1645
Posterior collateral circulation and bypassing perfusion changes after revascularization in Moyamoya disease patients1Radiology, Liaocheng people's hospital, Liaocheng, China, 2Neurosurgery department, Liaocheng people's hospital, Liaocheng, China, 3MR Research China, GE Healthcare, Beijing, China
Synopsis
In patients with Moyamoya disease, posterior collateral circulation plays an important role in defending ischemic syndrome and good revascularization outcome. The association between bypassing perfusion and posterior collateral circulation remains unknown. This study thus used territory arterial spin labeling to evaluate the territory changes of these vessels. Our results showed that good bypassing perfusion is along with the improvement of posterior collateral perfusion territory. This indicates that good operation outcome was not only associated with poor collateral perfusion, but also related with good collateral vessels functioning as blood channels.
Introduction
In patients with Moyamoya disease (MMD), posterior collateral circulation plays an important role in providing blood to ischemic middle cerebral artery (MCA) territory and anterior cerebral artery (ACA) territory.1 As a result, bypassing surgery region, which is always in MCA territory, has collateral vessels from posterior circulation. However, it is unknown that how the posterior collateral circulation change and its relationship with bypassing perfusion. Therefore, in the present study, we used territory arterial spin labeling (T-ASL) technique to evaluate posterior collateral circulation and bypassing perfusion in order to find the impact of collateral circulation on bypassing perfusion.Materials and Methods
16 pre-operative patients (mean age: 44.5±9.7y) diagnosed with Moyamoya disease were recruited for this study.T-ASL images were acquired before and 1-3 months after artery bypassing surgery at a 3.0T whole body system (MR 750W, GE) equipped with an eight-channel head coil. T-ASL imaging was based on a pseudo-continuous arterial spin labeling technique, and was acquired using a super-selective scheme. The pre-and postoperative T-ASL scheme included the bilateral external carotid artery and basilar artery. The scan parameters applied in T-ASL measurement were listed as follows: labeling duration 1450ms, and post labeling delay 2025ms, 3D stack of spiral fast spin echo acquisition with 6 arms, 3 NEX, field of view 200mm×200mm, slice thickness 4.0mm, TR 4762ms, TE10.6ms.
Two neuroradiologists (Shi and Luan) with 8 and 12 years experience in neuroradiology separately evaluated the T-ASL images using a 3-point grading scale describing the intensity of the collateral circulation and bypassing perfusion. As defined in this scale, 0-point represents no collateral or bypassing perfusion visible; 1-point: mild to moderate collateral or bypassing flow; 2-point: robust flow.
In addition, vessel-specific cerebral blood flow (CBF) maps were respectively obtained by analyzing T-ASL data with a vendor-provided software on GE ADW 4.6 workstation. Regional CBF values of cortical tissues were determined in 8 perfusion territories (i.e., 2 anterior and 6 middle sub-regions) per hemisphere corresponding to 2 slice locations of Alberta Stroke Programme Early Computed Tomography Score (ASPECTS).
Results
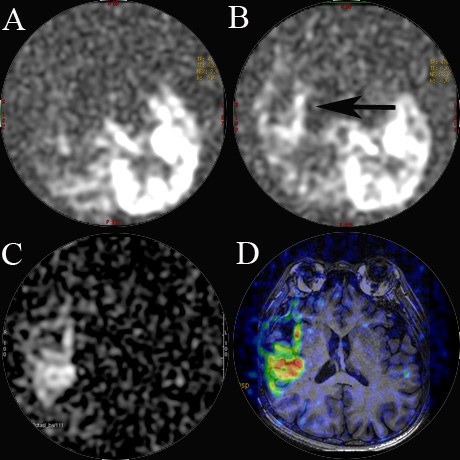
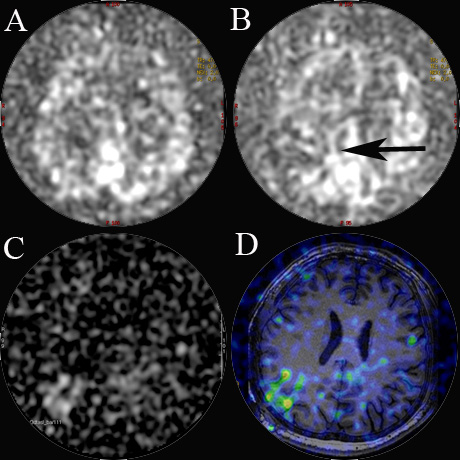
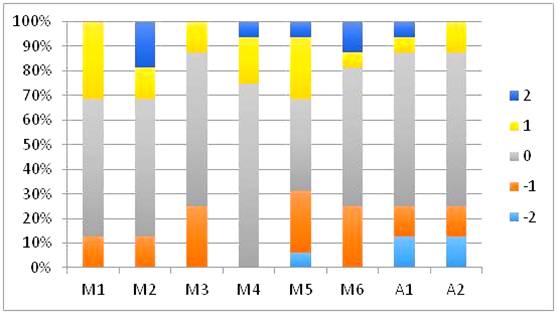
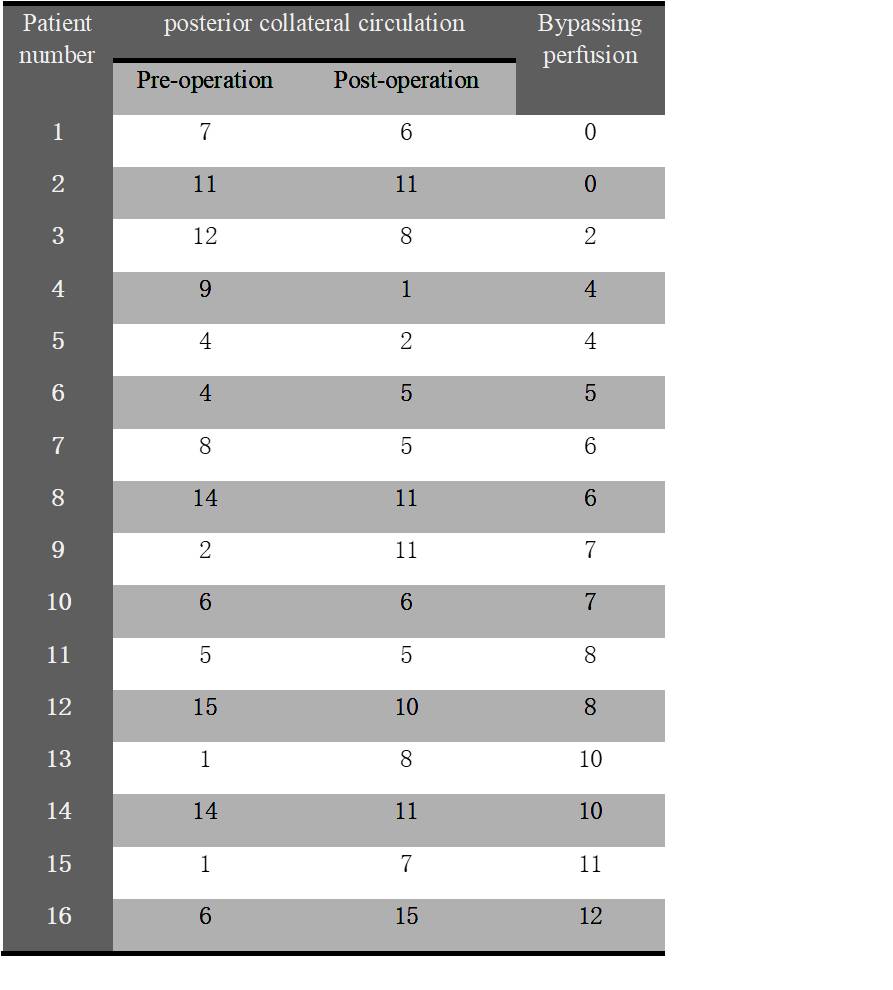
In total, 128 territories of 16 patients were taken into account. In good bypassing perfusion cases (score ≥8 points), the posterior collateral circulation territories were always improved (Figure 1) , whereas in poor bypassing perfusion ones (score <5 points), the blood supply of posterior collateral circulation decreased (Figure 2). The total scores of posterior collateral circulation and bypassing perfusion were showed for each patient in Table 1. The T-ASL score changes of separated regions were showed in Figure 3. M1, M2, M4 and M5 regions showed increased collateral perfusion in more than 25% patients (i.e., 4 patients), and M3, M5, M6, A1 and A2 regions showed decreased collateral perfusion in more than 25% patients (i.e., 4 patients).Discussion and Conclusion
Worse collateral circulation has been demonstrated with a strong demand for blood flow in MMD patients. A better angiographic outcome is expected. However, patients with poor collateral circulation have high rates of reoccurred stroke. 2 As the result of perfusion reconstruction, the recipient vessels are most likely located in posterior collateral perfusion territories. We hypothesized the bypassing perfusion had an association with collateral vessels, and it can replace the collateral perfusion or have an overlapping perfusion territory. T-ASL technique has been reported to be able to provide valuable information in the perfusion changes of major cerebral arteries. 3 This technique is thus expected to evaluate collateral and bypassing perfusion qualitatively and quantitatively.In the current study, significant bypassing perfusion is accompanied by increased territory of posterior collateral perfusion, presenting overlapping perfusion and maybe bypassing perfusion using the existed collateral vessels. Meanwhile, poor bypassing perfusion is along with a decrease of posterior collateral perfusion territory, indicating that bypassing perfusion might build a new blood channel. T-ASL score changes in separated regions showed the increased perfusion territory which is always near the surgical region (i.e., M1, M2, M4, and M5), and decreased perfusion territory being always far from the region of surgery (i.e., A1, A2, M3 and M6). Therefore, bypassing artery provides more blood flow in adjacent brain tissues than removed tissues.
In conclusion, evaluating posterior collateral circulation with T-ASL can predict bypassing perfusion after by-pass surgery, and it is useful to choose the appropriate surgery time for MMD patients.
Keywords
territory arterial spin labeling; Moyamoya disease; revascularization; collateral circulationAcknowledgements
I would like to express my gratitude to all those who have helped me during the writing of this thesis. I gratefully acknowledge the heip of Miss Xiaotong Yang and Mr Wenqi Gao. I do appreciate the help to measure the data and the suggestion of this thesis.References
1. Yamamoto, S., S. Hori, D. Kashiwazaki, et al., Longitudinal anterior-to-posterior shift of collateral channels in patients with moyamoya disease: an implication for its hemorrhagic onset. J Neurosurg, 2018. 130(3): p. 884-890.
2.Liu, Z.W., C. Han, F. Zhao, et al., Collateral Circulation in Moyamoya Disease. Stroke, 2019: p. STROKEAHA119024487.
3. Yuan, J., J. Qu, D. Zhang, et al., Cerebral Perfusion Territory Changes After Direct Revascularization Surgery in Moyamoya Disease: A Territory Arterial Spin Labeling Study. World Neurosurg, 2019. 122: p. e1128-e1136.
Figures