRI imaging characteristics of intracranial MCA and BA plaques, and discriminate the stability of early intracranial MCA and BA plaques. To improve the detection rate of symptomatic intracranial artery plaquesMaterial and Methods
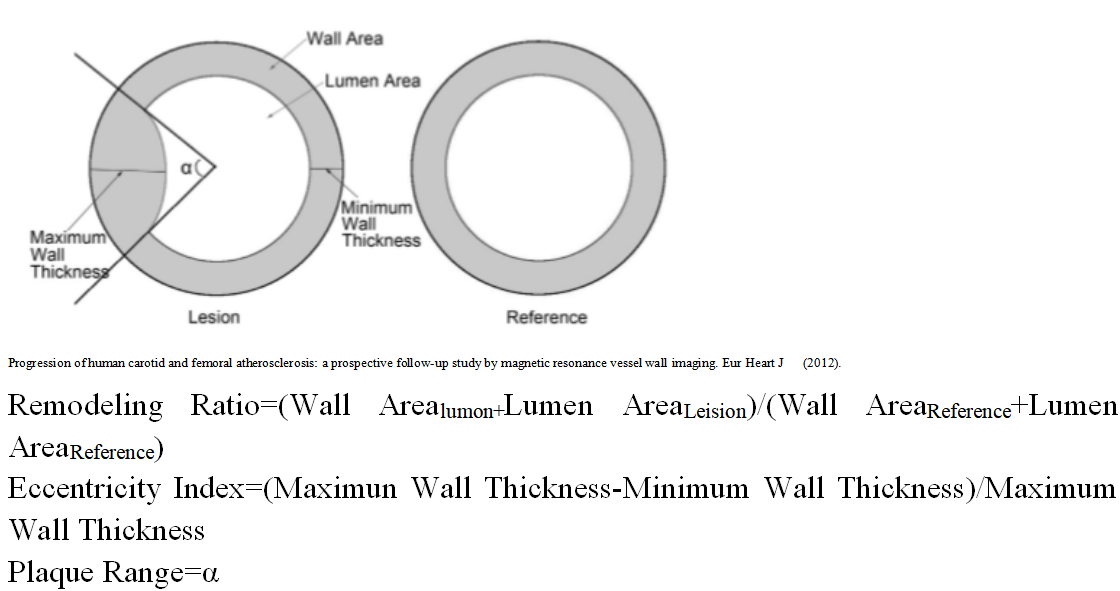
87 patients with acute ischemic stroke who visited the department of neurology of 1st Hospital of Jilin University from March 2017 to March 2019 were collected in the study. General data of patients were recorded. All the patients were performed with the HR-VW-MRI protocol, and the imaging characteristic features were discriminated and measured by two experienced neuroimaging doctors who did not know the patients’ information. All of the VWMRI examinations were performed on a 3 T Siemens Trio MR scanner (Siemens Healthcare, Erlangen, Germany). Two-dimensional T2-weighted VWMRI was obtained perpendicular to the long axis of the BA or the M1 segments of the relevant MCA and contralateral MCA. All patients had at least one MCA or BA plaque identified with an early or mild (< 50% stenosis) atherosclerosis with an MCA or BA plaque. The remodelling ratio, eccentricity index and plaque range (computational formula see Figure 1)of MCA and BA plaques were compared using MRI-PlaqueViewTM, and multilevel analysis was performed. SPSS 19.0 statistical software (SPSS, IBM, West Grove, PA, USA) was used for statistical analysis of the data. The quantitative data were expressed as mean SD. Qualitative data are expressed as quantity and percentage. For quantitative data, t-test (for normally distributed data) or Mann-Whitney U test was used, and a chi-square test was used for qualitative data. P<0.05 was considered statistically significant.Results
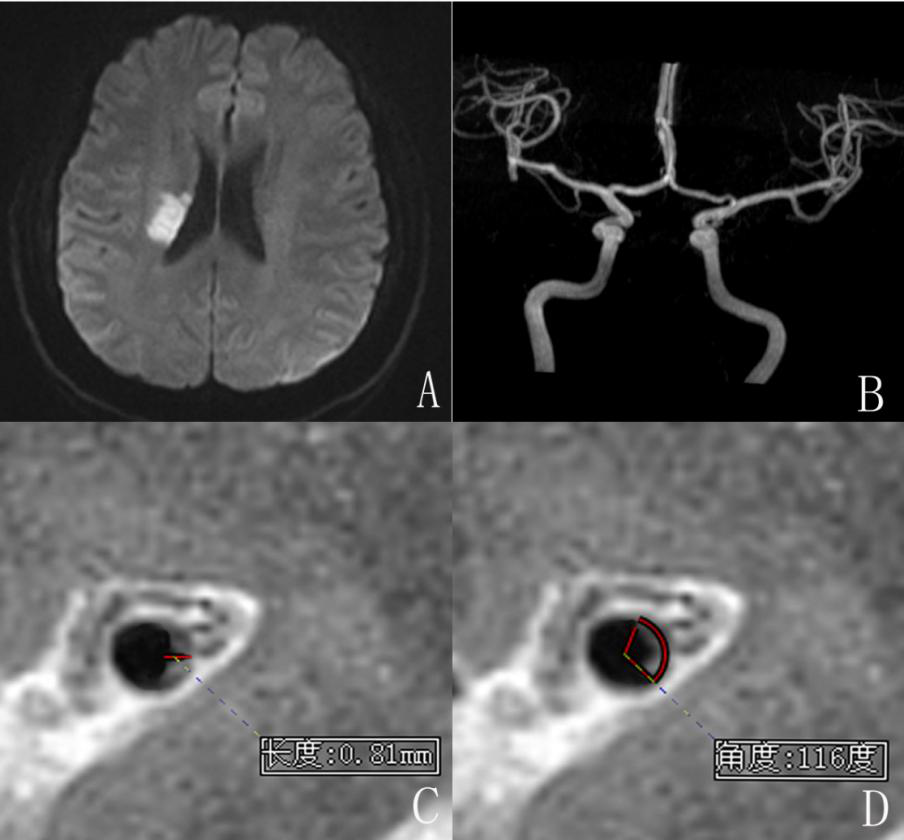
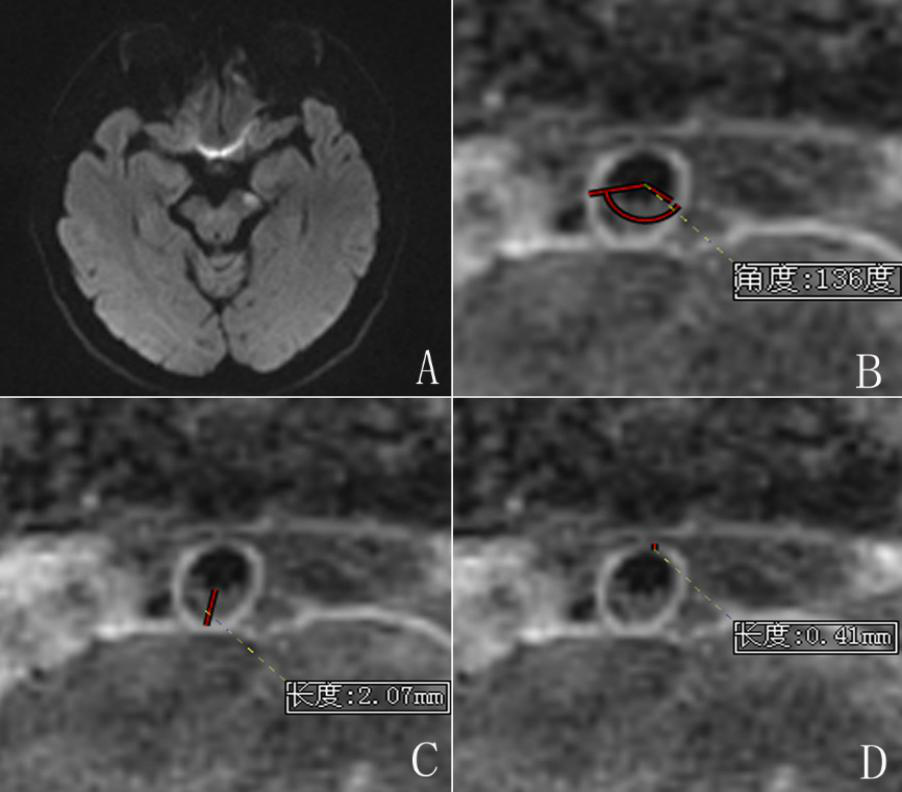
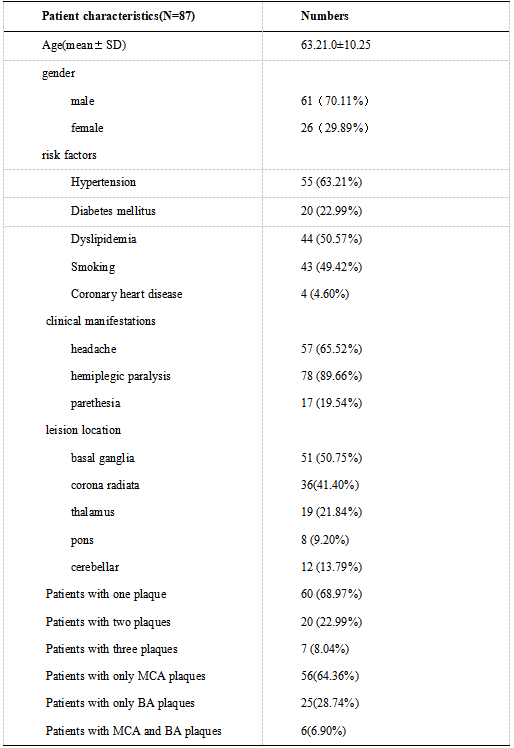
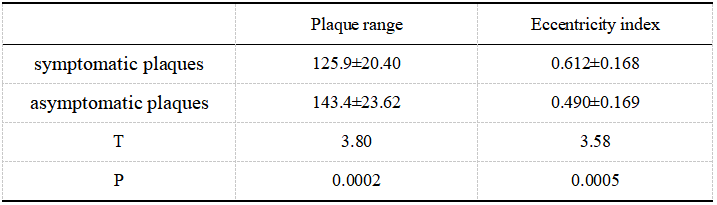
A total of 87 patients with 116 plaques were included in this study. The patients’ characteristics are demonstrated in Table 1( Table 1). There were 80 plaques located in the MCA and 36 plaques found in the BA. Among the 86 MCA plaques, 22 were classified as symptomatic, 7 were indeterminate, and 51 were asymptomatic. Among the 36 BA plaques, 13 were symptomatic, 14 were uncertain, and 9 were asymptomatic. The measurements of the magnetic resonance images of the vessel wall of MCA and BA are shown in Figure 2 and Figure 3. Among all plaques, the eccentricity index of symptomatic plaques was 0.612±0.168, while that of uncertain and asymptomatic plaques was 0.490±0.169 (p=0.0005). The plaque range in the symptomatic plaques was 125.9 ±20.40, while that of uncertain and asymptomatic plaques was 143.4 ±23.62 (p < 0.001)(Table 2). That meant the symptomatic plaques had much higher eccentricity index and much much smaller plaque range.Discussion
Traditional imaging methods such as CTA, MRA or DSAcould only show the stenosis or dilation of the vessel lumen, while could not demonstrate the vessel wall and account for the reasons of the vessel stenosis or dilation1. As HR-VW-MRI method could show the vessel wall as well as the lumen, the use of HR-VW-MRI has dramatically improved the understanding of the pathophysiology of atherosclerosis2. The symptomatic plaques that could cause ischemic stroke or transient ischemic attack, should be differentiate from asymtomatic plaques and need more clinical intervention and attention. The formula deduced from the remodeling model suggested that the remodelling ratio is positively accompanied by the plaque burden and inversely accompanied with degree of the stenosis3. Therefore, to assess the remodelling ratio differs between MCA and BA, degree of stenosis or plaque burden have to be considered. Previous studies showed that positive remodelling was related with the symptomatic plaques4. However, this was not accordance with our study. In our study we firstly demonstrate thateccentricity index and plaque range had no significant difference in discriminating the symptomatic plaques between MCA and BA. Secondly, the eccentricity index and plaque range had no significant difference in the asymptomatic and uncertain plaques of MCA and BA. Lastlybut not least, the symptomatic plaques had much higher eccentricity index and much much smaller plaque range.Those findings were beneficial for guiding significance to existing clinical guidelines. Another reason in point, different plaque analysis and various statistical analysis may account for the controversial results. A multi-center clinical trial should be performed to validate our conclusion.Conclusion:
There was no significant difference between the included MCA and BA symptomatic plaques and other plaques in this study (P>0.05). In this study, the characteristics of MCA and BA plaques in the early and middle stages included in the group were manifested as the symptomatic plaques prone to stroke with higher eccentricity index and smaller plaque range, which to some extent could reflect the stability characteristics of MCA and BA plaques in northern China.Acknowledgements
No acknowledgement found.References
1. Chen S, Zhao H, Li J, et al. Evaluation of carotid atherosclerotic plaque surface characteristics utilizing simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) technique[J]. J MagnReson Imaging. 2018, 47(3): 634-639.
2. Holmstedt C A, Turan T N, Chimowitz M I. Atherosclerotic intracranial arterial stenosis: risk factors, diagnosis, and treatment[J]. Lancet Neurol. 2013, 12(11): 1106-1114.
3. Bianda N, Di Valentino M, Périat D,Segatto JM, Oberson M, et al. Progression of human carotid and femoral atherosclerosis: a prospective follow-up study by magnetic resonance vessel wall imaging. Eur Heart J 2012 Jan;33(2):230-72019.
4. Dieleman N, Yang W, Abrigo J M, et al. Magnetic Resonance Imaging of Plaque Morphology, Burden, and Distribution in Patients With Symptomatic Middle Cerebral Artery Stenosis[J]. Stroke. 2016, 47(7): 1797-1802
Figures