1657
Evaluating collateral circulation and its association with clinical outcomes in patients with ischemic stroke using random vessel-encoded ASL1Radiology, Henan Provincial People's Hospital, Zhengzhou, China, 2Henan Key Laboratory of Neurological Imaging, Zhengzhou, China, 3MR Collaboration, Siemens Healthcare Ltd., Beijing, China, 4Stevens Neuroimaging Informatics Institute, Department of Neurology, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States
Synopsis
This study aimed to explore the clinical value of random vessel-encoded arterial spin labeling (rVE-ASL) in evaluating the collateral status as well as its association with clinical outcomes in patients with ischemic stroke. Results suggested that the rVE-ASL findings were consistent with DSA/CTA findings in characterizing collateral flows and poor collateral flows evaluated by rVE-ASL were associated with poor outcomes. The rVE-ASL could be a potentially useful tool to assess the cerebral collateral circulation in patients with ischemic stroke and predict the clinical outcome.
Introduction
Precise evaluation of cerebral collateral circulation plays an important role in individualized management in ischemic stroke. 1 Random vessel-encoded ASL (rVE-ASL) 2,3 as a novel ASL technique is capable of depicting perfusion vascular territories as well as corresponding feeding arteries, which has potential to evaluate the collateral status in ischemic stroke. This technique may offer the opportunity to rephrase the individualized management of each patient with ischemic stroke, based on the evaluation of cerebral collateral circulation. The purpose of this study was to investigate the clinical utility of rVE-ASL in evaluating cerebral collateral circulation and study its association with clinical outcomes in patients with ischemic stroke.Methods
The patients with ischemic stroke who underwent reperfusion therapies were imaged on a 3T MAGNETOM Prisma scanner (Siemens Healthcare, Erlangen, Germany) with a 64-channel head-neck coil. The rVE-ASL was performed using a single-shot 3D GRASE sequence with background suppression (BS) on each patient with the following parameters: FOV= 256 × 256 mm2, matrix size = 64 × 64, TE/TR = 22/3000 ms, 12 slices with slice thickness of 8 mm, 60 pairs of encoding steps with random orientation, phase and wavelength and two additional pairs of global label/control, leading to a total scan time of 6:12 mins. The locations of feeding arteries were identified by the correlation coefficient (CC) between the acquired perfusion signal and a database of predicted signal distributions. The corresponding perfusion territorial maps were subsequently generated based on the highest CC in each voxel. Each patient also had digital subtraction angiography (DSA) or CT angiography (CTA) scan as a reference for collateral evaluation. Two radiologists independently evaluated the collaterals in the left intracranial carotid artery (ICA), right ICA, and basilar artery territories on rVE-ASL and DSA/CTA images according to the following scoring criteria: 0: poor, no collateral circulation; 1: intermediate, partial collateral flow to the ischemic region; 2: good, full collateral flow to the site of occlusion; 3: normal antegrade flow. The neurologists recorded the modified Rankin score (mRS) at 3 months. The Kappa test was performed to evaluate the agreement between DSA/CTA score and rVE-ASL score, and Spearman rank correlation test was performed to explore the relationship between rVE-ASL score and mRS, using SPSS 26.0 (IBM Corp., Armonk/NY, US). P < 0.05 was considered statistically significant.Results
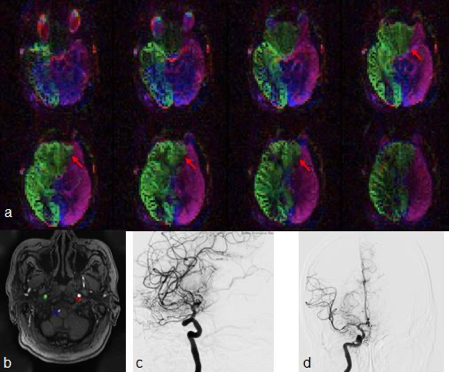
10 patients were enrolled in this study. 7 of them underwent DSA, and 3 of them underwent CTA. The vascular territorial maps using rVE-ASL were calculated for each patient. Figure 1 displays the perfusion territorial map (Fig 1a), locations of feeding arteries (Fig 1b) and DSA (Fig 1c, d). The k-coefficient of 0.68 indicated good agreement (P = 0.00). The rVE-ASL score was negatively correlated with mRS (P = 0.001, r = -0.87).Discussion
Over the past decade, the importance of cerebral collateral circulation has drawn much attention, which is associated with the efficacy of reperfusion therapies, the hemorrhagic transformation, the volume of infarction, and the risk of recurrence in ischemic stroke. 1 Although DSA is the gold standard for evaluating intracranial collateral circulation, it requires ionizing radiation and potentially toxic exogenous contrast agents. Therefore, this project explored the value of thecompletely non-invasive rVE-ASL technique in accurately evaluating the cerebral collateral circulation. Our results indicated that the rVE-ASL findings were consistent with DSA/CTA findings in evaluating the cerebral collateral circulation. The rVE-ASL may partially substitute DSA and avoid the invasive procedure in clinical practice. In addition, this study showed that the rVE-ASL score were negatively correlated with mRS, indicating poorer collateral flows evaluated by rVE-ASL were associated with worse outcomes, because the cerebral collateral might be not good enough to provide adequate cerebral blood flow to recover the ischemic tissue.Conclusion
As a completely non-invasive technique, rVE-ASL could be a potential alternative tool to DSA for the assessment of the cerebral collateral circulation in patients with ischemic stroke. Given the association of poor collateral flow with poor outcome, fast and reliable assessment of collateral flow using rVE-ASL may assist in establishing appropriate treatment strategy and improving the clinical outcomes of patents with ischemic stroke.Acknowledgements
This research was supported by the National Key R&D Program of China (2017YFE0103600), National Natural Science Foundation of China (81720108021, 81601466), and Zhongyuan Thousand Talents Plan Project - Basic Research Leader Talent (ZYQR201810117).References
1. Liping Liu, Jing Ding, Xinyi Leng, et al. The Chinese guidelines for the evaluation and management of cerebral collateral circulation in ischemic stroke. Zhonghua Nei Ke Za Zhi. 2017;56(6):460-471.
2. Wong EC, Guo J. Blind detection of vascular sources and territories using random vessel encoded arterial spin labeling. MAGMA. 2012;25(2):95-101.
3. Yan L, Wang S, Zhuo Y, et al. Unenhanced dynamic MR angiography: high spatial and temporal resolution by using true FISP-based spin tagging with alternating radiofrequency. Radiology. 2010;256(1):270-9.
Figures