1654
New Predict Parameter of Prognosis on Hyperacute Cerebral Infarction Evaluated by Multi-delay pCASL Imaging
Masafumi HARADA1, Takashi ABE1, Moriaki YAMANAKA1, Tomoki MATSUSHITA1, Yasushi TAKAGI2, Yuishin IZUMI3, Marc R Lebel4, and Mitsuharu Miyoshi5
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Neurosurgery, Tokushima University, Tokushima, Japan, 3Department of Neurology, Tokushima University, Tokushima, Japan, 4GE Healthcare, Calgary, AB, Canada, 5GE Healthcare, Hino, Japan
1Department of Radiology, Tokushima University, Tokushima, Japan, 2Department of Neurosurgery, Tokushima University, Tokushima, Japan, 3Department of Neurology, Tokushima University, Tokushima, Japan, 4GE Healthcare, Calgary, AB, Canada, 5GE Healthcare, Hino, Japan
Synopsis
The purpose of this study was to find a prognostic perfusion parameter to predict the enlargement of acute cerebral infarction. The prognostic parameter of the enlargement ratio (ER) was only mean delay transit time (DT) in all perfusion parameters, and the tendency was different depending on the existence of recanalization or not. DT obtained by multi-delay ASL may become a better prognostic index of acute cerebral infarction than the mismatch area between the infarction core and ischemic penumbra.
Abstract
IntroductionTo select acute ischemic patients suitable for intra-vascular thrombectomy, it is commonly considered to be important to evaluate mismatch area between the infarction core and ischemic penumbra. However, it has not been known whether the quantitative parameters of the ischemic lesion by the initial perfusion study are useful to predict the final infarction size or not. In this study, we compared the size of mismatch area between the infarction core and ischemic penumbra with multiple perfusion parameters observed by multi-delay pseud-continuous arterial spin labeling (pCASL) imaging. The purpose of this study was to find a prognostic perfusion parameter to predict the enlargement of acute cerebral infarction.
Method
Our subjects were 25 cases diagnosed as acute cerebral infarction in our stroke center from September 2017 until December 2018, and conducted by pCASL imaging.. The instrument of MRI was Discovery 750 (3T, GE, USA) with a standard 8-channel headcoil. Subjects was conducted by diffusion-weighted, T2*-weighted, FLAIR images and MRA as the routine protocol. In addition, all of subjects were conducted by multi-delay ASL for the clinical requirement. The time of MRI study from the onset was 0.6 to 20 hours (mean 6hours, <4.5 hours 16 cases). Twelve cases were received with conservative treatment. Three cases were treated by i.v. rtPA and 10 cases received intravascular thrombectomy. We evaluate the max and mean cerebral blood flow (CBF) and delay time (DT) at core and penumbra of infarction. And the sizes of infarction core and surrounding ischemic area as ischemic penumbra at the initial examination were also measured, The final infarction size was measured in the follow-up examination later than one week, and enlargement ratio of infarction (ER) were calculated.
Result
All subjects were divided by the non-recanalization group (18 cases) and the recanalization group (7 cases). In the no-recanalization group, ER and mean DT at penumbra are inversely correlated (r=-0.50). In recanalization group, infarct ER and mean DT at penumbra are positively correlated (r=0.79). There was no significant correlation between mismatch size between infarction core and ischemic penumbra. Furthermore, the other perfusion parameters except for mean DT were not correlated with ER.
Conclusion
The prognostic parameter of ER was only mean DT in all perfusion parameters, and the tendency was different depending on the existence of recanalization or not. DT obtained by multi-delay ASL may become a better prognostic index of acute cerebral infarction than the mismatch area between the infarction core and ischemic penumbra.
Acknowledgements
The sequence of multi-delay ASL imaging is provided by GE Healthcare, USA as the research purpose, and this study is approved by the institutional ethical committee of Tokushima University Hosptial.References
1)Multi-phase 3D arterial spin labeling brain MRI in assessing cerebral blood perfusion and arterial transit times in children at 3T. Hu HH, Rusin JA, Peng R, et al. Clin Imaging 2019: doi. 10.1016/j.clinimag.2018.11.001Figures
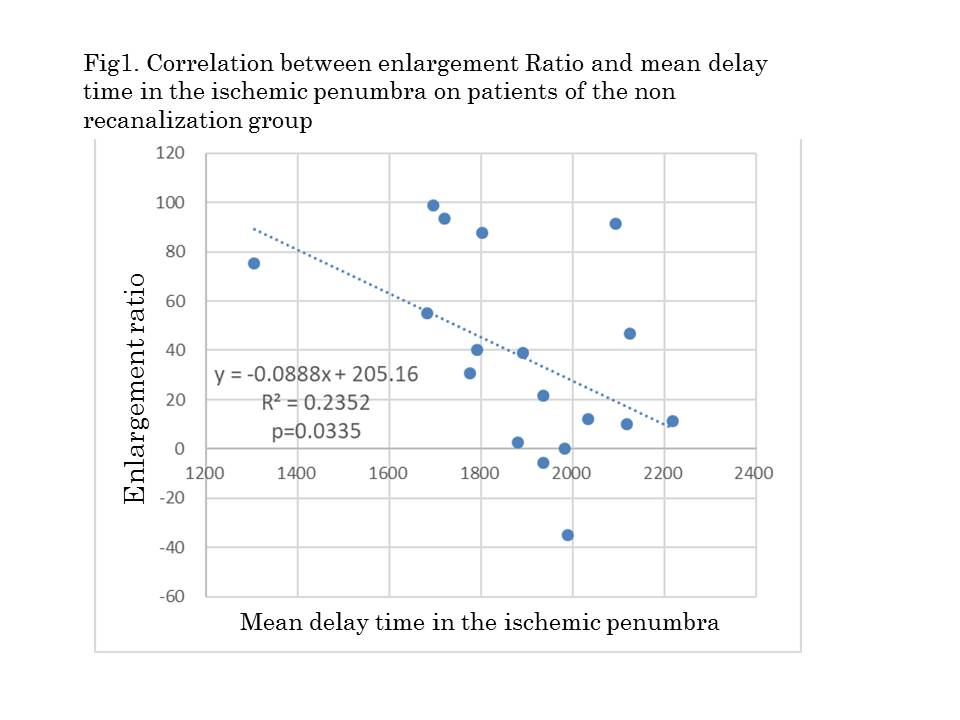
Fig1.
Correlation between enlargement Ratio and mean delay time in the ischemic
penumbra on patients of the non recanalization group
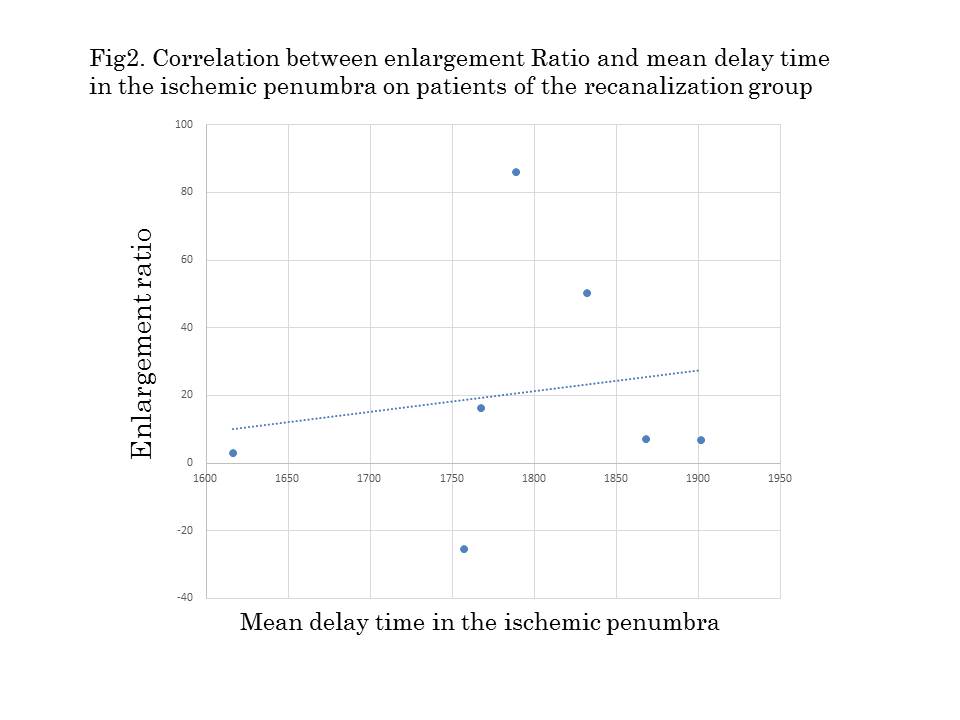
Fig2.
Correlation between enlargement Ratio and mean delay time in the ischemic
penumbra on patients of the recanalization group